Received: March 11, 2014
Accepted: September 4, 2014
Meditterr J Hematol Infect Dis 2014, 6(1): e2014058 doi: 10.4084/MJHID.2014.058
This article is available on PDF format at:

İlker Devrim1, Hüseyin Aktürk1, Nuri Bayram1, Hurşit Apa1, Şener Tulumoğlu2, Fatma Devrim4, Tülin Erdem2, Gamze Gulfidan2,Yüce Ayhan2, İpek Tamsel5, Demet Can3 and Hüdaver Alper5
1 Department of Pediatric Infectious Diseases, Dr. Behçet Uz Children's Hospital, İzmir, Turkey
2 Department of Clinical Microbiology, Dr. Behçet Uz Children's Hospital, İzmir, Turkey
3 Pediatric Allergy and Asthma Unit, Dr. Behçet Uz Children's Hospital, İzmir, Turkey
4 Department of Pediatrics, Dr. Behçet Uz Children's Hospital, İzmir, Turkey
5 Department of Radiology, Ege University, Faculty of Medicine, İzmir, Turkey
| This is an Open Access article distributed under the
terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Background:
Tuberculosis (TB) remains a major global health problem. The childhood
tuberculosis has some unique features different which makes the
diagnosis more complicated. Here we described the epidemiologic,
clinical and microbiologic features of children with extra pulmonary
and pulmonary TB.
Methods: The data of the patients <14 years with active TB were collected and compared in pulmonary (PTB) and extrapulmonary TB (EXPTB) patients. Results: A total of 128 cases was included. Forty-two cases occurred in children were < 5 years of age; 41 cases between 6-10 years and 45 cases > 10 years. PTB was present in 75,0% of the cases, and EXPTB was present in 25% of cases. There was no significant difference between the EXPTB and PTB by means of distribution of age groups (p=0,201). The rate of patients free of constitutional symptoms were significantly higher in EXPTB compared to PTB(p=0,000). There was no significant difference between EXPTB and PTB by means of sources detection(p=0,069). Conclusion: TB is still a major public health problem. EXPTB has an insidious and silent onset without any constitutional symptoms, and both microbiological confirmation and the source by an adult are not frequently found. Moreover, detection of the adult source is mandatory for controlling the TB disease in children |
Introduction
Tuberculosis (TB) remains a major global health problem affecting
millions of people annually. It is the second leading infectious cause
of death following human immunodeficiency virus (HIV) worldwide.[1]
In 2011, 9 million new cases and 1.4 million deaths due to TB were
reported. Despite difficulties for estimation of TB, 500000 new cases
and 64000-deaths among children under 15 years old were expected in
2011.[1] Recent data from Turkey; estimated the
incidence rate of TB as 24 (21–27) / 100000 population including
HIV-POSITIVE population, being the incidence of HIV-TB population only
0.04 (0.04–0.05) / 100000.[2]
TB is still a major health problem for children as well as adults.
Although children constitute 5% of TB population in low-burden
countries, it is reported to be as high as 20-40% in other countries.[3-6]
Turkey has an additional risk for outbreaks of TB comparing to Europe
and US; because of large numbers immigrants from war-zones of Middle
East such as Syria had been travelling across the country.
Tuberculosis in children has unique features, different from adults,
which make the diagnosis more difficult. The symptoms of TB in children
have a broad spectrum changing from non-specific symptoms to severe
clinical presentations. Although pulmonary involvement is frequent, all
organs can be involved.[7,8] Almost every child in
Turkey has Bacillus Calmette–Guérin (BCG) vaccination at least once,
thus the tuberculin skin test (TST) has limited benefit at diagnosis.
Although previous studies suggested whole-blood interferon-gamma
release assays (IGRAs) for confirmation of exposure in TST positive
children, discrimination of latent and active TB disease could not be
done based on this test as the value of the test have not been well
studied in young children and infants;[9,11]
moreover IGRAs are not routinely performed in clinical settings in
Turkey. Thus, the diagnosis and decision to start therapy are based on
clinical suspicion supported by history of exposure, clinical features,
chest radiograph and TST as well as some degree of IGRAs.[12,13]
In this study, we reviewed our experience at pediatric patients with
active TB admitted in a tertiary hospital in a 5-year period in Turkey.
