Central Nervous System Involvement in Adult Acute Lymphoblastic Leukemia: Diagnostic Tools, Prophylaxis, and Therapy
Maria Ilaria Del Principe1, Luca Maurillo1, Francesco Buccisano1, Giuseppe Sconocchia2, Mariagiovanna Cefalo1, Giovanna De Santis1, Ambra Di Veroli1, Concetta Ditto1, Daniela Nasso1, Massimiliano Postorino1, Marco Refrigeri1, Cristina Attrotto1, Giovanni Del Poeta1, Francesco Lo-Coco3, Sergio Amadori1 and Adriano Venditti1
1 Ematologia, Dipartimento di Biomedicina e Prevenzione, Università Tor Vergata, Roma, Italia.
2 Istituto di Farmacologia Translazionale, Dipartimento di Medicina, CNR, Roma, Italia.
3 Fondazione S. Lucia
Corresponding author: Maria Ilaria Del Principe. Istituto di
Ematologia, Policlinico Tor Vergata. Viale Oxford 81 –00133, Roma,
Italia. Tel: +39 06 20903226, Fax +39 06 20903221. E-mail:
del.principe@med.uniroma2.it
Published: November 01, 2014
Received: September 01, 2014
Accepted: October 23, 2014
Meditter J Hematol Infect Dis 2014, 6(1): e2014075, DOI
10.4084/MJHID.2014.075
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
In adult patients with acute
lymphoblastic leukemia (ALL), Central Nervous System (CNS) involvement
is associated with a very poor prognosis. The diagnostic assessment of
this condition relies on the use of neuroradiology, conventional
cytology (CC) and flow cytometry (FCM). Among these approaches, which
is the gold standard it is still a matter of debate. Neuroradiology and
CC have a limited sensitivity with a higher rate of false negative
results. FCM demonstrated a superior sensitivity over CC, particularly
when low levels of CNS infiltrating cells are present. Although
prospective studies of a large series of patients are still awaited, a
positive finding by FCM appears to anticipate an adverse outcome even
if CC shows no infiltration. Current strategies for adult ALL
CNS-directed prophylaxis or therapy involve systemic and intrathecal
chemotherapy and radiation therapy. An early and frequent intrathecal
injection of cytostatic combined with systemic chemotherapy is the most
effective strategy to reduce the frequency of CNS involvement. In
patients with CNS overt ALL, at diagnosis or upon relapse, allogeneic
hematopoietic stem cell transplantation might be considered. This
review discusses risk factors, diagnostic techniques for identification
of CNS infiltration and modalities of prophylaxis and therapy to manage
it.
|
Introduction
Over the last two decades, clinical trials have generated improved
response rates in adult patients with acute lymphoblastic leukemia
(ALL). Advances in understanding disease biology, adoption of induction
and maintenance programs based on risk-adapted strategies, similar to
the treatment in children, and better supportive care, have all
contributed to those improvements. Overall, adults with ALL have a
60-90% chance of attaining a first complete remission using combination
chemotherapy.[1-3] In this context of a better-controlled systemic
disease, central nervous system (CNS) involvement has become an even
more influential limitation to achievement of long-term cure and a
primary cause of mortality.
CNS may be involved at initial
diagnosis or relapse. At initial diagnosis, about 5% of adults has CNS
involvement[4,5] being, their duration of overall survival (OS) shorter
than the one of those without CNS involvement. The incidence of CNS
involvement upon relapse is quite variable. Surapaneni et al[6]
reported a CNS relapse rate of 7% whereas, in the French
LeucémieAiguësLymphoblastique de l’Adulte (LALA) trials, 15% of the
patients developed a CNS relapse.[7] Isolated CNS recurrences range
from 0% to 11%,[1,8,9] while CNS and bone marrow relapses occur in an
additional 1-4% of the patients.[10] Most patients with isolated CNS
recurrence subsequently relapse in the bone marrow too. Although these
figures might be underestimated, given the possibility that physicians
do not systematically investigate CNS involvement at the time of
relapse, CSF analysis and CNS prophylaxis should be mandatory in each
treatment protocols. Prognosis of adult patients who experience CNS
relapse is very poor with a median OS of six months and a projected
5-year OS of zero.[11]
In the present review, we discuss some
aspects of this serious complication, such as risk factors, diagnostic
tools, prophylaxis, and therapy.
Risk Factors for Cns Localization
Several
risk factors have been associated with the development of ALL CNS
involvement. Age seems to be a key factor with a higher incidence in
younger adults.[12] Mature B-cell subtype is also associated with an
increased risk of CNS localization. A retrospective analysis by Bassan
and colleagues[13] indicates that adult patients with mature B-ALL have
an 18% incidence of CNS involvement at presentation compared with an
overall incidence of 4.5%. In contrast, Lazarus et al.[4] reported a
higher incidence of CNS involvement at diagnosis in association with
the T-cell immunophenotype. The Philadelphia (Ph) chromosome positivity
is also considered as a high-risk signature for CNS leukemia.[14]
Patients with CNS involvement at diagnosis are more likely to have
lymph node enlargement, mediastinal mass,[4,7] and other
extra-medullary localizations.[7] Finally, lactate dehydrogenase (LDH)
level, white blood cell (WBC) count and proliferative index have been
identified as additional risk factors rendering patients prone to CNS
relapse. Incorporating elevated LDH, serum β2-microgobulin
and high leukemia cell proliferation rate in a multivariate analysis,
the colleagues from the M.D. Anderson Cancer Center identified discrete
categories of adult patients with different chances to develop CNS
leukemia.[14,15] Patients with one risk factor had 13% probabilities to
develop CNS disease at 1 year, if two or more risk factors were present
probabilities increased to >20%. Above all, the presence of leukemic
cells in the cerebrospinal fluid (CSF) is considered the most crucial
feature of risk. Traditionally, patients are considered at increased
risk of CNS relapse if detection of blast cells in CSF is accompanied
by a CSF-WBC count exceeding 5 cells/μl. In 1990s, it was proposed that
the presence of any number of blast cells in the CSF, regardless of
CSF-WBC count, is associated with an increased risk of CNS
relapse.[5,16,17] Based on this, a specific risk score was generated:
CNS1, denoting the absence of identifiable leukemic cells in CSF; CNS2,
denoting the presence of blast cells in a CSF sample containing <5
WBC/μl; and CNS3, a CSF sample that contains ≥5WBC/μl
together with identifiable blast cells, or the presence of cerebral
mass, or cranial nerve palsy together with leukemic cells in the CSF.
An increased incidence of CNS relapse has also been observed when a
traumatic lumbar puncture is associated with the presence of blast cell
in the CSF. The relevance of this CNS risk score has been subject of
dispute since several authors did not find significant differences in
outcome, for patients categorized as CNS1 versus CNS2.[18,19] In
addition, the clinical significance of traumatic lumbar puncture
remains unclear and controversial.[20] Diagnostic Tools
CNS involvement in ALL remains under-diagnosed; this is
confirmed by the autoptic demonstration of CNS infiltration in patients
who, at the onset of ALL, were considered as having bone marrow disease
only.[21] Therefore, a correct and timely diagnosis
still represents a challenge. Besides the clinical evaluation of
neurological signs and symptoms, three independent techniques are used
to diagnose CNS disease in ALL patients: CNS neuroradiology, CSF
cytology and flow cytometry examination.[22]
Clinical evaluation:
Clinical manifestations may vary, depending on the size of leukemic
infiltration, the sites and number of sites involved. Brain
localization scan cause headache, alteration of mental status, walking
abnormalities, nausea and vomiting, loss of consciousness, seizures,
gait or sensory disturbances, papilloedema. Cranial nerves localization
may be associated with diplopia, hearing and visual loss, facial
numbness, dysphagia. Spinal involvement can determine focal weakness
(of legs more often than arms), paresthesias, back pain, radicular
pain, bladder, and bowel dysfunction. The correct interpretation of
clinical presentation is often challenging. In fact, neurological
symptoms and signs may be subtle, and sometimes attributed to other
causes, directly or indirectly related to ALL, such as
hyperleukocytosis, metabolic encephalopathy, treatment-related
neuropathy, opportunistic infections. In some patients, CNS involvement
develops completely asymptomatic and therefore detected by routine
lumbar puncture.
