Received: August 16, 2013
Accepted: November 28, 2013
Meditter J Hematol Infect Dis 2014, 6(1): e2014008, DOI 10.4084/MJHID.2014.008
This article is available on PDF format at:

Poorvi Chordia and Pranatharthi Chandrasekar
Division of Infectious Diseases,
Department of Internal Medicine. Wayne State University, Detroit, MI,
USA.
|
This
is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract Reactivation
of human herpes virus-6 (HHV-6) after stem cell transplantation occurs
frequently. It is associated with clinical manifestations varying from
nonspecific symptoms such as fevers or rash, to severe life threatening
complications including post-transplantation limbic encephalitis. We
report a case of severe HHV-6 encephalitis with viremia in an
allogeneic peripheral stem cell transplant recipient who presented with
status epilepticus unresponsive to antiepileptic therapy. With
intravenous ganciclovir and supportive care, the patient’s condition
improved. Awareness of HHV-6 infection in stem cell transplant
recipients may help with early diagnosis and improved outcome.
|
Introduction
HHV-6
reactivation has been increasingly recognized in stem cell transplant
recipients.[1] Primary infection
with HHV-6 usually occurs during infancy
with reactivation in 40-60% patients after stem cell transplantation.[1]
Clinical manifestations of HHV-6 reactivation in stem cell
transplantation recipients are variable, including fever, rash,
diarrhea, pneumonia, hepatitis, encephalitis, delayed platelet
recovery, graft versus host disease (GVHD), and increased mortality.[2]
Median onset of symptoms is about three weeks after stem cell
transplant, and often coincides with engraftment.[3]
Our case involves a
patient with myelodysplastic syndrome who underwent an allogeneic stem
cell transplantation following which he developed severe HHV-6
encephalitis causing status epilepticus.
Case Report
A 68-year-old man with myelodysplastic syndrome (MDS)
secondary to treatment with capecitabine-oxaliplatin for colon cancer,
underwent a matched, unrelated donor peripheral stem cell
transplantation. Conditioning regimen comprised of fludarabine,
busulfan and total body irradiation. For GVHD prophylaxis, the patient
received tacrolimus, mycophenolate and thymoglobulin. Stem cell donor
was Cytomegalovirus (CMV) seronegative, while the patient was CMV
seronegative and Herpes Simplex Virus (HSV) seropositive.
On day +4 after transplantation, cefepime was started for fever during
neutropenia. On day +8, the patient developed a generalized
non-blanching erythematous maculopapular rash and loose stools.
Engraftment syndrome was suspected, and a short course of intravenous
steroid therapy was started. The patient engrafted on day +14.
On day +18, the patient developed confusion and anterograde amnesia.
Over the next three days, he developed increasing lethargy and multiple
generalized tonic-clonic seizures. A CT scan of the head showed no
abnormalities. On day +21, the patient developed status epilepticus,
unresponsive to antiepileptic medications. Due to declining mental
status and to protect his airway, he was endotracheally intubated. For
treatment of seizures, therapy with levetiracetam was started.
Video EEG demonstrated bilateral central-frontal slow epileptiform
waves with clinical manifestations of right arm jerking that spread to
bilateral lower extremities. Cerebrospinal fluid (CSF) analysis showed
normal levels of protein and glucose, and no pleocytosis. CSF bacterial
cultures as well as CSF polymerase chain reaction (PCR) for Herpes
Simplex Virus, West Nile Virus, Epstein Barr Virus and Varicella Zoster
Virus were negative. Serum tacrolimus level was within normal limits.
MRI brain showed increased symmetric T2/FLAIR signal in medial temporal
lobes, hippocampi, medial thalamus, and insular regions (Figure1).
Plasma and CSF HHV-6 DNA PCR were 57,000 copies/ml and 81,796
copies/ml, respectively. Based on clinical and characteristic
radiographic findings along with HHV-6 PCR, the diagnosis of HHV-6
encephalitis was made.