We aimed to compare the epidemic, clinical and microbiological features
of the extra-pulmonary tuberculosis (EPTB) and pulmonary tuberculosis
(PTB) in children.
Methods
Patients under 14 years of age diagnosed with active TB in our unit
between December 2008 and September 2013 were included. Medical records
of children suspected of having tuberculosis hospitalized in Dr. Behcet
Uz Children’s Hospital (Izmir, Turkey) were reviewed. Data including
demographic characteristics, clinical history, microbiology, imaging
studies, medications and outcomes of the patients were collected from
medical records. The microbiologically confirmed active TB was defined
as the presence of at least one positive clinical specimen for
Mycobacterium tuberculosis (Mtb) in culture, or positive AFB smear
microscopy, or histological confirmation of caseating granulomas.[14]
Probable tuberculosis was defined as the presence of suggestive
radiologic signs in the absence of bacteriologic confirmation, or
radiologic certainty, positive nucleic acid amplification test for Mtb
and good clinical response to antitubercular treatment.[15]
Tests including TST, radiologic studies, conventional x-ray graphs,
computerized tomography (CT), cranial magnetic resonance imaging (MRI);
microbiological and molecular tests were used for the diagnosis of TB.
Purified protein deri¬vate of five units was used for TST.
Sample processing:
2454 samples from 1024 patients were available for analysis, including
sputum (n=511), gastric fluid (n=1633), urine (n=61), cerebral spinal
fluid (CSF) (n=14), bronchoalveolar lavage fluid (n=47) and other
sterile body fluids (n=188). All of the samples, except sterile body
fluids, were processed by standard decontamination using Mycoprosafe
(NaOH 2%-Trisodium Citrate %1,47, Salubris, Turkey).
Kinyoun acid fast-stain smear examination, Lowenstein Jensen
cultivation and automatized culture were performed to all samples. As a
result of the establishment of molecular analysis system at recent year
(2013) PCR was performed in a limited number of gastric fluid (n=282),
sputum (n=87), urine (n=50), 27 bronchoalveolar lavage fluid (n=27),
CSF (n=4) and other sterile body fluids (n=54) samples from 504
patients.
Smear, cultures and PCR tests were performed as described previously in
accordance with standard protocols and/or manufacturers’ protocols:
Kinyoun acid fast-stain smear:
Two drops (approximately 200 μl) of processed sample deposit were
placed on a slide and stained by Kinyoun fast staining method according
to the conventional methodology.
Lowenstein Jensen cultivation:
Two drops of each deposit was inoculated into a Lowenstein Jensen tube
media (GBL, Turkey) tube following the manufacturer’s protocol. The
culture was incubated in a CO2 incubator at 37°C for 42 days.
Bac/Alert 3D system:
Five hundred microliters of each deposit was inoculated into a
supplemented Bact/Alert MP bottle following the manufacturer’s protocol
(Biomerieux, France). The cultures were incubated in Bact/Alert 3D
automatized system at 37°C, and the results automatically reported.
Identification of Mycobacteria:
Five hundred microliters of each culture (Bact/Alert) positive samples
was inoculated into a supplemented Bact/Alert MP bottle in which 200
microliters 4-nitro benzoic acid (Aldrich, U.S.A.) solution prepared by
following the manufacturer’s protocol was added. For controls, a second
sample was inoculated into a 4-nitro benzoic acid free Bact/Alert MP
bottle. The cultures were incubated in Bact/Alert 3D automatized system
at 37°C, and the results automatically reported. The samples that show
no cultivation in 4-nitro benzoic acid containing medium but positive
in the control bottle were identified as Mycobacterium tuberculosis
complex. The samples with duplicate cultivation were identified as
atypical Mycobacteria.