Neuroradiology:
A variety of neuroradiographic methods are available to evaluate
patients with suspected CNS involvement, including cranial computed
tomography (C-CT), gadolinium-enhanced brain and spine magnetic
resonance imaging (MRI). C-CT is abnormal in about 25% of patients with
carcinomatous meningitis.[22-24] However, the
detection power of this technique decreases when it comes to the
evaluation of patients with suspected leukemic meningitis, so that
positive findings are significantly less than the 25% achievable in
solid tumors meningitis.[25] MRI with gadolinium enhancement has a superior sensitivity than cranial C-CT[24]
and accordingly, it is the radiologic first choice to explore CNS
localization of ALL. Since ALL can potentially infiltrates any area of
neuraxis, T1-weighted sequences, with and without contrast, combined
with fat suppression T2-weighted sequences, represent the standard
techniques to scan the entire CNS, in patients for whom localizations
are suspected. Indicative of CNS disease are MRI enhancement and/or
enlargement of cranial nerves, nodular or linear leptomeningeal
enhancement extending into sulci or basal cisterns, and
intradural-enhancing nodules, especially those located at the cauda
equine. Finally, MRI allows identifying abnormalities, such as
leukoencephalopathy, brain atrophy, old hemorrhages or old infarcts,
due to treatment but not to disease. Despite its superiority over C-CT,
even MRI has some pitfalls. One study found that MRI was capable of
detecting 100% of case of neoplastic meningitis due to solid tumor but
only 44% of those due to B-cell ALL.[26] It has been
estimated that the potential false-negative rate of MRI is as high as
60-65% and the false-positive one about 10%. These data limit the use
of MRI as a stand-alone diagnostic tool, and a normal MRI imaging does
not provide certainty about the absence of occult CNS disease in the
course of ALL.
CSF examination:
CSF examination is the most useful laboratory test in the diagnosis of
ALL CNS involvement. Abnormalities include increased opening pressure
(>200 mm of H20), elevated protein (>50 mg/dl) and decreased glucose (<60 mg/dl) CSF concentration and increased WBC count (>5/mm3),
which is not diagnostic but only suggestive of CNS involvement. In
infectious diseases, like bacterial and viral meningitis, there may be
a marked elevation of WBC count. Besides, some authors observed no
significant difference in total protein, glucose and WBC count between
patients with CNS localization and patients without.[27,28]
The
presence of leukemic cells in the CSF is diagnostic for CNS involvement
and, if the lumbar puncture is clinically and technically feasible, CSF
examination must be performed. CNS leukemia is defined as unequivocal
morphologic evidence of leukemic blast in the CSF and/or mononuclear
cell count ≥5/μl.
Morphologic examination is performed on cytospin preparation stained
with May- Grunwald-Giemsa. Conventional cytology (CC) is estimated to
have a >95% specificity for CNS involvement. However, it has a
relatively low sensitivity (<50%) and consequently is often falsely
negative. Low sensitivity of CC is due to paucity of cells in CSF and
morphological similarities that can make it difficult to distinguish
benign from malignant cells. In the largest postmortem analysis of
patients with neoplastic meningitis, Glass et al.[29]
showed that 41% had leukemic meningitis on autopsy but a negative
pre-mortem CC. They also demonstrated that, in patients with a focal
leptomeningeal disease, the occurrence of cytological false negatives
was >50%, emphasizing the frequent co-occurrence of CNS disease and
negative CC. In patients with suspected CNS involvement, because of the
low detection rate, lumbar punctures are often repeated up to three
times. However, even after repeated CSF sampling, false negative
cytology reportedly occurs in 10% to 20% of patients with
leptomeningeal disease. In a series including lymphomatous and leukemic
meningitis Kaplan et al.[30] found the frequent
dissociation between CSF cell count and malignant cytology (29% of
cytological positive CSF had concurrent CSF count <4/μl).
Flow
cytometric (FCM) immunophenotyping is a valuable tool for the diagnosis
and staging of haematological disorders involving lymph nodes, blood,
and bone marrow. Clinical flow cytometry assays have been implemented
to reliably detect phenotypically abnormal cells representing 0,01% of
events (1 cell in 104) and is a useful tool for monitoring minimal residual disease in acute leukemia.[31]
Although powerful and extremely sensitive, FCM assay relies on rigorous
technical requirements: CSF samples of sufficient volume must be
obtained via lumbar puncture. After sampling, CSF should be processed
within 1 hour to avoid cell deterioration. In this view, some authors
recommend the use of fixative (TransFix/ethylenediaminetetraacetic acid
EDTA; Immunostep SL Salamanca, Spain).[32] The
samples should be collected in tubes with no anticoagulant and
transferred to the laboratory as quick as possible. To obtain the
maximum number of cells for analysis, CSF should be concentrated by
low-speed centrifugation.[33] One subject of controversy pertains the threshold defining FCM positivity. Di Noto et al.[34] use a threshold of at least 30 events; in a less restrictive approach, Qujiano et colleagues[32] considered a minimum of ten events, shaping a cluster, as a proof of CNS infiltration. Subira et al.[35]
suggest that at least 9 B-cell or 12 T-cell events are required to
reach a confidence level of 95%, thus indicating the presence of CNS
disease. These results are in agreement with those of Craig et
coworkers,[36] in the experience of whom, at least 13
clustered events displaying identical features are required to identify
a specific cell population. In general, the presence of fewer than 5
clustered events is not regarded as related to the presence of a
specific population. A qualitative approach might be an alternative to
the quantitative one. Rather than defining a numerical threshold, it
might be important to take into account how tightly the cells are
clustered and whether their characteristics profile a particular
disease entity.[31] The use of a cocktail of 6-9
monoclonal antibodies represents a further strategy to increase FCM
sensitivity and enhance qualitative information achievement.[37]
Based on the above-mentioned considerations, FCM is considered to be
more sensitive than CC for the detection of malignant hematologic cells
in CSF.
A number of studies published in recent years, dealing
with detection of CNS disease in ALL or newly diagnosed aggressive
non-Hodgkin’s Lymphomas, demonstrated the superior sensitivity of FCM
over standard cytology.[27,32,34,38]
In a retrospective analysis of CSF samples collected from 219 patients
with leukemia/lymphoma, FCM discovered CNS infiltration in 44 patients,
of these only 19 were positive by CC. Patients with a positive finding
by CC had a higher incidence of neurological signs and symptoms and CSF
pleocytosis.[28] FCM characterizes for the ability to reveal hematologic disease in CSF specimen even when cellularity is very low.[36,39]
This peculiarity has been confirmed in pediatric ALL patients where FCM
was able greatly to improve the recognition of occult CSF involvement.[40] Mitri et al.[41]
applied FCM to 267 CSF samples obtained from 80 adult ALL patients and
fund that FCM had 100% sensitivity and specificity in detecting
lymphoblasts. The authors concluded that additional information is
needed to determine the clinical significance of a single FCM
positivity. In fact, in the absence of morphologically evident blasts
on CC, it is still a matter of debate whether or not the FCM positivity
affects clinical outcome in ALL. Although Mitri et al. analyzed a
consistent number of samples, one would argue that they provided no
information whether or not their patients belonged to a consecutive
series. In addition, they analyzed CSF samples in a 4-color assay
which, on a technical ground, might not be appropriate to detect rare
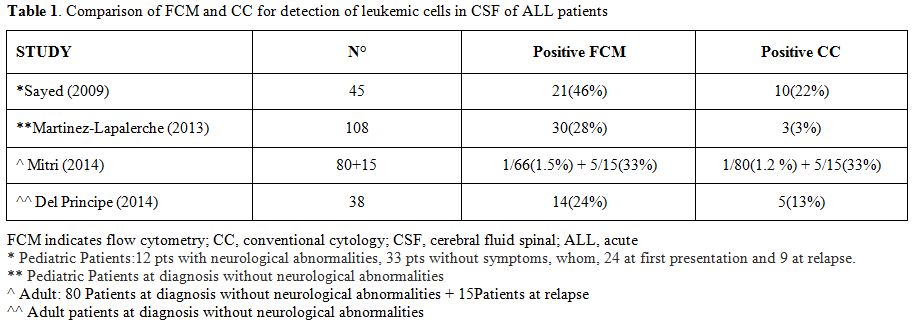
events. These observations may explain why Mitri et al.[41] found a positive CNS sample with FCM only in 1.5% of newly diagnosed cases whereas we[42] and others[43] have found in 24% and 28%, respectively (Table 1).
