Received: November 20, 2013
Accepted: November 24, 2013
Meditter J Hematol Infect Dis 2014, 6(1): e2014006, DOI 10.4084/MJHID.2014.006
This article is available on PDF format at:

Maria Dimou and Panagiotis Panayiotidis
1st
Department of Propaedeutic Medicine, Division of Hematology, University
of Athens, Greece.
|
This
is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract The
use of interferon-α
(INF) in chronic myeloid leukemia, when it
started in the 80s, was considered as a breakthrough in the therapy of
this disease; INF administered alone or in combination with
aracytin was the standard choice for treatment for Chronic
Myeloid Leukemia (CML) patients unfit for bone marrow
transplantation. With the appearance of the first Tyrosine Kinase
Inhibitor (TKI) (imatinib) and based on the results of the pivotal IRIS
trial, imatinib monotherapy was the new treatment of choice for CML,
according to the ELN recommendations. The possibility of combining INF
with imatinib, for obtaining better therapeutic responses in CML
patients has been already tested and reported. The current challenge is
the combined use of second generation TKIs with pegylated –IFN, in
order to minimize failures to therapy and increase the number of CML
patients with deep molecular responses, who may be able to discontinue
lifelong treatment.
|
Introduction
The
beginning of the use of INF as treatment for CML started at 1983 after
a report by Talpaz et al that leukocyte IFN induced cytoreduction in
CML.[1] Other studies confirmed the
effect of IFN in CML.[2,3,5]
Complete hematologic responses were observed in 80% of CML patients
treated with IFN and in 7-10% of them complete cytogenetic responses
(CCyR) were obtained. CML patients in CCyR under IFN-a treatment have
an 80% chance of 10 years survival.[6,7]
Since there was a clear
benefit in the survival of CML patients treated with IFN compared to
bulsufan or hydroxyurea, IFN became the standard of CML therapy in the
90s and early response after 3 months of therapy was associated with
good outcome.[8] The major issues
raised during that time were
the right dose of IFN-α used and the issue of
combining
IFN with other drugs, e.g. busulfan, hydroxyurea, aracytin.[2-5]
Most studies were performed with high dose of IFN-α, at 5MU/m2/day
and side effects, mainly flu-like symptoms, fatigue, hematologic
toxicity, weight loss, neurotoxicity and depression and cardiotoxicity.
Dose reductions in IFN-α were frequent both in clinical trials and the
everyday clinical practice. In a study comparing high dose IFN versus
low dose (3MU/day/5 das/week) no difference is responses was observed.
Overall survival after 5 years was 50% in the low dose arm versus 49%
in the high dose IFN arm. Complete cytogenetic response was 9% in the
low dose arm and 7% in the high dose IFN arm.[9]
Mechanism of Action of IFN–α in CML
CML progenitor stem cells are deficient in adhering to bone marrow
stromal cells, when compared to normal hematopoietic stem cells.[10]
This was considered to contribute to the pathogenesis of CML, since it
was suggested that circulating CML stem cells, due to their failure to
adhere to bone marrow, could contribute to leukocytosis and
extra-medullary hemopoiesis e.g. splenomegaly.
A minority of CML patients treated with a-IFN obtained CCyR, and some
have discontinued treatment. In a study by Mahon et al. IFNα treated
CML patients who were in CCyR or bcr-abl negativity, discontinued IFN
and 8 patients lost CCyR after 3-33 months.[11]
Seven patients that
were in CCyR>24 months and were bcr-abl negative before
discontinuation did not relapse (median time of observation 36 months).
The results of the pivotal IRIS trial documented the superiority of
imatinib compared to the combination of IFN +Aracytine in the treatment
of newly diagnosed patients with CML in chronic phase.[12]
In 2013 the
TKI inhibitors imatinib, nilotinib and dasatinib are approved as first
line therapy in CML,[13,14] while
bosutinib and ponatinib are approved
for use as second/third line therapy in CML.[15,16]
The mode of action of TKIs is obviously, totally different from that of
IFN and the issue of combining these drugs for the treatment of CML was
soon raised by different groups. The basis for these trials was to have
better response rates and to obtain deeper, sustained molecular
responses. Although deep molecular responses (MR4, MR4.5) may not have
an impact on patient survival, they may offer a higher probability of
successful treatment discontinuation of TKIs.