PCR:
The PCR system (Expert MTB/RIF, Cepheid, U.S.A) integrates and
automates sample processing, nucleic acid amplification, and detection
of the target sequences in simple or complex samples using real-time
PCR and reverse transcriptase PCR. The PCR test was conducted
simultaneously with conventional procedures on decontaminated and
sterile samples following the manufacturer’s standard operating
procedure. One and a half milliliters of sample reagent was added to
0.5 ml of processed sample, and incubated at room temperature for 15
minutes with intermittent shaking and finally added to the test
cartridge and loaded onto the machine. The result was available after 2
hours.
Rifampin resistance:
For any sample with a positive result for rifampicin resistance by
Expert MTB/RIF, the corresponding isolate from the same sample isolated
by Lowenstein Jensen or Bact/Alert culture was tested for RIF
susceptibility in an external mycobacterium reference laboratory. The
primers in the Xpert MTB/RIF assay amplify a portion of the rpoB gene
containing the 81 base pair “core” region.
Tests for HIV antibodies were performed with commercial kits (Du Pont,
Wilmington, DE). Patients were grouped into two groups including EXPTB
and PTB patients for further analysis. White blood cells (WBC),
C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were
compared between EXPTB and PTB groups. CRP levels were classified into
three groups as a < 2, 2-10 and 10-20 mg/l.
This study was approved by the Local Research Ethics Board of Dr. Behçet Uz Children’s Hospital.
Statistical analysis:
SPSS, version 13.0 (SPSS Inc, Chicago, USA) was used for statistical
analyses. Independent samples t-test or a non-parametric analog,
Mann-Whitney U test, were used to compare the means of two independent
groups. The Chi-square or Fisher’s exact test were used to test for
equality of proportions between groups. P < 0.05 was considered
statistically significant.
Results
Demographic data:
A total of 129 cases of active TB was identified. Among them, 12 cases
having both EPTB and PTB manifestations were excluded from the study.
The mean age of the TB patients was 7.0±4.5 years (ranging from 3
months to 14 years of age). Forty-three subjects (36.8%) were under 5
years of age, and 74 (63.2%) were older than ten years of age. In our
study; 15 (12.8%) of the patients were under one year of age.
Clinical presentation:
Ninety-two (78.6%) of the cases had PTB and 25 (21.4%) of the cases had
EPTB (Table 1). Although six cases were diagnosed as miliary TB
according to the CT images, they were then regrouped as PTB since no
extrapulmonary focus was found. Sixty of the patients were female
(51.3%), and 57 patients (48.7 %) were male. There was no significant
difference between EXPTB and PTB groups according to the gender and age
(p=0.94; p=0.31).
Table 2 summarizes the main clinical and microbiological
characteristics of the children with PTB, EXPTB and the whole active TB
group. The most common signs and symptoms on admission were fevers in
40 cases (34.2%) and cough in 81 cases (69.2%). The incidence of cough
was significantly higher in the PTB group (81.5%) when compared with
EXPTB group (36.0%) (p<0.05). The number of patients without
symptoms including fever, cough, malaise and weight loss were
significantly higher in EXPTB (72.0%) group when compared with patients
in PTB group (13.0%) (p<0.05).
Only 37.1% of the total patients had higher leucocyte counts while
53.0% of children had increased CRP values. ESR was in normal range in
47.0% of the patients. There was no significant difference between
children with PTB and EXPTB by means of WBC, CRP and ESR (p> 0.05)
(Table 3)
TST was done in all subjects and was found to be positive in 74 (63.2%)
of the patients. We found no significant difference between PTB and
EXPTB groups by means of TST positivity (p=0.075). In this study; TST
was anergic in 11 cases (9.4%) including two patients with miliary TB,
eight with PTB and one with TB peritonitis. Only 15 patients had IGRA’s
thus this data were not included in further analysis.
The source of infection was determined in 44 of the patients (37.6%),
including father (n=21), mother (n=5), grandparents (n=7), siblings
(n=3), secondary relatives and neighbors (n=8). In eight cases; there
was more than one person as a source of infection in households. The
detection rate of source in PTB group (42.4%) was significantly higher
than the rate in EPTB group (20.0%) ( p=0.04). In the drug-resistant
group, no source of infection could be established in 5 of 9 patients
(55.5%). There was no significant difference between patients younger
than 5 years of age and 5 to 14 years of age by means of detection of
the source (p=0.26).