|
|
Table 1. Comparison of FCM and CC for detection of leukemic cells in CSF of ALL patients |
In patients affected with high-risk non-Hodgkin lymphomas
and Burkitt’s lymphomas, a single FCM positivity of CSF was associated
with a significantly higher risk of CNS relapse and a worse prognosis.[44,45]
One hundred and 68 CSF samples taken from 31 patients with ALL were
analyzed by FCM and conventional cytology. In all samples findings were
concordant but in 10, results of which were discrepant. However, all
patients with negative FCM results remained free from CNS disease.[35]
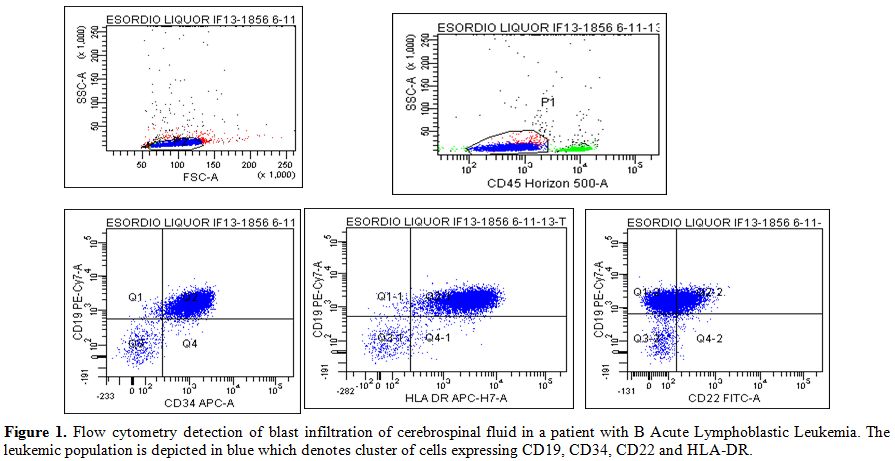
In a population of 38 adults with ALL or lymphoblastic lymphoma, we
confirmed that FCM was more sensitive than CC in recognizing CSF
localization (Figure 1). In our
study, CC failed to identify the presence of neoplastic cells in 9/14
(64%) FCM positive patients, and 3 (33%) of these 9 developed an overt
CNS disease. None of the FCM negative patients experienced such a
progression. Furthermore, the median overall survival of patients with
a single FCM positivity was intermediate between patients double
positive and negative.[42] Consistently, the
molecular CSF detection of a leukemic signature in pediatric patients
correlated with a shorter 4-year event-free survival compared with
those without such a signature.[45] In a multicentric prospective study of children with ALL, Martinez-Laperche et al.[43]
demonstrated that identification by FCM of subclinical leukemic
infiltration of CSF during maintenance correlated with a significantly
shorter duration of 3-years relapse-free and overall survival. However,
despite the efficient sensitivity of FCM, complementary diagnostic
approaches might be required to solve cases such as those with
neurological symptoms but with no radiological or cytometric evidence
of CNS disease. In this regard, it has been demonstrated that
quantification of soluble CD19 represents a surrogate biomarker for
occult CNS lymphoma,[47] paving the way to its assessment even in B-ALL.
|
|
Figure 1. Flow cytometry detection of blast
infiltration of cerebrospinal fluid in a patient with B Acute
Lymphoblastic Leukemia. The leukemic population is depicted in blue
which denotes cluster of cells expressing CD19, CD34, CD22 and HLA-DR. |
Prophylaxis of CNS localization:
Due to the limited penetration of cytostatic drugs across the
blood-brain barrier into the CSF and brain parenchyma, CNS represents a
sanctuary site. Blood-brain barrier (BBB) is a highly specialized
network where interactions between astrocytes and vascular endothelium
counteract delivery of many chemotherapeutic agents. The insufficient
CNS accumulation of the drugs conventionally used to treat ALL explain
why, in absence of adequate prophylaxis, recurrence at this site is
observed in approximately 30% of adult patients.[48] Standard CNS prophylaxis in ALL relies on the combined use of systemic and intrathecal (IT) chemotherapy or radiation therapy.
Systemic chemotherapy:
The prophylactic role of systemic chemotherapy is strictly dependent on
factors such as the ability of the drugs to cross the BBB and to
distribute uniformly within the parenchyma, and their active extrusion
from CNS. The ability of high-dose cytarabine (ARAC) and metotrexate
(MTX) to penetrate the BBB makes them suited agents for CNS prophylaxis
in ALL.[48,49] MTX is the most widely used
hydrophilic chemotherapeutic agent, but high doses must be administered
to achieve therapeutic drug concentration in CNS. The bolus intravenous
injection increases brain delivery of MTX compared with the slow
intravenous infusion. With the use of calcium folate based rescue, very
high systemic doses of MTX (5-8 g/m2)
can be administered safely, and therapeutic levels can be achieved
despite its limited capability of CSF penetration. High-dose ARAC has
also been successfully used for CNS prophylaxis. Since the ARAC
half-life in CSF is 8-fold greater than in plasma, prolonged cytotoxic
concentrations can be achieved with doses of 3 g/m2 given every 12 hours. Cortes et al.[50]
demonstrated the efficacy of the combination of high-dose of both MTX
and ARAC with the adjunct of IT ARAC, to prevent CNS recurrence in
adult patients with ALL. Although MTX and ARAC were identified as the
most effective drugs for systemic CNS prophylaxis, no agreement has
been reached on the optimal doses and number of cycles at which they
should be delivered. In the Cortes’ study,[50] MTX
dose might be too low for an effective CNS penetration whereas that of
ARAC too high in terms of toxicity. Current approaches favor the use of
higher MTX (2.5-3 g/m2) and lower ARAC (2 g/m2)
doses. Steroids have also been extensively used. Dexamethasone
concentration can reach higher CSF levels and has a longer half-life
than prednisone.[51,52] Annino et al.[53]
reported that the addition of high-dose of dexamethasone to systemic
treatment reduces the rate of CNS recurrence to 2%. Systemic etoposide[54] and 6-mercaptopurine[55]
can also reach adequate concentrations in CSF, as well as systemic
administration of L-asparaginase can result in prolonged CSF depletion
of L-asparagine.[56] In childhood ALL, delivery of
Erwinia-derived asparaginase was associated with CNS relapse at a
nearly six times rate than patients treated with Escherichia
coli-derived asparaginase.[57] The experience with
the use of systemic chemotherapy indicates that, when given alone, it
is not sufficient for CNS prophylaxis. This is mainly due to the
difficulties to maintain persistent drugs concentration while in
presence of remarkable side effects (neurotoxicity, mucositis,
diarrhea, fever, liver dysfunction) associated with administration of
high-dose MTX and/or ARAC.
Intrathecal chemotherapy (IT):
IT chemotherapy is the preferred method for CNS prophylaxis. Commonly
used IT therapies include injection of MTX, ARAC, and liposomal ARAC.
