Received August 20, 2013
Accepted: November 11, 2013
Meditter J Hematol Infect Dis 2014, 6(1): e2014009, DOI 10.4084/MJHID.2014.009
This article is available on PDF format at:

Ibrahim C. Haznedaroglu, MD
Hacettepe University Medical
School, Department of Hematology, Ankara-Turkey
|
This
is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract The aim of oral
tyrosine kinase inhibitor (TKI) treatment in chronic myeloid leukemia
(CML) is to get ideal hematological, cytogenetic, molecular responses
at the critical time points. The depth of the response obtained with
TKI and the time to achieve this response are both important in
predicting the prognosis in patients with CML. The high efficacy of the
TKI treatment of CML has prompted the need for accurate methods to
monitor response at levels below the landmark of CCyR. Quantification
of BCR-ABL transcripts has proven to be the most sensitive method
available and has shown prognostic impact with regard to
progression-free survival. European LeukemiaNet (ELN) molecular program
harmonized the reporting of results according to the IS (International
harmonization of Scale) in Europe. The aim of this review is to outline
monitoring the response to optimal TKI treatment based on the ELN CML
2013 recommendations from the clinical point of view as a physician.
Careful cytogenetic and molecular monitoring could help to select the
most convenient TKI drug and to optimize TKI treatment. Excessive
monitoring may have an economic cost, but failure to optimize TKI
treatment may result in CML disease acceleration and death.
|
Introduction
Current
standard therapy for chronic phase (CP-) Ph+ Chronic myeloid leukemia
(CML) is the chronic oral administration of tyrosine kinase inhibitor
(TKI) drug.[1]
European LeukemiaNet (ELN) 2013 recommendations provided
clear, practical suggestions for the physicians dealing with CML
management, based on the best available evidence about the TKI drugs,
without disregarding clinical realities and expectations.[1] The aim of
this review is to outline monitoring the response to optimal TKI
treatment based on the ELN CML 2013 recommendations from the clinical
point of view as a physician.
Based on the true ELN philosophy, the cost of monitoring is much lower
than the cost of the TKI drugs.
Careful cytogenetic and molecular monitoring could help selecting the
most convenient TKI drug and to optimize TKI treatment.[1]
Excessive
monitoring may have an economical cost, but failure to optimize TKI
treatment may result in CML disease acceleration and death.
Insufficient diagnostic/therapeutic clinical intervention during the
management of CML disease course with TKI drugs can cause accelerated
phase (AP) or blastic crisis (BC). The survival after the progression
into AP/BC is still significantly shorter even in the powerful TKI era.[2]
Diagnostic Tools and Surrogate Markers for the Monitoring the Response to TKI in CML
Ph+ CML disease burden should be monitored during the TKI treatment.[3]
Hematologic response (HR) is measured by the evaluation of complete
blood counts (CBC), white blood cell differential (WBC), and assessment
of the spleen size. The definition of the hematologic, cytogenetic and
molecular responses is depicted in Table
1. Cytogenetic response (CyR)
is detected via the chromosome banding analysis of the bone marrow cell
metaphases. The principle of the molecular response (MR) depends upon
the measurement of the BCR-ABL transcript levels relative to a control
gene. After one year of TKI treatment in CML, complete (C) HR can be
obtained in about 98%, CCyR in 57-88%, and major (M)MR in 18-58% of the
patients.[1,4-6]
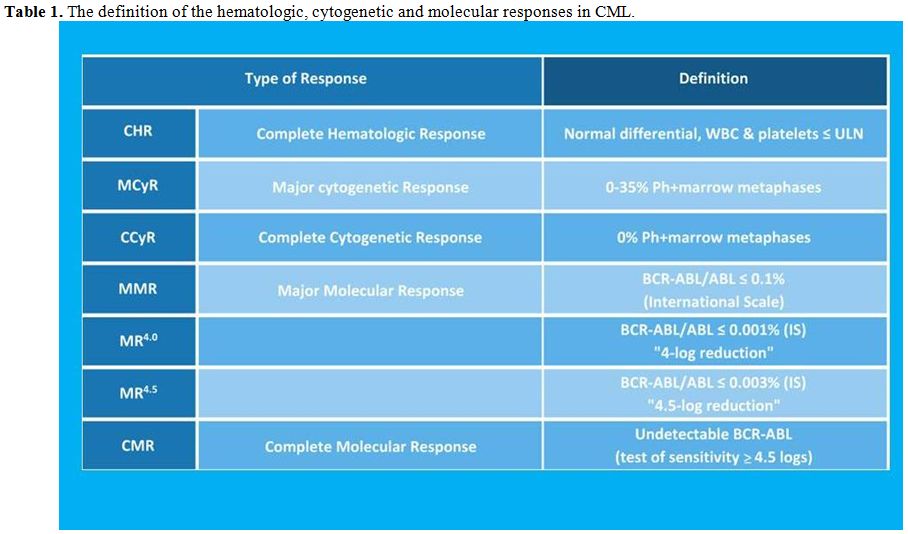 | Table 1. The definition of the hematologic, cytogenetic and molecular responses in CML. |