Microbiology:
The diagnosis of active TB was microbiologically confirmed by
Ziehl–Neelsen staining, culture or PCR. Ziehl–Neelsen staining was
positive in 14 cases (11.9%) of 117 patients. PCR was performed in 86
patients with positive results in 17 cases (22.9%). The culture
positivity in samples of sputum or gastric lavage was found in 15 of
117 cases (12.8%).
Drug susceptibility test results for isoniazid (INH), rifampicin (RIF),
ethambutol (EMB), and pyrazinamide (PYZ) were available in 15 isolates.
Resistance to INH was present in five patients (33.3 %). Resistance to
both INH and RIF (defined as multi-drug resistance, MDR) was detected
in 2 (6.6 %) cases. Two cases were resistant to all of INH, RF, EMB and
PYZ. As further analysis for other anti-Tb drugs was not available in
our institution, two patients were referred to another health care
center for this purpose.
Treatment: TB was successfully treated in 115 patients (98.2%) with
clinical and microbiological improvement. Two patients were found to be
resistant to the standard first-line anti-TB drugs. We had two relapses
in one-year follow-up time (0.85%).
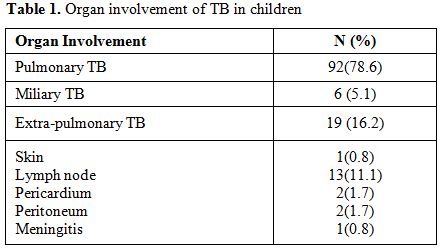 |
Table 1. Organ involvement of TB in children |
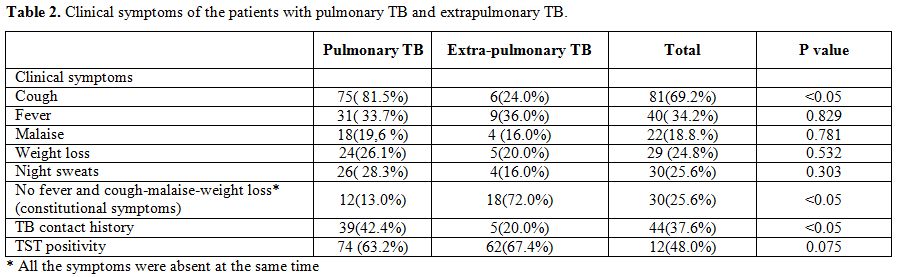 |
Table 2. Clinical symptoms of the patients with pulmonary TB and extrapulmonary TB. |
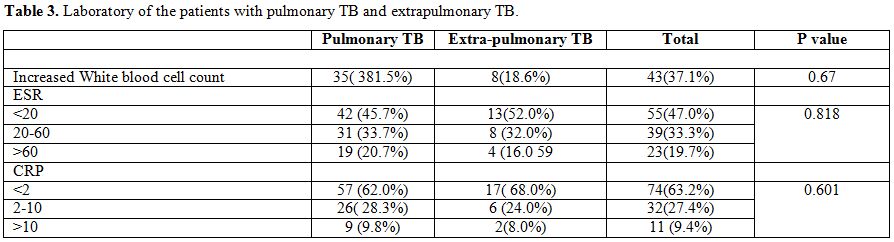 |
Table 3. Laboratory of the patients with pulmonary TB and extrapulmonary TB. |
Discussion
Every organ could be the target organ of TB. The diagnosis of EPTB
is a difficult challenge and frequently delayed since the symptoms are
non-specific depending on the affected sites. In our study, the number
of patients without symptoms including fever, cough, malaise and weight
loss were significantly higher in EPTB and 5 times more than PTB, in
accordance with previous findings().[8,16]
Moreover, the incidence of cough was significantly higher in the PTB
group (81.5%) compared to EPTB group (36.0%) (p<0.05). Absence of
classic signs and symptoms of cough, fever, night sweats, weight loss,
anorexia or fatigue in EPTB is the main factor for delays in diagnosis.