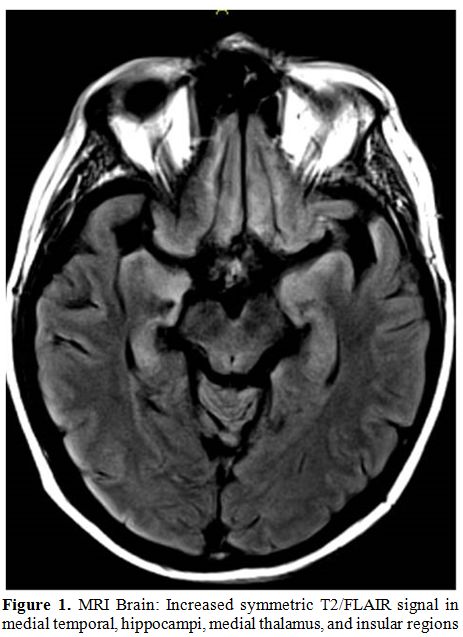 | Figure 1. MRI Brain: Increased symmetric T2/FLAIR signal in medial temporal, hippocampi, medial thalamus, and insular regions. |
The patient was treated in the intensive care unit with ventilator support, anticonvulsants, intravenous ganciclovir (5mg/kg twice daily). Gradually, his seizures subsided and he was subsequently extubated. He continued to have progressive improvement, although mild anterograde amnesia was observed even after ten days of antiviral treatment. Repeat plasma HHV-6 DNA PCR at two weeks was negative, and intravenous ganciclovir was discontinued after a total treatment of 3 weeks.
Discussion
HHV-6 encephalitis is a sporadic complication of HHV-6
reactivation in stem cell transplant recipients. Our patient had early
features of HHV-6 reactivation as evidenced by fevers and rash on day
+8 after transplantation. His condition progressed to encephalitis with
symptoms of confusion and anterograde amnesia on day +18, and status
epilepticus on day +21. The severity of our patient’s neurologic
manifestations could be explained by the long clinical evolution. In a
study by Fujimaki et al., 9 of 11 patients with HHV-6 encephalitis had
herald symptoms of fevers and rash prior to the onset of neurologic
signs and symptoms.[4] Prodromal
symptoms of fevers and rash in this
setting should alert the physician of possible HHV-6 reactivation.
Similar to our patient, analysis of CSF in HHV-6 encephalitis is
usually unremarkable. Lack of pleocytosis and normal levels of protein
and glucose are common.[5] The
presence of a positive CSF HHV-6 PCR, with
suggestive clinical findings clinches the diagnosis. The patient also
had characteristic MRI findings of limbic encephalitis which is typical
for HHV-6 encephalitis.[6]
As with the cytomegalovirus PCR, the international standardization of
HHV-6 PCR quantification is urgently needed. There are no data
correlating quantification of PCR with severity of symptoms. Our
patient had a “high” viral load in the serum and CSF, perhaps
suggesting severe illness. In a study by Ogata et al., it was found
that plasma HHV-6 DNA ≥10,000 copies/ml correlated with the development
of HHV-6 encephalopathy and offered 100% sensitivity and 64.6%
specificity.[7]
Although it remains uncertain if HHV-6 reactivation after stem cell
transplantation increases mortality, the prognosis associated with
HHV-6 encephalitis remains poor. In one study, 80% patients with HHV-6
encephalitis post-transplantation were disabled because of persistent
neuropsychological problems that included retrograde amnesia and
seizures.[8]
Treatment for HHV-6 encephalitis includes intravenous ganciclovir,
foscarnet or cidofovir. Acyclovir is not active against HHV-6. Due to
poor outcomes secondary to HHV-6 reactivation, the usefulness of
preemptive[9] or prophylactic
therapy[10] needs to be
determined.
Currently, the European Conference on Infections in Leukemia does not
recommend routine prophylaxis with potentially toxic ganciclovir or
foscarnet against HHV-6 reactivation in patients who have undergone
stem cell transplantation.[11]
HHV-6 reactivation after stem cell transplantation is not uncommon, and
can often lead to potentially lethal complications such as limbic
encephalitis. More data are needed to determine the benefits of routine
surveillance and pre-emptive therapy, especially in those patients at
high risk to reactive HHV-6, as seen with cord blood transplant
recipients.
References

[TOP]