Received: September 6, 2014
Accepted: November 28, 2014
Mediterr J Hematol Infect Dis 2015, 7(1): e2015008, DOI 10.4084/MJHID.2015.008
This article is available on PDF format at:

Aneesh Basheer1, Somanath Padhi2*, Vinoth Boopathy3, Saumyaranjan Mallick4, Shashikala Nair5, Renu G’Boy Varghese2 and Reba Kanungo5
1Departments of General Medicine, Pondicherry Institute of Medical Sciences, Puducherry, India.
2Department of Pathology, Pondicherry Institute of Medical Sciences, Puducherry, India.
3Department of Gastroenterology, Pondicherry Institute of Medical Sciences, Puducherry, India.
4Department of Pathology, All India Institute of Medical Sciences, New Delhi, India.
5Department of Microbiology, Pondicherry Institute of Medical Sciences, Puducherry, India.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Background: Hemophagocytic
lymphohistiocytosis (HLH) is an uncommon, potentially fatal,
hyperinflammatory syndrome that may rarely complicate the clinical
course of Orientia tsutsugamushi disease (scrub typhus). Methods: Here we describe the clinicopathological features, laboratory parameters, management, and outcome of three adult patients (1 female, 2 males) with scrub typhus associated HLH from a tertiary center. A brief and concise review of international literature on the topic was also added. Results: All three patients satisfied the HLH-2004 diagnostic criteria; one had multi-organ dysfunction with very high ferritin level (>30,000 ng/ml), and all had a dramatic recovery following doxycyclin therapy. Literature review from January 1990 to March 2014 revealed that scrub typhus associated HLH were reported in 21 patients, mostly from the scrub endemic countries of the world. These included 11 females and 10 males with a mean age of 35 years (range; 8 months to 81 years). Fifteen of 17 patients (where data were available) had a favorable outcome following early serological diagnosis and initiation of definitive antibiotic therapy with (N=6) or without (N=9) immunosuppressive/immunomodulator therapy. Mutation analysis for primary HLH was performed in one patient only, and HLH-2004 protocol was used in two patients. Conclusion: We suggest that HLH should be considered in severe cases of scrub typhus especially if associated with cytopenia (s), liver dysfunction, and coagulation abnormalities. Further studies are required to understand whether an immunosuppressive and/or immunomodulator therapy could be beneficial in those patients who remain unresponsive to definitive antibiotic therapy. |
Introduction
Hemophagocytic lymphohistiocytosis (HLH) is a syndrome, often fatal,
of exacerbated but ineffective inflammatory response, characterized by
excessive macrophage and T-cell activation as well as impairment of the
ability of natural killer (NK) cell and cytotoxic T lymphocytes to kill
the target cells. This results in uncontrolled histiocytic phagocytosis
of mature blood elements and their precursors throughout the
reticuloendothelial organs; and associated cytokine-mediated multiorgan
dysfunction.[1,2] Primary or familial HLH
appears to have a genetic basis, whereas secondary or acquired HLH may
be associated with infections (commonly Epstein Barr Virus, bacteria,
Rickettsia, etc), hematological malignancies (mostly T/NK cell
leukemias/lymphomas), rheumatological/autoimmune disorders (so-called
macrophage activation syndrome), etc.[3-5] The
diagnosis is established by fulfilling one of the following HLH-2004
criteria: i) positive family history or molecular diagnosis consistent
with HLH (mutations of PRF, SAP, or MUNC13-4 genes), ii) any five out
of the following eight criteria: prolonged fever, unexplained
progressive cytopenias involving at least 2 cell lines (hemoglobin ≤ 90
g/L, platelet count ≤ 100 x 109/L, absolute neutrophil count < 1 x 109/L),
splenomegaly, hyperferritinemia (≥ 500ng/mL), fasting
hypertriglyceridemia (≥ 265 mg/dL) or hypofibrinogenemia (≤ 1.5 g/L),
histiocytic hemophagocytosis in bone marrow, liver, spleen, or lymph
nodes without evidence of malignancy, low or absent NK cell
cytotoxicity, and elevated soluble CD25 levels (≥ 2400 IU/mL of
interleukin-2Rα chain).[6]
In this manuscript, we
describe three adult patients with scrub typhus associated HLH from a
tertiary care center in South India. We also present a brief concise
review of international literature regarding scrub typhus associated
HLH in relation to the clinicopathological characteristics,
immunopathology, and therapeutic outcome.