Optimal Cytogenetic and Molecular Monitoring in CML Based on ELN 2013 Recommendations
The responses to TKI in CML can be assessed either with molecular tests
alone or with cytogenetic tests alone, depending on the local
laboratory facilities.[1,7-14] However, both cytogenetic and
molecular
tests are recommended, until a CCyR and an MMR are achieved. Then
quantitative molecular tests from the peripheral blood samples alone
may be sufficient.[1]
The molecular ELN CML 20131 recommendations are; quantitative RT-PCR of
blood cells every 3 months, until the MMR is achieved and confirmed,
and then RT-PCR every 3 to 6 months. The molecular results must be
expressed by the IS (International harmonization of Scale).[1]
The cytogenetic ELN CML 20131 recommendations are; chromosome banding
analysis (CBA) of marrow cell metaphases at 3 and 6 months, then every
6 months until the CCyR is achieved. CBA of the bone marrow cells
should be repeated at least every 12 months only if the molecular
response cannot be measured. FISH of the blood cells can substitute for
CBA only if bone marrow cells cannot be obtained, and only for the
definition of CCyR.[1]
Mutational analysis is recommended in case of progression, failure and
warning based on the ELN CML 20131,[15]
recommendations. In case of
failure, warning, and of development of myelodysplastic features
(unexpected leukopenia, thrombocytopenia, or anemia), CBA of the bone
marrow cell metaphases is recommended.[1]
Monitoring TKI Response at the Critical Time Points in CML Based on ELN 2013 Recommendations
At the diagnosis of CML; CBA of the marrow cell metaphases, FISH in
case of Ph negativity, to identify variant, cryptic translocations and
qualitative PCR (identification of transcript type) are required.[1]
During the treatment of CML; Quantitative, real-time PCR (RQ-PCR) for
the determination of BCR/ABL1 transcripts level on the international
scale, to be performed every 3 months until an MMR has been achieved,
then every 3 to 6 months and/or CBA of the bone marrow cell metaphases
(at least 20 banded metaphases), to be performed at 3, 6 and 12 months
until a CCyR has been achieved, then every 12 months. Once a CCyR is
achieved, FISH on blood cells can be used. If an adequate molecular
monitoring can be assured, cytogenetics can be spared.[1]
In the case of failure or progression of CML; RQ-PCR, mutational
analysis, and CBA of the bone marrow cell metaphases and
immunophenotyping in blastic phase are required.
When a ‘Warning’ sign appeared during the TKI administration in CML
based on ELN 2013; Molecular and cytogenetic tests to be performed more
frequently. CBA of the bone marrow cell metaphases recommended in case
of myelodysplasia or complex karyotypic abnormalities (CCA)/Ph+ with
chromosome 7 involvement.[1]
Ideal Response Level to the TKI Treatment Detectable During the Long-Term Monitoring in CML
The ideal responses to the TKI treatment detectable during the long-term monitoring of CML are depicted in Table 2. Inability to detect ELN-warnings in a CML patient receiving a given TKI, resulting in drug failure and/or disease progression can cause damage to the patient.[16] Proper therapeutic interventions in case of primary and secondary failures during the TKI treatments are described in the ELN 2013 recommendations.[1]
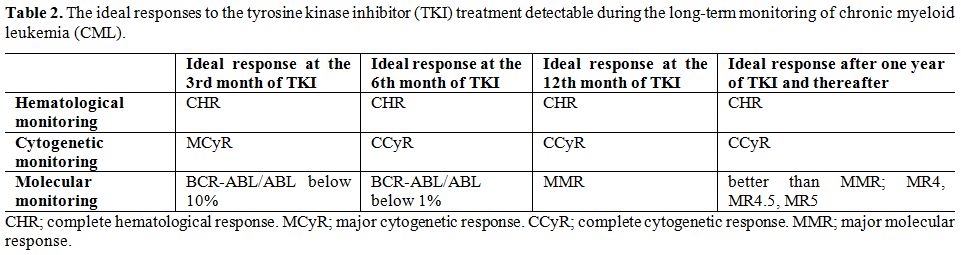 | Table 2. The ideal responses to the tyrosine kinase inhibitor (TKI) treatment detectable during the long-term monitoring of chronic myeloid leukemia (CML). |
Clinical Significance of the Ideal Response Level to the TKI Treatment Detectable During the Long-Term Monitoring in CML
The aim of TKI treatment in CML is to get ideal hematological,
cytogenetic, molecular responses in the critical time-points (at the
3rd
month, at the 6th
month, after one year, and thereafter) as
depicted in Table 1.