MTX has always been considered superior to ARAC because it persists
longer in the CSF and penetrates more deeply into meninges and CNS
parenchyma.[58] MTX dose can be variable with some authors suggesting 12.5 mg,[3] others 15 mg.[7,59]
It can be given either alone or in conjunction with ARAC and
hydrocortisone or methylprednisolone. It was thought that the
combination of MTX with ARAC may have additive or synergistic effects,
with the role of corticosteroids being the one to attenuate
arachnoiditis associated with MTX/ARAC administration. ARAC is the
second most widely used agent for IT prophylaxis. It is usually
injected at doses of 30 mg/m2, which achieves peak concentrations of up to 1 mM.[60]
After IT injection of ARAC, conversion to the inactive metabolite
uracil arabinoside is negligible, because of the significantly low
cytidine deaminase activity in the brain and CSF; this enhances a
longer half-life of ARAC in CSF than in plasma. Usually, IT
chemotherapy is initiated early during induction therapy and continued
throughout the maintenance. The number of IT injections is variable. In
the LALA trials, CNS prophylaxis consisted of 6-8 IT injections of ARAC
and MTX, plus or minus methylprednisolone (40mg), in patients receiving
only chemotherapy, and 5 IT injections in those also transplanted.[3,7] In the HypeCVAD program, 16 IT treatments were planned.[2]
More recently, IT liposomal ARAC has been used for the prophylaxis of
CNS malignant involvement. ARAC is encapsulated in a multivescicular
liposome preparation named DepoFoam, and the product is known as
DTC-101 or DepoCyt.[61] This encapsulation modifies
the pharmacokinetics of the free ARAC released in CSF in a way that the
cytotoxic concentration of the drug is maintained for as long as 14
days. A phase II randomized trial of radiation–free CNS prophylaxis,
comparing IT triple therapy (methotrexate 12.5 mg, cytarabine 50mg,
prednisone 40mg) with liposomal ARAC (50mg), showed that liposomal ARAC
was feasible and at least as effective as other regimens.[62]
In
the adult ALL German Multicenter Study Group prospective trial,
liposomal ARAC confirmed its safety and effectiveness even in the
subgroup of older (>55 years) Ph-negative patients. Analysis of
efficacy indicated that CR was increased, and mortality decreased in
the arm receiving IT liposomal ARAC likely due to a less pronounced
bone marrow toxicity.[63]
Radiation Therapy:
Although cranial (CI) and/or cranio-spinal irradiation (CSI) is the
oldest approach for CNS prophylaxis in pediatric patients with ALL,[64,65]
few studies have systematically explored its prophylactic role in
adults. In the prospective trial of Southeastern Cancer Study Group,
random assignment to CNS prophylaxis, including CI, or not resulted in
a significant prolongation of CNS relapse-free interval for patients
receiving CNS prophylaxis.[66] Sanders et al.[67]
reported the effectiveness of CSI in preventing CNS recurrence in adult
patients who achieved complete remission. Although CI/CSI can be an
effective form of CNS-directed therapy it is often associated with late
adverse effects, such as endocrinopathy, neurocognitive dysfunction,
and neurotoxicity. These side effects are fewer and less pronounced in
adults than in children, although patients aged >60 years appear to
be more susceptible than younger to cognitive impairment. It remains
not clarified what dosage of CI/CSI and what prophylaxis strategy is
the best. Twenty-four grays are the standard prophylactic dose for CI
in combination with IT-MTX. Others found that a dose of 18 grays is
equally effective.[68] There have also been attempts to omit CI in clinical trials of adult patients. Kantarjian et al.[2]
reported that systemic MTX and ARAC plus IT-MTX reduced the rate of CNS
recurrence to 4%, with no need of CI/CSI. Furthermore, in a study
recruiting a series of 467 adult patients who received IT and high-dose
of systemic therapy, but not CI, the frequency of CNS recurrence was
similar to that observed in protocols including prophylactic CI.[59]
The phase 2 study 19802, from Cancer and Leukemia Group B (CALGB),
demonstrated that the combination of high-dose systemic and IT MTX can
substitute for CI. In fact, isolated CNS relapses occurred in 6% of the
patients, a rate that is comparable to the one of four prior CALGB
studies including CI.[69]
Therapy of CNS Localization
CNS
prophylaxis in adults with ALL determines a reduction of CNS
localization by 20-30%. Nevertheless, about 10% of subjects who are
diagnosed with ALL eventually develop overt CNS disease. Although such
a circumstance connotes a very adverse prognosis, the available
therapeutic options are as the same as those used for CNS prophylaxis.
As a consequence, strategies such as more frequent IT treatments and
intensification of systemic chemotherapy have been adopted. In the LALA
trials,[3,7] patients with CNS
involvement at diagnosis were treated with 18 double (ARAC plus MTX) or
triple (ARAC, MTX and methylprednisolone) IT injections associated with
a pre-transplant CI of 15-20 grays. In the absence of HSCT, patients
received a 24 grays CI. When compared with MTX or ARAC administered
twice a week, liposomal ARAC has a similar safety profile and same or
even better effectiveness in the treatment of lymphomatous meningitis.[70]
Side effects commonly associated with liposomal ARAC include headache,
arachnoiditis, and confusion; to mitigate the occurrence of
arachnoiditis, liposomal ARAC should be given in conjunction with
dexamethasone.[71] Because of the occurrence of
severe neurotoxicity, an additional precaution, and strict surveillance
should be adopted when IT liposomal ARAC and BBB penetrating systemic
agents are administered simultaneously or in close sequence.[72]
In a phase 2 European trial, 19 patients with isolated or bone marrow
associated CNS relapse were treated with liposomal ARAC and systemic
chemotherapy. Liposomal ARAC was administered at dosage of 50 mg on day
1 and continued with an administration every 14 days for a maximum of
five additional injections. Early complete cytological remission of CSF
was observed in 74% of the patients.[73] It has been
observed that patients with CNS overt leukemia at diagnosis, by
intensifying the therapy, have a similar outcome than those who did not
present with this condition.[7] In the international MRC UKALLXII/ECOG 2993 trial, Lazarus and coworkers[4]
observed CNS involvement in 77 of 1508 (5%) adult patients with ALL. In
addition to treatment by protocol, these 77 patients received IT or
intra-ventricular MTX (12.5 mg three times/week) followed or not, at
physicians’ discretion, by CI. CI or CSI were administered at dosage of
24 and 12 grays, respectively. After induction and intensification, all
patients were recruited to receive either consolidation/maintenance or
allogeneic hematopoietic stem cell transplantation. Complete remission
rate in patients with or without CNS disease was comparable (90%)
whereas 5-year overall survival rate was 29% and 38%, respectively
(p=.03). The authors concluded that both allogeneic hematopoietic stem
cell transplantation and chemotherapy intensification are valid options
to improve outcome of patients with active CNS disease at diagnosis.
Finally, it should be pointed out that the therapeutic role of CI/CSI
is not clearly defined as the prophylactic one. It is very marginal
when the CNS involvement occurs as a relapse in patients who have
already been irradiated. In this situation, it should be delayed until
completion of systemic chemotherapy. Ph-chromosome positive ALL:
Treatment of Ph-positive ALL has been subjected to substantial changes
since the introduction of BCR-ABL tyrosine kinase inhibitors (TKI).
Exploring to what extent the use of TKI might prevent CNS localization
of ALL has been a major point of interest. Imatinib is the first
generation TKI approved for the treatment of patients with Ph-positive
ALL and, despite its use, up to 20% of treated patients develops CNS
relapse.[74] In many cases, these relapses occur in patients with morphologic complete remission[74] and have been attributed to the insufficient penetration of imatinib into the CSF.[75]
Dasatinib, a second-generation TKI of SRC-kinase and BCR-ABL, has shown
significant activity in adults with imatinib-resistant or -intolerant
Ph-positive ALL.[76] BBB penetration of dasatinib was
observed in pre-clinical mouse models of intracranial Ph-positive
leukemia and in pharmacokinetic studies of a series of 22 patients with
Ph-positive ALL or chronic myeloid leukemia.[77]
Detectable levels of dasatinib were found in only in 6 (2 adults and 4
children) of these 22 patients, thus its reported clinical activity in
CNS localization of Ph-positive ALL is anecdotic and still awaits for a
formal demonstration. Similar to dasatinib, nilotinib, is a
second-generation TKI which in preliminary studies has demonstrated
activity in treating CNS localization of Ph-positive leukemia.[78]
Hypothetic reasons for nilotinib activity rely on its pharmacokinetic
profile. In fact, nilotinib has a high protein-binding affinity, which
contrasts with the low protein concentration in CSF; this condition is
supposed to translate into a relatively higher amount of free and
therefore active nilotinib in CSF than in blood.[78]
Finally, aggregation studies have indicated that imatinib and dasatinib
do interfere with platelets function whereas nilotinib does not.[79]
This might have practical implications in thrombocytopenic patients.