However, all TKIs examined so far, have failed to eliminate the CD34+
CD38- CML stem cells.[17,18] In
contrast to mature CML sells, survival
of CML stem cells is not dependent on bcr-abl activity and various
other pathways participate in CML cells survival; cellular interactions
between CML stem cells and bone marrow stroma, activation of several
pathways (Wnt, Hedgehog signaling, autophagy, etc).[19-22]
Published Trials of TKIs plus IFN in CML
Published Trials of
TKIs plus IFN in CML
In a study by the CML Italian group, 76 early phase CML patients were
treated with 400 mg imatinib in combination with 50 or 100 or 150
μg/week of pegylated –IFN. The median administered dose of peg-IFN was
32-36 μg/week and 45 of 76 patients (59%) discontinued peg-IFN during
the first year of treatment.[23]
In the French SPIRIT trial,[24]
636 patients with untreated chronic
phase CML were randomized to imatinib 400mg, imatinib 600mg, imatinib
400mg plus peg IFN 90μg/week, and imatinib 400mg plus cytarabine. The
dose of cytarabine was 20mg/m2
on
days 15-28 of a 28 days cycle. During the trial, the arm of imatinib
600 mg/day and the imatinib plus aracytin arm was omitted due to
toxicity and the superior results of imatinib plus peg-IFN. The dose of
peg-IFN after the first year of the study was reduced to 45μg/week
which was better tolerated by the patients. In the first year of the
trial, 45% of patients randomized to the peg-IFN arm discontinue
treatment. The major side effects in this group of patients were an
increase in hematological toxicity, skin rash and asthenia, compared to
the group that received imatinib alone. The median dose of peg-IFN
delivered in the first year of the study was 54μg/week. No difference
in the rate of cytogenetic response after 12 months of therapy was
noted between the four arms of the study. In patients who managed to
receive peg-IFN more than 12 months, 82% had MMR and 49% had MR4 after
two years compared to 43% and 21% respectively in the imatinib 400 arm.
Patients who manage to receive IFN for less than 4 months had
significantly inferior results. The results of this study demonstrated
that the most tolerated dose of pegylated IFN is around 45μg/m2 and the
combination with imatinib results in faster and deeper molecular
responses.
The rate of responses in the Imatinib-peg-IFN arm was comparable to the
responses obtained with the second generation inhibitors nilotinib and
dasatinib.[15,16]
In the German CML IV randomized study,[25]
1104 newly diagnosed CML
patients in chronic phase were randomized to receive imatinib 800mg/d
(n=338), imatinib 400mg/d (n=325), or imatinib 400mg/d plus interferon
alfa (IFN- α; n=351). Primary endpoint of the study was MMR at 12
months.
MMR rates were similar between the imatinib 400 mg and the arm of
imatinib 400+IFN-α (44% vs 46%). The IFN-α used in the study
was
the classical recombinant IFN –a at a schedule of 3 million units x 3
times weekly s.c. It is possible that the IFN-α formulation and e.g.
pegylated versus classical recombinant may and dosage of IFN used may
be responsible for the different therapeutic results between the CML IV
and the SPIRIT trial.
In another phase II study,[26] the
Nordic group randomized 112 chronic
phase CML patients with low or intermediate risk who were in complete
hematologic remission after therapy with 400mg imatinib to a)
continuation with imatinib alone b) receive imatinib plus 50μg
pegylated IFNa/week; 34 of the 56 patients in the combination arm
discontinued peg-IFNα and the dose of peg-IFN was reduced to 30μg/week.
In accordance with the results obtained in the SPIRIT trial, the MMR
rate at 12 months was significantly higher in the imatinib plus
Peg–IFN-α arm (82%) compared with the imatinib monotherapy
arm
(54%).
In a trial by the MD Anderson group, 94 early phase CML patients were
randomized in two arms a) 800mg of imatinib and b) imatinib 800mg plus
0,5μg/kg peg-IFN/week and GM-CSF 125mcg/m2
three times per week subcutaneously. No difference in MMR at 12 months
or at any other time point during the study was observed. It should be
noted, however, that peg-IFN-α was discontinued in all patients due to
side effects or other reasons.[27]
IFN-α has been recently reported to induce proliferation of
hematopoietic stem cells in mice.[28]
Induction of CML stem cells to
exit G0 and entry into cell cycle may render them susceptible to TKIs
and produce the superior results when the two agents are combined for
the treatment of CML patients. CML stem cells have been shown to be
resistant to the administration of the second generation inhibitors
dasatinib and nilotinib.[18,19]
Concomitant administration of IFN-α may
increase the proportion of CML patients achieving deep molecular
responses that may lead to treatment discontinuation.
A number of clinical trials are currently exploring the combination of
IFN-α with TKIS in the treatment of CML (Table 1).