Materials and Methods
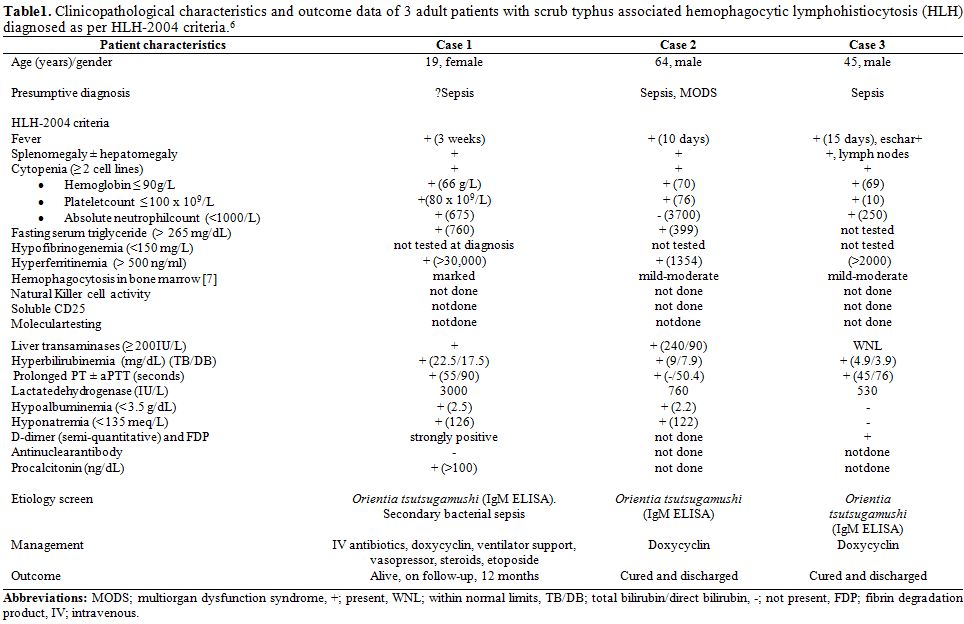 |
Table 1. Clinicopathological characteristics and outcome data of 3 adult patients with scrub typhus associated hemophagocytic lymphohistiocytosis (HLH) diagnosed as per HLH-2004 criteria.[6] |
Review of International Literature
A systematic search of HLH that complicated the course of scrub
typhus over last 24 years (January 1990 to March 2014) was done by the
search engine of PubMed, PubMed Central, Medline, and Directory of Open
Access Journal databases. The following terminologies were used in the
data search; hemophagocytic
lymphohistiocytosis/hemophagocytosis/erythrophagocytosis/ macrophage
activation syndrome and scrub typhus/Orientia tsutsugamushi/tsutsugamushi
disease/Rickettsial disease; and references of all articles were
cross-checked for relevant articles. Review showed 18 papers describing
21 cases of scrub typhus associated HLH around the world.[5,8-25]
Cascio et al, in 2011, reported a case of HLH (negative for perforin 1,
MUNC 13-4, SYNTAXIN 11 mutations) in a 5 year old Italian male child
secondary to Rickettsia conorii (Mediterranean Spotted Fever, MSF); and
reviewed another 16 cases of rickettsia associated HLH till that year
[7 due to scrub typhus, 5 due to MSF, and 4 due to human monocytic
ehrlichiosis (HME)].[5] In 4 of 21 cases of scrub typhus (2 from Taiwan, two from Japan), complete articles were not fully accessible for study.[19,22,25] Clinical and laboratory data available have been put in a tabular format (Table 2).