Among ten adults with Ph-positive ALL receiving imatinib, Patel et al.[80]
described 3 instances of subdural hematomas occurring after IT
injection of chemotherapeutic agents. Given the apparent lack of effect
of nilotinib on platelet aggregation, the authors suggest that this TKI
should be considered for combination therapies including systemic and
IT delivery of cytotoxic drugs.Chimeric antigen receptor (CAR):
Engineered CAR-T cells targeting CD19 or CD20 antigens are emerging as
powerful therapies in hematologic B-malignancies, and CAR-T cells were
found in CSF of several patients recruited to dedicated trials.[81,82]
CAR-T cells presence in CSF might be due to the enhanced cell
trafficking through BBB promoted by IL6 release following CAR-T
infusion.[83] Alternatively, authors have claimed
that some cross-reactivity or undetectable expression of CD19 in the
brain might trig CAR-T cells migration to CSF.[81]
Whatever the reason is underlying the presence of CAR-T cells into CSF,
an open question remains whether these might have a role in eradicating
CNS disease. Lee et al.[84] reported that in 3 of
eight patients treated for a diagnosis of refractory B-malignancies,
CAR-T cells were detected in CSF. Of these 3, one with a stage CNS2 at
the time of trial enrollment cleared all CSF blasts as demonstrated by
flow-cytometry. Very recently, it has been shown in an ALL pediatric
population that CAR-T cells were detectable in CSF, and that 2, whose
CSF contained blast cells at the time of CAR-T infusion, became
subsequently free of CNS.[85] Conclusions
In ALL, effective CNS clearance requires adequate systemic and/or IT
prophylaxis and therapy. The devastating effects of CNS relapse and the
subsequent intensive CNS-directed therapy both require that the
patients are properly stratified in order to avoid over and
undertreatments. Owing to its superiority over CC in detecting even low
levels of infiltrating cells, FCM may well serve the purpose of
risk-stratification and should therefore become a routine tool for
diagnostic assessment of ALL. Further and large studies are needed to
standardize the procedures and permit an optimal clinical application
of this technique.
References
- Thomas X, Boiron JM, Huguet F, Dombret H, Bradstock
K, Vey N, et al. Outcome of treatment in adults with acute
lymphoblastic leukemia: Analysis of LALA-94 trial. J ClinOncol 2004;
22: 4075-86 http://dx.doi.org/10.1200/JCO.2004.10.050 PMid:15353542

- Kantarjian
HM, O'Brien S, Smith TL, Cortes J, Giles FJ, Beran M et al. Results of
treatment with Hyper-CVAD, a dose-intensive regimen in adult acute
lymphocytic leukemia.J Clin Oncol 2000; 18:
547-61 PMid:10653870
- Thomas X, Le QH. Central Nervous system involvement in adult acute lymphoblastic leukemia. Hematology 2008; 13:293-302 http://dx.doi.org/10.1179/102453308X343374 PMid:18854093
- Lazarus
HM, Richards SM, Chopra M Litzow MR, Burnett AK, Wiernik PH, et
al.Medical Research Council (MRC)/National Cancer Research Institute
(NCRI) Adult Leukaemia Working Party of the United Kingdom and the
Eastern Cooperative Oncology Group.Central Nervous system involvement
in adult acute lymphoblastic leukemia at diagnosis: results from
international ALL trial MRC UKALL XII/ECOG E2993. Blood 2006; 108:
465-72 http://dx.doi.org/10.1182/blood-2005-11-4666 PMid:16556888 PMCid:PMC1895498
- Jabbour
E, Thomas D, Cortes J, Kantarjian H, O'Brien S. Central Nervous System
Prophylaxis in Adults with Acute Lymphoblastic Leukemia. Cancer 2010; http://dx.doi.org/10.1002/cncr.25008
- Surapaneni
UR, Cortes JE, Thomas D, O'Brien S, Giles FJ, Koller C, et al. Central
Nervous system relapse in adults with acute lymphoblastic leukemia.
Cancer 2002; 94: 773-79 http://dx.doi.org/10.1002/cncr.10265 PMid:11857312
- Reman
O, Pigneux A, Huguet F, Vey N, Delannoy A, Fegueux N, et al. Central
nervous system involvement in adult lymphoblastic leukemia at diagnosis
and/or at first relapse: Results from the GET-LALA group. Leuk Res
2008; 32(11): 1741-50 http://dx.doi.org/10.1016/j.leukres.2008.04.011 PMid:18508120
- Linker
C, Damon L, Ries C, Navarro W. Intensified and shortened cyclical
chemotherapy for adult acute lymphoblastic leukemia. J Clin Oncol.
2002;20(10):2464-71 http://dx.doi.org/10.1200/JCO.2002.07.116
- Annino
L, Vegna ML, Camera A, Specchia G, Visani G, Fioritoni G, et al.GIMEMA
Group.Treatment of adult acute lymphoblastic leukemia (ALL): long-term
follow-up of the GIMEMA ALL 0288 randomized study. Blood 2002; 99(3):
863-71 http://dx.doi.org/10.1182/blood.V99.3.863 PMid:11806988
- Gökbuget
N, Stanze D, Beck J, Diedrich H, Horst HA, Hüttmann A, et al. German
Multicenter Study Group for Adult Acute Lymphoblastic LeukemiaOutcome
of relapsed adult lymphoblastic leukemia depends on response to salvage
chemotherapy, prognostic factors, and performance of stem cell
transplantation.Blood. 2012;120(10):2032-41. http://dx.doi.org/10.1182/blood-2011-12-399287 PMid:22493293
- Fielding
AK, Richards SM, Chopra R, Lazarus HM, Litzow MR, Buck G, et al.
Medical Research Council of the United Kingdom Adult ALL Working Party;
Eastern Cooperative Oncology Group. Outcome of 609 adults after relapse
of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study.
Blood. 2007;109(3):944-50. http://dx.doi.org/10.1182/blood-2006-05-018192 PMid:17032921
- Pavlovsky
S, Eppinger-Helft M, Sackmann MF. Factors that influence the appearance
of central nervous system leukemia. Blood 1973; 2: 935-38
- Bassan
R, Intermesoli T, Di Bona E, Pogliani E.M.G. Rossi, Fabris P. Central
nervous system involvement in adult acute lymphoblastic leukaemia:
retrospective analysis from the Northen Italy Leukaemia Group (NILG) on
687 total patients (1979-2004). Abstract 0418. Presented at the 10th
Congress of European Hematology Association. Stockhlm, Sweden, June
2-5, 2005
- Kantarjian HM, Walters RS,
Smith TL, Keating MJ, Barlogie B, McCredie KB,
FreireichEJ.Identification of risk groups for development of central
nervous system leukemia in adults with acute lymphocytic leukemia.
Blood 1988; 72: 1784-89 PMid:3052630
- Cortes J. Central nervous system involvement in adult acute lymphocytic leukemia. Hematol Oncol Clin North Am 2001; 15: 145-62 http://dx.doi.org/10.1016/S0889-8588(05)70203-3
- Mahmoud
HH, Rivera GK, Hancock ML Krance RA, Kun LE, Behm FG, et al. Low
leukocyte counts with blast cells in cerebrospinal fluid of children
with newly diagnosed acute lymphoblastic leukemia. N Engl J Med 1993;
329: 314-19 http://dx.doi.org/10.1056/NEJM199307293290504 PMid:8321259
- Smith
M, Arthur D, Camitta B, Carroll AJ, Crist W, Gaynon P, et al. Uniform
approach to risk classification and treatment assignment for children
with acute lymphoblastic leukemia. J Clin Oncol 1996;
14:18-24 PMid:8558195
- Gilchrist
GS, Tubergen DG, Sather HN, Coccia PF, O'Brien RT, Waskerwitz MJ, et
al. Low numbers of CSF blasts at diagnosis do not predict for the
development of CNS leukemia in children with intermediate-risk acute
lymphoblastic leukemia: a Childrens Cancer Group report. J Clin Oncol
1994; 12(12): 2594-2600 PMid:7989934
- Tubergen
DG, Cullen JW, Boyett JM, Gilchrist GS, O'Brien RT, Coccia PF et al.