Therefore, invasive procedures are requested for an early and certain
diagnosis; of course, invasive procedures are more troublesome and
dangerous in children. In our opinion; the typical findings and
constitutional symptoms are not necessarily present especially in EPTB
and diagnosis require high clinical suspicion.
In our study the majority of the TB cases (78.6%) were associated with
pulmonary involvement supporting the findings of the recent papers from
Italy, Denmark and Turkey.[11,14,17,18]
Nearly 2/3 of the patients had EPTB alone suggesting that EPTB could be
underdiagnosed in the absence of pulmonary findings. Lymphadenopathy
(LAP) was the most prominent finding in isolated EPTB. CNS involvement
was found in one patient in our study. Current articles have reported
LAP as the common site of extra pulmonary involvement[14] however some reports had suggested that CNS involvement in TB could be as high as 15.8%.[14,18] A recent study from China reported the incidence of TB meningitis as 38.8% in TB.[19]
The low incidence of CNS TB in our study would be due to the high rate
of BCG vaccination. The protective features of BCG for meningeal
disease, despite the unequal efficiency between different geographic
regions, would be a possible mechanism for this finding.[20]
Age could be an important factor in TB development and progression.
Children have a higher probability of progression comparing to the
adults. Possibility of developing severe and extra pulmonary forms of
TB was reported to be more frequent in children under five years of
age.[11] A recent study from Italy suggested higher TB rates in children under 5 years of age,[14]
however in our study the majority of the cases were found to be older
than 5 years, suggesting that the distribution of age could show
differences from country to country.
Finding the source of TB infection is essential for controlling the TB
burden. In our study; 37.6% of the patients; had no detectable source
of infection. Moreover, the source of TB infection could not be
determined in 80% of the EPTB patients while this ratio decreases to
57,6% in PTB patients. The rate of detection of the source in children
was reported in 28.0% and 38.8%;[14,19]
moreover in a recent study a negative history of contact was associated
with extra-pul¬monary localizations, supporting our findings.[14]
In our study, negative contact history did not show any statistical
difference between age groups, this could be because mostly adult
contacts were parents or grandparents in our country, and the presence
at day-care center before 5 years of age is not frequent. The negative
contact history was present nearly half of the drug-resistant TB cases;
which indirectly reflects undetected adult patients infected with
resistant mTB. This conclusion is in accordance with the recent report
in which only 1.8% of children had developed TB as household contacts
with adult TB patients.[21]
Acute-phase reactants were reported to be high in patients with TB although they are not specific to TB.[22] Among these reactants, CRP has been suggested as a candidate biomarker for active infection with M. tuberculosis.[22,23] Moreover, Kumat et al. reported that CRP, besides other molecules, could be used for distinguishing PTB from EPTB.[23] On the contrary to this article; neither CRP nor ESR was found to be high in PTB compared to EPTB in our study.
The World Health Organization (WHO) estimates that HIV prevalence among children with TB was changing from 10 to 60%[24]
depending on the prevalence of HIV. In our clinic, only one patient who
was diagnosed as HIV infection had suffered from TB demonstrating its
low incidence in our study. In developed countries such as England, two
children with HIV per year were presented with active TB over 5 year
period with a total of 5.5% of HIV infected patients, had TB[25] supporting our findings.
In our study, INH resistance was found to be high as 33.0%; however,
this high proportion was thought to be due to the low number of
isolated mycobacteria. In a recent systemic review of 95 studies
including 8,351 children with TB, the median proportion of children INH
resistant was 8%.[26] In one study from Turkey; frequency of INH-resistant TB was reported as 6.7 % in children.[27]
However, this various findings supported that isoniazid-resistant
tuberculosis in children is a widespread and geographically variable
phenomenon.
Conclusion
EPTB diagnosis is more difficult than PTB in children due to the
various problems such as absence of associated pulmonary involvement,
lack of constitutional symptoms and negative TB exposure history
compared to PTB. Even acute phase reactants failed to be useful in
discrimination of EPTB. New strategies are required for improving the
diagnosis of EPTB in children.
References