The depth of the response obtained with TKI and
time to achieve this response are important for the prediction of
prognosis in the patient with CML.[16]
Clinical significances of the
ideal response level to the TKI treatment detectable during the
long-term monitoring in CML are indicated below.
CHR;
complete hematological response is defined as normal CBC, normal
peripheral blood smear and normal spleen in the physical examination.[17]
CHR is the first station during the TKI treatment and must be obtained
less than 3 months and should be maintained during the long-term
management of CML. CHR can be achieved in about 98% of the patients
with CML in the TKI era. Absence of CHR at any stage during the CML
disease course is a clear sing of disease progression. Proper
therapeutic intervention in the absence of CHR during the TKI
treatments is described in the ELN 2013 recommendations.[1]
CCyR;
complete cytogenetic response is defined as the absence of Ph+
chromosome in the CBA of the bone marrow cells in at least 20 banded
metaphases. CCyR is the golden standard during the TKI treatment and
must be obtained within the first year (ideally at the six months of
TKI regimen) and should be maintained during the long-term management
of CML. CCyR is a significant barrier against the CML disease
progression. CCyR can be achieved in about 57-88% of the patients with
CML in the TKI era. Absence of CCyR after one year of CML disease
course is a great danger for disease progression. Proper therapeutic
intervention in the absence of CCyR during the TKI treatments is
described in the ELN 2013 recommendations.[1]
MMR;
major molecular response is defined as BCR-ABL ≤ 0.1% in the
quantitative RT-PCR of blood cells. MMR is a safe haven during the TKI
treatment and must be obtained within the 18 months (ideally at the
12th
months of TKI regimen) and should be maintained during the
long-term management of CML. MMR is a very significant barrier against
the CML disease progression. MMR can be achieved in about 18-58% of the
patients with CML in the TKI era. Absence of MMR after 18 months of CML
disease course is a danger for disease progression. Proper therapeutic
intervention in the absence of MMR during the TKI treatments is
described in the ELN 2013 recommendations.[1]
EMR;
early molecular response is defined as BCR-ABL/ABL ≤ 10% cut-off
in the quantitative RT-PCR of blood cells.[18,19]
EMR (ideally at the 3rd
month of TKI treatment) can predict long-term prognosis during the TKI
treatment and must be reached within the first 6 months during the
management of CML.[8,16,20]
EMR is a prognostic sign for CML disease
course. EMR can be achieved in about 91% of the patients with CML
receiving nilotinib and 67% receiving imatinib in the ENESTnd trial.[21]
Absence of EMR after 6 months of CML disease course represents an
aggressive disease course in the long-term for instance after 5 years.
Proper therapeutic intervention in the absence of EMR during the TKI
treatments is described in the ELN 2013 recommendations.[1]
TFR (treatment-free remission) is the discontinuation of TKI in the
superior-TKI responder patient with CML. The deeper molecular responses
(MR4, MR4.5, MR5) detected during at least two years of monitoring in
CML are candidates for TFR. MR4 can be achieved by a BCR-ABL expression
< 0.01%, MR4.5 by <0.0032% BCR-ABLIS, and MR5 by
<0.001%
BCR-ABLIS.