Blasts in CSF with a normal cell count do not justify alteration of
therapy for acute lymphoblastic leukemia in remission: a Childrens
Cancer Group study. J Clin Oncol. 1994;12(2):273-8 PMid:8113836
- Burger
B, Zimmermann M, Mann G, Kuhl J, Loning L, Riehm H et al. Diagnosed
cerebrospinal fluid examination in children with acute lymphoblastic
leukemia: significante of low leukocyte counts with blasts or traumatic
lumbar puncture. J Clin Oncol 2003; 21: 184-88 http://dx.doi.org/10.1200/JCO.2003.04.096
- Glass
JP, Melamed M, Chernik NL, Posner JB. Malignant cells in cerebrospinal
fluid (CSF): the meaning of a positive CSF cytology. Neurology 1979;
29: 1369-75. http://dx.doi.org/10.1212/WNL.29.10.1369 PMid:573381
- Chamberlain
MC, Glantz M, Groves MD, Wilson WH. Diagnostic tools for neoplastic
meningitis: detecting disease, identifying patient risk, and
determining benefit of treatment. Semin Oncol 2009;36; S35-44 http://dx.doi.org/10.1053/j.seminoncol.2009.05.005 PMid:19660682
- Chamberlain MC. Leptomeningeal metastases: a review of evaluation and treatment. J Neuro Oncol 1998;37; 271-84 http://dx.doi.org/10.1023/A:1005976926058 PMid:9524085
- Grossman SA, Krabar MJ. Leptomeningeal carcinomatosis. Cancer Treat Rev 1999; 25(2): 103-19 http://dx.doi.org/10.1053/ctrv.1999.0119 PMid:10395835
- Chamberlain
MC, Nolan C, Abrey LE. Leukemic and lymphomatous meningitis: incidence,
prognosis and treatment. J Neuro Oncol 2005;75: 71-83 http://dx.doi.org/10.1007/s11060-004-8100-y PMid:16215818
- Chamberlain
MC, Sandy AD, Press GA. Leptomeningeal metastasis: A comparison of
gadolinium-enhanced MR and contrast-enhanced CT of the brain. Neurology
1990; 40: 435-38 http://dx.doi.org/10.1212/WNL.40.3_Part_1.435 PMid:2314584
- Zeiser
R, Burger JA, Bley TA, Windfuhr-Blum M, Schulte-Monting J, Behringer
DM. Clinical follow-up indicates differential accuracy of magnetic
resonance imaging and immunocytology of the cerebral spinal fluid for
the diagnosis of neoplastic meningitis-a single centre experience. Br J
Haematol. 2004; 124: 762-68 http://dx.doi.org/10.1111/j.1365-2141.2004.04853.x PMid:15009064
- Hegde
U, Filie A, Little RF, Janik JE, Grant N, Steinberg SM et al. High
incidence of occult leptomeningeal disease detected by flow cytometry
in newly diagnosed aggressive B-cell lymphoma at risk for central
nervous system involvement: the role of flow cytometry versus cytology.
Blood 2005; 105: 496-502 http://dx.doi.org/10.1182/blood-2004-05-1982 PMid:15358629
- Bromberg
JEC, Breems DA, Kraan J, Bikker G., van der Holt, Sillevis Smitt P, et
al. CSF flow cytometry greatly improves diagnostic accuracy in CNS
hematologic malignancies. Neurology 2007; 68: 1674-79 http://dx.doi.org/10.1212/01.wnl.0000261909.28915.83 PMid:17502548
- Kaplan
JG, DeSouza TG, Farkash A, Shafran B, Pack D, Rehman F, et
al.Leptomeningeal metastases: comparison of clinical features and
laboratory data of solid tumors, lymphomas and leukemias. J Neurooncol
1990; 9(3): 225-29 http://dx.doi.org/10.1007/BF02341153 PMid:2086737
- Craig F, Foon KA. Flow cytometricimmunophenotyping for hematologic neoplasms. Blood 2008; 111: 3941-67 http://dx.doi.org/10.1182/blood-2007-11-120535 PMid:18198345
- Quijano
S, Lopez A, Manuel Sancho J, Panizo C, Debén G, Castilla C et al.
Spanish Group for the Study of CNS disease in NHL. Identification of
leptomeningeal disease in aggressive B-cell non Hogkin's lymphoma:
improved sensitivity of flow cytometry. J Clin Oncol 2009; 27: 1462-69 http://dx.doi.org/10.1200/JCO.2008.17.7089 PMid:19224854
- de
Graaf MT, de Jongste AH, Kraan J, Boonstra JG, SillevisSmitt PA,
Gratama JW. Flow cytometric characterization of cerebrospinal fluid
cells.Cytometry B ClinCytom.2011;80(5):271-81. http://dx.doi.org/10.1002/cyto.b.20603 PMid:21567940
- Di
Noto R, Scalia G, Abate G Gorrese M, Pascariello C, Raia M et al.
Critical role of multidimensional flow cytometry in detecting occult
leptomeningeal disease in newly diagnosed aggressive B-cell lymphomas.
Leuk Res 2008: 32: 1196-99 http://dx.doi.org/10.1016/j.leukres.2007.12.016 PMid:18262645
- Subira
D, Castanon S, Roman A, Aceituno E, Jimenez-Garofano C, Jimenez A et
al. Flow cytometry and the study of central nervous disease in patients
with acute leukemia. Br J Hematol 2001; 112: 381-84 http://dx.doi.org/10.1046/j.1365-2141.2001.02505.x
- Craig
FE, Ohori NP, Gorrill TS, Swerdlow SH. Flow cytometricimmunophenotyping
of cerebrospinal fluid specimens. Am J Clin Pathol 2011; 135:22-35 http://dx.doi.org/10.1309/AJCPANA7ER1ABMZI PMid:21173121
- Buccisano
F, Maurillo L, Del Principe MI, Del Poeta G, Sconocchia G, Lo-Coco F,
et al. Prognostic and therapeutic implications of minimal residual
disease detection in acute myeloid leukemia. Blood 2012; 119: 332-41 http://dx.doi.org/10.1182/blood-2011-08-363291 PMid:22039260
- Roma
A, Garcia A, Avagnina A, Rescia C, Elsner B. Lymphoid and myeloid
neoplasms involving cerebrospinal fluid: comparison of morphologic
examination and imunophenotyping by flow cytometry. DiagnCytopathol
2002; 27: 271-75 http://dx.doi.org/10.1002/dc.10190 PMid:12411991
- Nuckel
H, Novotny JR, NoppeneyR,Savidou I, Duhrsen. Detection of malignant
haematopoietic cells in the cerebrospinal fluid by conventional
cytology and flow cytometry. Clin Lab Haem. 2006; 28: 22-29 http://dx.doi.org/10.1111/j.1365-2257.2006.00741.x PMid:16430456
- Sayed
D, Badrawy H, Ali AM, Shaker SImmunophenotyping.and immunoglobulin
heavy chain gene rearrangement analysis in cerebrospinal fluid of
pediatric patients with acute lymphoblastic leukemia.Leuk Res.
2009;33(5):655-61 http://dx.doi.org/10.1016/j.leukres.2008.09.033 PMid:18996593
- Mitri
Z, Siddiqui MT, Rassi EF, Holden JT, Heffner LT, Langston A et al.