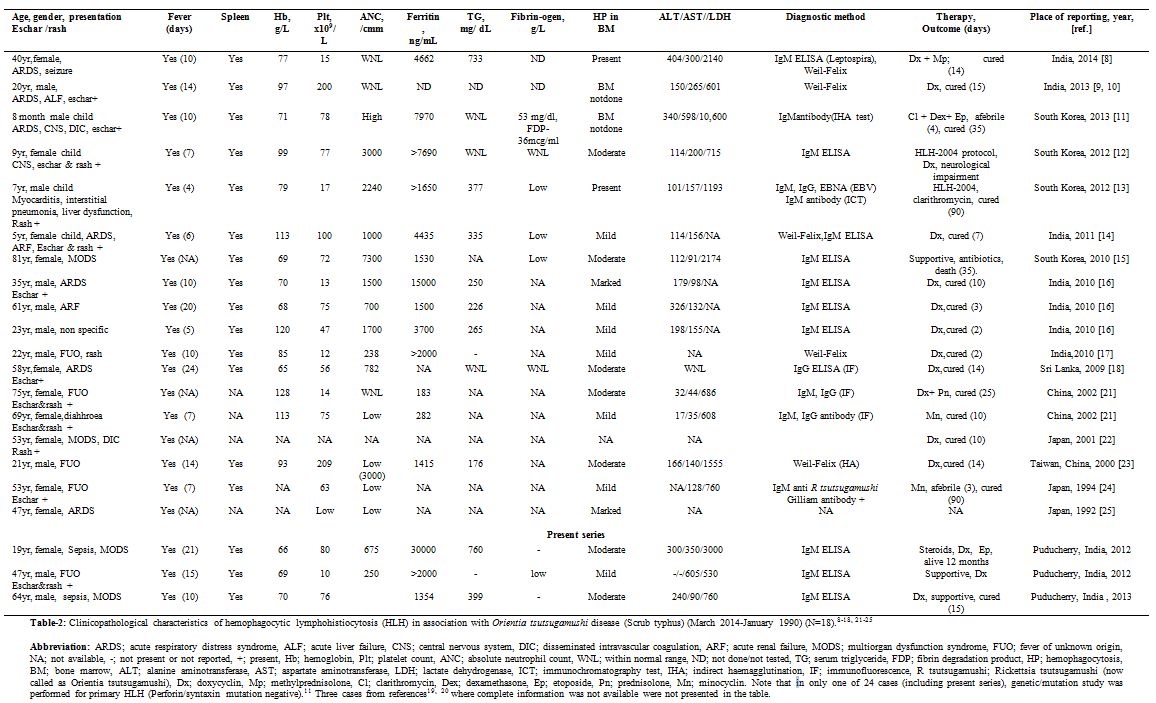 |
Table 2. Clinicopathological characteristics of hemophagocytic lymphohistiocytosis (HLH) in association with Orientia tsutsugamushi disease (Scrub typhus) (March 2014-January 1990) (N=18).[8-18,21-25] |
Result and Discussion
Scrub typhus, also known as tsutsugamushi disease, is a
chigger-borne zoonosis which is of great public health importance in
tropical Asia and the islands of the Western Pacific Ocean. This
infection or its etiologic agent (O. tsutsugamushi)
has been documented within an endemic triangle with apices in the
Primorje region of the Russian Far East, northern Australia, and
Afghanistan.[26] Scrub typhus is an acute febrile
illness which results from the bite of infected larval form of mite,
called chigger, in endemic areas. Following an incubation period of 7
to 10 days, the nonspecific prodrome of pyrexia, skin rash, myalgia,
gastrointestinal disturbances, and lymphadenopathy starts. Although not
consistently seen, the most pathognomonic sign of scrub typhus is an eschar that develops at the site of mite bite. During human infection, O. tsutsugamushi,
being a rickettsial organism, selectively targets the vascular
endothelial cells of the small to medium-sized blood vessels. However,
it can also invade underlying tissues such as smooth muscle cells,
perivascular macrophages, and monocytes. Consequently, widespread
vasculitis/perivasculitis is the hallmark pathophysiologic mechanism
implicated in multiorgan dysfunction syndrome (MODS) in patients with
severe infections.[5,26]
The
main pathophysiologic characteristic of HLH is exacerbated but
deregulated Th1 cell-mediated immune response against an intracellular
pathogen, macrophage hyperactivity, widespread hemophagocytosis, and
hypercytokinemia leading to multi-organ dysfunction. This results due
to impaired or suppressed function of cytotoxic T cells and NK cells to
effectively clear the antigenic stimulus and thus turn off the
inflammatory response.[1] The severity of rickettsial diseases varies with the causative organism and the host. Some rickettsial species such as Rickettsia rickettsii, Rickettsia prowazekii, and O. tsutsugamushi
often cause more severe disease. Host factors like old age, alcoholism,
diabetes mellitus, liver and respiratory diseases, and
glucose-6-phosphate dehydrogenase deficiency have been associated with
more severe disease.[5] Experimental studies have
shown that human cells are capable of controlling rickettsial