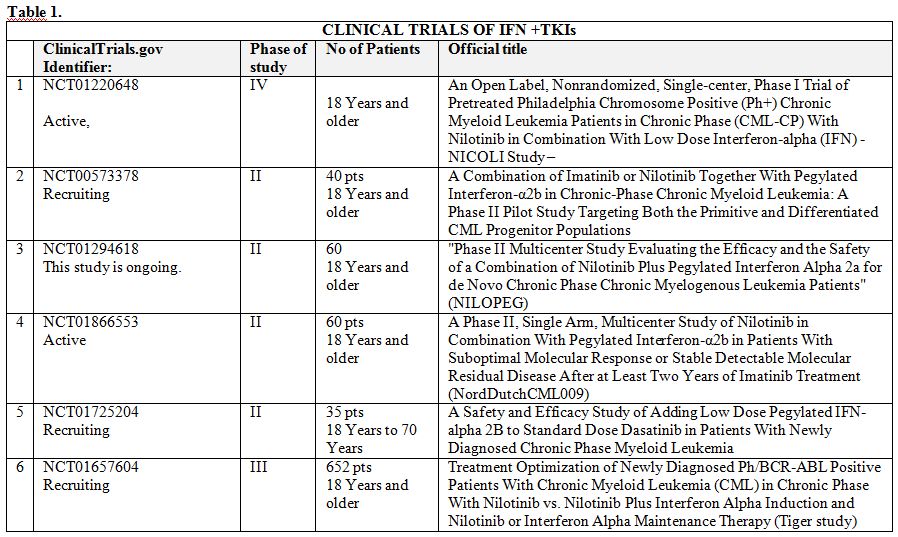 | Table 1. |
In trial No 1
(NICOLI), the maximum tolerated dose of peg-IFN-α in CML patients
receiving nilotinib will be determined.
In trial No 2, the aim is to investigate whether patients with
chronic-phase chronic myeloid leukemia who have achieved a CCyR) on
imatinib or nilotinib can then be treated with a combination of the
tyrosine kinase inhibitor and peg-IFN-α for 2 years. Subsequently these
patients will have their therapy discontinued. Relapse-free survival
(RFS) rate 1 year after discontinuation of the TKI and IFN will be the
main objective of the study.
Forty CML patients will participate in this study. The planned dose for
peg-IFN-α, is 150μg s.c./week, and many side effects and drug
discontinuations are expected.
In the trial No 3, (NILOPEG), 60 chronic phase CML patients will
receive nilotinib 300mg twice a day + Pegylated interferon 2a, 45μg
weekly. Peg-IFN will start after 2-12 months according to investigator
choice. Primary end point is the “CMR” rate at 12 months.
In the trial No 4, by the Nordic group, the purpose will be to assess
the effect of switching CML patients, who have been treated with
imatinib ≥ 2 years and who have stable detectable molecular residual
disease between 0.01-1.0 percent (IS), to a combination of Nilotinib
and PegIFN-α, in terms of the proportion of patients who achieve
confirmed MR4.0. Patients will start therapy with 300mg nilotinib BID
for 3 months, and then Peg IFN will be added at 25μg/week s.c. In the
absence of toxicities, the dose will increase to 40μg/week s.c. The
estimated enrollment is 60 patients.
In the study No 5, by the Nordic group, 35 newly diagnosed CML patients
will receive dasatinib 100mg/day for 3 months, and then 15 μg/week
Peg-IFN. If no significant toxicities emerge, peg-IFN-α dose will
escalate up to 25μg/week for the next 9 months. Primary end point
is the rate of MMR after 1 year.
The study No 6, (TIGER) by the German group, 652 chronic phase CML
patients will be randomized to:
a) nilotinib 300mg bid plus Peg-IFN-α 30μg/week s.c. After confirmed
MMR and at least 24 months therapy, nilotinib will be discontinued.
When MR4 for more than a year, discontinuation of peg-IFN-α.
b) nilotinib 300mg bid for more than 3 years. If MR4 more than a year,
discontinuation
The aim of the trial is to improve treatment strategies in CML by
improving induction therapy and deescalating maintenance therapy, using
low-dose IFN as inducer of immune surveillance.
Primary end point will be the rate of MMR after 18 months and
feasibility to discontinue therapy when patients have in stable MR4
response for more than a year.
From the current trials incorporating IFN in the therapy of CML, it is
obvious that the pegylated form of IFN is universally used, at doses
much lower than the ones used in previous studies. The question is if
these lower peg-IFN doses with acceptable toxicities will retain their
activity against CML. The possibility of effective targeting the CML
stem cells via the combination of TKIs and peg-IFN remains an open
question. If this combination will succeed in inducing higher rates of
treatment discontinuations then IFN-α (the pegylated form) will
reappear officially in the treatment of CML patients.
References

[TOP]