Sensitivity and specificity of cerebral fluid flow cytometry for the
diagnosis of leukemic meningitis in acute lymphoblastic
leukemia/lymphoma. Leuk Lymphoma 2014; 55(7): 1498-500 http://dx.doi.org/10.3109/10428194.2013.852667 PMid:24134778
- Del
Principe MI, Buccisano F, Cefalo M, Maurillo L, Di Caprio L, Di Piazza
F, et al. High sensitivity of flow cytometry improbe detection of
occult leptomeningeal disease in acute lymphoblastic leukemia and
lymphoblastic lymphoma. Ann Hematol 2014; 93(9):1509-13 http://dx.doi.org/10.1007/s00277-014-2080-6 PMid:24752416
- Martinez-Laperche
C, Gomez-Garcia AM, Lassaletta A, Moscardo C, Vivanco J, Molina J et
al. Detection of occult cerebrospinal fluid involvement during
maintenance therapy identifies a group of children with acute
lymphoblastic leukemia at high risk for relapse. Am J Hematol 2013;
88(5): 360-65 http://dx.doi.org/10.1002/ajh.23407 PMid:23468276
- Benevolo
G, Stacchini A, Spina M, Ferreri AJM, Arras M; Bellio L, et al. Final
results of a multi center trial addressing role of CSF flow cytometric
analysis in NHL patients at high risk for CNS dissemination. Blood
2012; 120: 3222-28 http://dx.doi.org/10.1182/blood-2012-04-423095 PMid:22927246
- Wilson
W, Bromberg J, Stetler-Stevenson M, Steinberg S, Martin-Martin L, Muniz
C et al. Detection and outcome of occult leptomeningeal disease in
diffuse large B-cell lymphoma and Burkitt Lymphoma. Haematologica
2014;99(7):1228-35 http://dx.doi.org/10.3324/haematol.2013.101741 PMid:24727817 PMCid:PMC4077085
- Scrideli
CA, Queiroz RP, Takayanagui OM, Bernardes JE, Melo EV, Tone LG.
Molecular diagnosis of leukemic cerebrospinal fluid cells in children
with newly diagnosed acute lymphoblastic leukemia. Haematologica 2004,
89(8): 1013-18 PMid:15339689
- Mu-iz
C, Martìn-Martìn L, López A, Sánchez-González B, Salar A, Almeida J et
alContribution of cerebrospinal fluid sCD19 levels to the detection of
CNS lymphoma and its impact on disease outcome. Blood 2014; 123 (12):
1864-9 http://dx.doi.org/10.1182/blood-2013-11-537993 PMid:24501214
- Gökbuget N, Hoelzer D. Meningeosisleukaemica in adult lymphoblastic leukaemia. J Neurooncol 1998; 38: 167-80 http://dx.doi.org/10.1023/A:1005963732481 PMid:9696368
- Morra
E, Lazzarino M, Inverdadi D, Brusamolino E, Orlandi E,
CanevariA.Systemic high-dose araC for the treatment of meningeal
leukemia in adult acute lymphoblastic leukemia and non-Hodgkin's
lymphoma. J Clin Oncol 1986; 4: 1207-11 PMid:3461134
- Cortes
J, O'Brien SM, Pierce S, Keating MJ, Freireich EJ, Kantarjian HHM. The
value of high-dose systemic chemotherapy and intrathecal therapy for
central nervous system prophylaxis in different risk groups of adult
acute lymphoblastic leukemia. Blood 1995; 86:
2091-2097 PMid:7662956
- Bostrom
BC, Sensel MR, Sather HN, Gaynon PS, La MK, Johnston K, Erdmann GR,
Gold S, Children's Cancer Group.Dexamethasone versus prednisone and
daily oral versus weekly intravenous mercaptopurine for patients with
standard-risk acute lymphoblastic leukemia: a report from the
Children's Cancer Group.Blood. 2003; 101(10):3809-17 http://dx.doi.org/10.1182/blood-2002-08-2454 PMid:12531809
- Jones
B1, Freeman AI, Shuster JJ, Jacquillat C, Weil M, Pochedly C, Sinks L,
Chevalier L, Maurer HM, Koch K, et al. Lower incidence of meningeal
leukemia when prednisone is replaced by dexamethasone in the treatment
of acute lymphocytic leukemia. Med Pediatr Oncol.1991;19(4):269-75 http://dx.doi.org/10.1002/mpo.2950190411 PMid:2056971
- Annino
L, Vegna ML, Camera A Specchia G, Visani G, Fioritoni G et al. GIMEMA
Group. Treatment of adult acute lymphoblastic leukemia (ALL): long-term
follow-up of the GIMEMA ALL 0288 randomized study. Blood 2002; 99:
863-71 http://dx.doi.org/10.1182/blood.V99.3.863 PMid:11806988
- Relling
MV, Mahmoud HH, Pui CH Sandlund JT, Rivera GK, Ribeiro RC, et
al.Etoposide achieves potentially cytotoxic concentrations in CSF of
children with acute lymphoblastic leukemia.J Clin Oncol.
1996;14(2):399-404.PMid:8636749
- Zimm
S, Ettinger LJ, Holcenberg JS KamenBA, Vietti TJ, Belasco J, et al.
Phase I and clinical pharmacological study of mercaptopurine
administrated as a prolonged intravenous infusion. Cancer Res 1985; 45:
1869-73 PMid:4038917
- Riccardi
R, Holcenberg JS, Glaubiger DL, Wood JH, Poplack DG. L-asparaginase
pharmacokinetics and asparaginase levels in cerebrospinal fluid of
rhesus monkeys and humans. Cancer Res 1981; 41:
4554-8 PMid:6895481
- Moghrabi
A, Levy DE, Asselin B, Barr R, Clavell L, Hurwitz C, et al.Results of
the Dana-Farber Cancer Institute ALL Consortium Protocol 95-01 for
children with acute lymphoblastic leukemia.Blood. 2007;109(3):896-904 http://dx.doi.org/10.1182/blood-2006-06-027714 PMid:17003366 PMCid:PMC1785142
- Blasberg
RG, Patlak C, Fenstermacher JD. Intrathecal chemotherapy: brain tissue
profiles after ventriculocisternal perfusion.J Pharmacol ExpTher. 1975;
195(1):73-83 PMid:810575
- Sancho
JM, Ribera JM, Oriol A Hernandez-Rivas JM, Rivas C, Bethencourt C, et
al. Programa para el Estudio y Tratamiento de Hemopatias Malignas
Group. Central nervous system recurrence in adult patients with acute
lymphoblastic leukemia: frequency and prognosis in 467 patients without
cranial irradiation for prophylaxis. Cancer 2006; 106 2540-6 http://dx.doi.org/10.1002/cncr.21948 PMid:16700036
- Chabner
BA. Cytidine analogues. In Chabner BA, Longo DL. (eds) Cancer
chemotherapy and biotherapy: principles and practice, 2nd ed.
Philadelphia, PA: Lippincott-Raven 1996; 213-33
- Kim
S, Khatibi S, Howell SB, McCully C, Balis FM, Poplack DG. Prolongation
of drug exposure in cerebrospinal fluid by encapsulation into
DepoFoam.Cancer Res.
1993;53(7):1596-1598. PMid:8453629
- Bassan
R, Masciulli A, Intermesoli T, Audisio E, Cattaneo C, Pogliani EM, et
al. Phase II randomized trial of radiation-free central nervous system
comparing intratheca triple therapy with liposomal cytarabine
(DepoCyte) in adult acute lymphoblastic leukemia. Abstract 3901.
Presented at the 55th Congress of American Society of Hematology. New
Orleans, LA, December 7-10, 2013
- Goekbuget
N, Beck J, Brueggemann M, Burmeister T, Buss EC,Frickhofen N, et al.