Young and low prognostic risk CML patients are candidates of
first line 2nd
generation TKIs with the aim of drug discontinuation in
their future life.[16]
Mutational analyses shall only be performed in patients with suboptimal
responses, warnings, and failures in CML cases subject to the
alterations in the treatment strategies.[1]
Mutations detected during the
TKI therapy may be resulted in drug switches based on the nature of the
mutation. T315I, Y253K, E255K, E255V, F359V, F359C, are the mutations
poorly sensitive to nilotinib; whereas T315I, T315A, F317L, F317C,
V299L are the mutations poorly sensitive to dasatinib. T315I is a
unique mutation making the CML patient irresponsive to all available
TKIs but ponatinib and allografting.[22-29]
Patients with advanced phase (AP/BC) CML are currently treated with the
most powerful TKI[30] available
(dasatinib[31] or ponatinib[32]) and
multi-agent chemotherapy before allografting. Monitoring of those
patients is also problematic. Durable hematological, cytogenetic,
molecular responses are hard to be obtained in the CML patients with
advanced phase (AP/BC) disease. Although durable hematologic,
cytogenetic and molecular responses can be hardly obtained in AP and
particularly in BP patients, the definition of the responses should be
the same as for CP patients. Proper therapeutic interventions in
advanced phase CML are described elsewhere.[1,2]
Practical Problems in the Long-Term Monitoring of TKI Treatment in CML
CHR, early CCyR, faster MMR, and the deeper, durable molecular
responses (MR4, MR4.5, MR5) are the ultimate goals of the TKI-receiving
patients with CML. Critical evaluations of the CML patients to hit
those targets shall be made at the baseline, and at the 3rd month, 6th
month, 12th
month, and thereafter the TKI administration. There are
some practical and technique-related problems during the hematological,
cytogenetic, molecular monitoring of TKI treatment in CML. Clinical
significances of those incidences during the long-term monitoring in
CML are indicated below.
Hydroxyurea treatment, especially in sustained high doses, before the
initiation of TKI regimen, could obscure the evaluation of CHR and
baseline CML disease risk profile of the patient. Before the TKI
decision, the baseline assessments of the de novo CML patient shall
include exact medical diagnosis of CML, basic laboratory evaluation
covering CBC and peripheral blood smear (PBS), bone marrow cytology,
conventional cytogenetics and/or FISH analyses for Ph+ chromosome, and
qualitative molecular analyses for the BCR-ABL.[1]
Tumor load and disease
phase should be defined. Newly diagnosed CP-CML patients should be
stratified based on the Sokal, Euro/Hasford and EUTOS CML prognostic
scoring systems.[33] Hydroxyurea
can affect CBC, PBS, spleen size, bone
marrow cellularity, the quality of metaphases, and essential parameters
of the Sokal, Euro/Hasford and EUTOS CML prognostic scoring systems.
Therefore, baseline CML disease risk profile of the patient shall be
obtained before the hydroxyurea and/or TKI were administered to the
patient.
The estimated ratio of BCR-ABL/ABL is highly technique-dependant. Many
laboratories in the world are not yet qualified for the international
harmonization of scale (IS). Standardization of BCR-ABL quantification
in Europe have been performed by European LeukemiaNet (ELN) and the
European Treatment, and Outcome Study (EUTOS).[34]
The high efficacy of
the TKI treatment of CML has prompted the need for accurate methods to
monitor response at levels below the landmark of CCyR. Quantification
of BCR-ABL transcripts has proven to be the most sensitive method
available and has shown prognostic impact with regard to
progression-free survival. The variations in the methods used to
quantify BCR-ABL made it difficult to compare results between
laboratories. ELN program harmonized the reporting of results according
to the IS in Europe. The ELN recommendations for the propagation of the
IS by national or regional laboratory networks.[34]
The 2012 status of
the BCR-ABL standardization within 64 participating laboratories in 28
countries including the Mediterranean land is depicted in Figure 1.