Moderate intensive chemotherapy including CNS-prophylaxis with
liposomal cytarabine is feasible and effective in older patients with
Ph-negative acute lymphoblastic leukemia (ALL): results of prospective
trial from German Multicenter Study Group for adult ALL
(GMALL).Abstract 1493. Presented at the 54th Congress of American
Society of Hematology. Atlanta, GA, December 8-11, 2012
- Simone
JAur RJA, Hustu HO, Pinked D. "Total therapy" studies of acute
lymphocytic leukemia in children: current results and prospects for
care. Cancer 1972; 30: 1488-94 http://dx.doi.org/10.1002/1097-0142(197212)30:6<1488::AID-CNCR2820300612>3.0.CO;2-D
- Pui
C-H, Dodge RK, Look AT George SL, Rivera GK, Abromowitch M et al. Risk
of adverse events in children completing treatment for acute
lymphoblastic leukemia: St. Jude total stdies VIII, IX, X. J Clin Oncol
1991; 9: 1341-7 PMid:2072137
- Omura
GA, Moffitt S, Vogler R, Salter MM. Combination chemotherapy of adult
acute lymphoblastic leukemia with randomized central nervous system
prophylaxis. Blood 1980; 55 (2): 199-204 PMid:6928104
- Sanders
KE, Ha CS, Cortes-Franco JE, Koller CA, Kantarjian HM, Cox JD.The role
of craniospinal irradiation in adults with a central nervous system
recurrence of leukemia.Cancer. 2004;100(10):2176-80 http://dx.doi.org/10.1002/cncr.20280 PMid:15139061
- Durrant
IJ, Prentice HG, Richards SM. Intensification of treatment for adults
with acute lymphoblastic leukaemia: results of U.K. Medical Research
Council randomized trial UKALL XA. Medical Research Council Working
Party on Leukaemia in Adults.Br J Haematol. 1997;99(1):84-92. http://dx.doi.org/10.1046/j.1365-2141.1997.3613175.x PMid:9359507
- Stock
W, Johnson J, Stone RM, Kolitz JE, Powell BL, Wetzler M, et al. Dose
intensification of daunorubicin and cytarabine during treatment of
Adult Acute Lymphoblastic Leukemia. Result of Cancer and Leukemia Group
B Study 19802. Cancer 2013; 119(1): 90-8 http://dx.doi.org/10.1002/cncr.27617 PMid:22744771
- Phuphanich
S, Maria B, Braeckman R, Chamberlain M. A pharmacokinetic study of
intra-CSF administered encapsulated cytarabine (DepoCyt) for the
treatment of neoplastic meningitis in patients with leukemia, lymphoma,
or solid tumors as part of a phase III study. J Neurooncol.
2007;81(2):201-8 http://dx.doi.org/10.1007/s11060-006-9218-x PMid:16941075
- Bomgaars
L, Geyer JR, Franklin J, Dahl G, Park J, WinickNJ, et al. Phase I trial
of intrathecal liposomal cytarabine in children with neoplastic
meningitis.J ClinOncol. 2004;22(19):3916-21 http://dx.doi.org/10.1200/JCO.2004.01.046 PMid:15459213
- Jabbour
E, O'Brien S, Kantarjian H, Garcia-Manero G, Ferrajoli A, Ravandi F, et
al. Neurologic complications associated with intrathecal liposomal
cytarabine given prophylactically in combination with high-dose
methotrexate and cytarabine to patients with acute lymphoblastic
leukemia. Blood 2007; 109: 3214-8 http://dx.doi.org/10.1182/blood-2006-08-043646 PMid:17209054
- Gökbuget
N, Hartog CM, Bassan R, Derigs HG, Dombret H, Greil R, et al. German
Multicenter Study Group for Adult ALL and the European Working Group
for Adult ALL Liposomal cytarabine is effective and tolerable in the
treatment of central nervous system relapse of acute lymphoblastic
leukemia and very aggressive lymphoma. Haematologica. 2011;
96(2):238-44 http://dx.doi.org/10.3324/haematol.2010.028092 PMid:20952517 PMCid:PMC3031691
- Leis
JF, Stepan DE, Curtin PT, Ford JM, Peng B, SchubachS,et al. Central
nervous system failure in patients with chronic myelogenous leukemia
lymphoid blast crisis and Philadelphia chromosome positive acute
lymphoblastic leukemia treated with imatinib (STI-571).Leuk Lymphoma.
2004;45(4):695-8 http://dx.doi.org/10.1080/10428190310001625728 PMid:15160941
- Takayama
N1, Sato N, O'Brien SG, Ikeda Y, Okamoto S. Imatinib mesylate has
limited activity against the central nervous system involvement of
Philadelphia chromosome-positive acute lymphoblastic leukaemia due to
poor penetration into cerebrospinal fluid. Br J Haematol.
2002;119(1):106-8. http://dx.doi.org/10.1046/j.1365-2141.2002.03881.x
- Hochhaus
A, Kantarjian HM, Baccarani M, Lipton JH, Apperley JF, Druker BJ, et
al.. Dasatinib induces notable hematologic and cytogenetic responses in
chronic-phase chronic myeloid leukemia after failure of imatinib
therapy. Blood. 2007;109(6):2303-9 http://dx.doi.org/10.1182/blood-2006-09-047266 PMid:17138817
- Porkka
K, Koskenvesa P, Lundán T, Rimpiläinen J, Mustjoki S, Smykla R, et al.
Dasatinib crosses the blood-brain barrier and is an efficient therapy
for central nervous system Philadelphia chromosome-positive
leukemia.Blood. 2008;112(4):1005-12 http://dx.doi.org/10.1182/blood-2008-02-140665 PMid:18477770
- Reinwald
M, Schleyer E, Kiewe P, Blau IW, Burmeister T, Pursche SM et al.
Efficacy and pharmacologic data of second-generation tyrosine
kinase inhibitor nilotinib in BCR-ABL-positive leukemia patients with
central nervous system relapse after allogeneic stem cell
transplantation. Biomed Res Int. 2014; Epub 2014 Jun 15.
- Quintás-Cardama
A, Han X, Kantarjian H, Cortes J.Tyrosine kinase inhibitor-induced
platelet dysfunction in patients with chronic myeloid leukemia Blood.
2009 Jul 9;114(2):261-3 http://dx.doi.org/10.1182/blood-2008-09-180604 PMid:19414863 PMCid:PMC3952950
- Patel
SB, Gojo I, Tidwell ML, Sausville EA, Baer MR. Subdural hematomas in
patients with Philadelphia chromosome-positive acute lymphoblastic
leukemia receiving imatinib mesylate in conjunction with systemic and
intrathecal chemotherapy. Leuk Lymphoma 2011; 52(7): 1211-4 http://dx.doi.org/10.3109/10428194.2011.566950 PMid:21534873
- Maus
M, Grupp SA, Porter DL, June CH. Antibody-modified T cells: CARs take
the front seat for hematologic malignancies. Blood 2004; 123(17):
2625-35 http://dx.doi.org/10.1182/blood-2013-11-492231 PMid:24578504
- Grupp
SA, Kalos M, Barrett D, Aplenc R, Porter DL, Rheingold SR, et al
.Chimeric antigen receptor-modified T cells for acute lymphoid
leukemia.N Engl J Med. 2013;368(16):1509-18 http://dx.doi.org/10.1056/NEJMoa1215134 PMid:23527958 PMCid:PMC4058440
- Fisher
DT, Chen Q, Skitzki JJ, Muhitch JB, Zhou L, Appenheimer MM, et al. IL-6
trans-signaling licenses mouse and human tumor microvascular gateways
for trafficking of cytotoxic T cells.J ClinInvest. 2011;121(10):3846-59
http://dx.doi.org/10.1172/JCI44952 PMid:21926464 PMCid:PMC3195455
- Lee
III DW, Shah NN, Stetler-Stevenson M, Sabatino M, Delbrook RN, Richards
K, et la. Abstract 68. Anti-CD19 chimeric antigen receptor (CAR) T
cells produce complete responses with acceptable toxicity but without
chronic B-cell aplasia in children with relapsed or refractory acute
lymphoblastic leukemia (ALL) even after allogeneic hematopoietic stem
cell transplantation. Presented at the 55th Congress of American
Society of Hematology. New Orleans, LA, December 7-10, 2013
- Maude
SL, Frey N, Shaw PA, Aplenc R, Barrett DM, Bunin NJ. Chimeric antigen
receptor T cells for substained remissions in leukemia. N Engl J Med
2014; 371 (16): 1507-17 http://dx.doi.org/10.1056/NEJMoa1407222 PMid:25317870
[TOP]