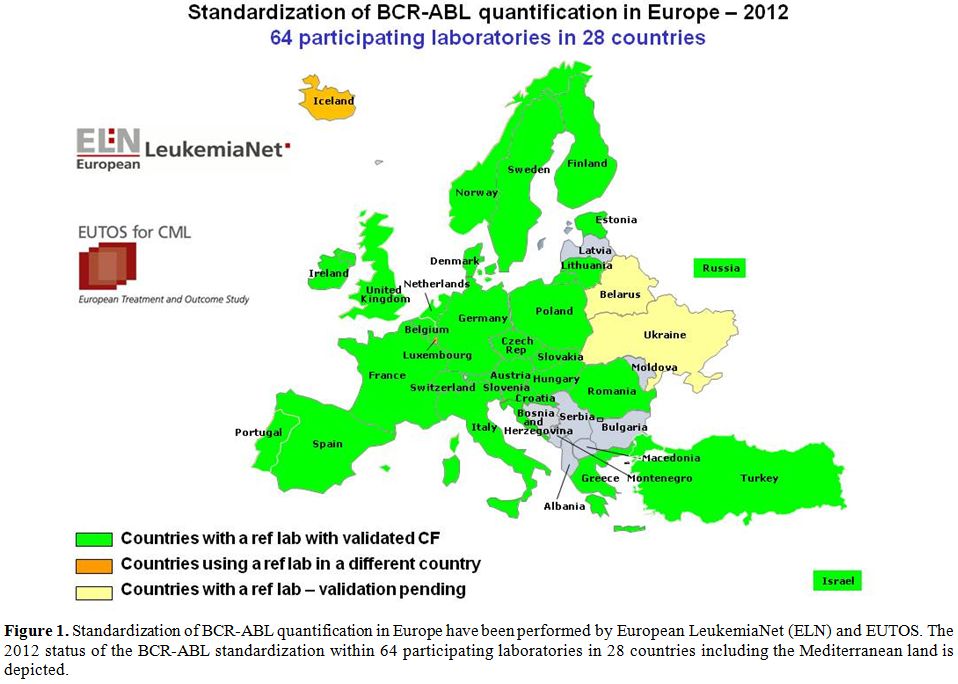 | Figure 1. Standardization of BCR-ABL quantification in Europe have been performed by European LeukemiaNet (ELN) and EUTOS. The 2012 status of the BCR-ABL standardization within 64 participating laboratories in 28 countries including the Mediterranean land is depicted. |
Regarding the EMR,
the challenges for the widespread routine use of the
10% BCR-ABL transcript cut-off at the 3 month of TKI are
present.
High ratio values on IS scale, housekeeping control gene problem,
variations in the samples, delays in the exact molecular assessment
time after TKI and early unexpected variation kinetics of response in
individual CML patients complicate the interpretation of the 10%
BCR-ABL transcript cut-off at the 3rd
month of TKI. Likewise, the tumor
burden at diagnosis, prognostic scoring, gene profile, cytoreduction
before TKI, treatment adherence, and numerous confounding effects may
obscure the real-life decision at the 3rd
month of TKI outside the
clinical trials. Nevertheless, obtaining faster, deeper and durable
molecular responses particularly MMR are essential for the patient with
CML in the TKI era. Proper therapeutic interventions based on the
molecular responses are described in the ELN 2013 recommendations.[1]
The cytogenetic analyses also have technique-dependant problems.
Obtaining the CBA of the bone marrow cell metaphases at 3 and 6 months,
then every 6 months until the CCyR[1]
could not be possible in all cases
of CML under TKI. Invasive nature of the bone marrow aspiration/biopsy
could represent another clinical problem. FISH of the blood cells can
substitute CBA if bone marrow cells cannot be obtained for the
definition of CCyR. The standardization about the sensitivity level of
FISH has improved. Nevertheless, obtaining earlier and stable
cytogenetic responses particularly CCyR are essential for the patient
with CML in the TKI era. Proper therapeutic interventions based on the
cytogenetic responses are described in the ELN 2013 recommendations.[1]
CML treatment may be modelled on the individual disease and patients
characteristics (risk, molecular profile, age, co-morbidities,
aggressive clinical course, etc.). Therefore, the CML monitoring
strategy to detect the response to TKI may also be varied and tailored
on an individual basis. Drug tolerability, patient compliance of TKI,
physician adherence to TKI, and off-target TKI complications should
always be monitored during the CML treatment. Otherwise, late,
off-target complications of TKI (lung toxicity,[35]
cardiac
toxicity,[36,37] metabolic
syndrome,[21] bone toxicity,[38] arterial and
venous occlusive events,[39]
pancreas toxicity,[1] and others)
may limit
the benefits of the given TKI. Proper therapeutic interventions based
on the therapeutic monitoring of the CML patients and TKI drugs are
described in the ELN 2013 recommendations.[1]
Future Perspectives in the Monitoring of TKI Treatment in CML
Novel recent investigations for the de novo CML patients have searched
the validity of gene expression profiling, genetic polymorphisms, next
generation genomics, multi-drug resistance genes (MDR, OCT1),[15] fusion
transcripts and pre-existing BCR-ABL kinase domain mutations. The
cessation of the TKI therapy with the aim of cure,[40]
stem cell
depletion, stem cell exhaustion, immunological control of the disease
will be the future therapeutic tools of CML. The improvements in the
international harmonization of scale about the molecular monitoring
would be very important in the TFR stage of CML with the intention to
cure the disease.
References

[TOP]