infections intracellularly, by one or combination of three mechanisms
involving nitric oxide synthesis, hydrogen peroxide production, and
tryptophan degradation. These mechanisms involve a complex interaction
of CD4+ and CD8+
T lymphocytes, macrophages, NK cells, B lymphocytes, antibodies, and
cytokines. Inflammatory responses of humans appear to coincide with the
disease severity in scrub typhus, and the cytotoxic T-cell mediated
macrophage over activity may induce hemophagocytosis in susceptible
individuals.[27] This hypothesis has been further
substantiated by the observation of increased serum levels of IFN- γ,
M-CSF and TNF-α in patient with scrub typhus in several studies.[28]
A
concise review on clinicopathological characteristics of all reported
cases of scrub typhus associated HLH till March 2014 is presented in Table 2.
There were 21 reported cases with HLH, complicating the course of scrub
typhus (7 from India, 5 from China, 4 from Japan, 4 from South Korea,
and 1 from Sri Lanka).[5,8-25] These
included 11 females and 10 males, with a mean age of 35 years (range; 8
months to 81 years); and none of these cases had obvious underlying
co-morbidities. All patients, 18/18, in whom data were available,
presented with acute febrile illness (mean duration; 10 days, range: 4
to 24 days): similarly all cases reported (14/14) had
hepatosplenomegaly with or without regional lymphadenopathy. A
characteristic eschar was signaled in 9/18 (50%) patients and seven of
18 (39%) had ARDS, 3 (16.7%) had neurological manifestations, 2 (11%)
had acute renal failure, 2 (11%) had DIC with MODS, 2 (11%) had at
onset acute hepatic failure. One had co-existent leptospirosis,[8] and one had myocarditis, interstitial pneumonia, and reactivation of EBV infection.[13]
Eleven of 18 patients (61%), in whom data were available, had
bicytopenia; 4/18 (22%) had pancytopenia, and 6/13 (37.5%) had
coagulation abnormalities. Histiocytic hemophagocytosis was reported in
bone marrow of all 16 examined patients (100%). Hemophagocytosis was of
mild to moderate intensity in 14 (87.5%) patients whereas appeared
marked in only two patients. This was reflected by modest elevation of
serum ferritin level (N=13/21) (mean; 3320 ng/ml, range; 1415-15,000
ng/ml). Molecular analysis for
primary HLH such as mutation of perforin and SYNTAXIN gene was
performed in one patient (8 month male child) only.[11] A recent
study on pediatric HLH patients (N=38; 20 primary HLH, 18 secondary
HLH) reported that hyperbilirubinemia with cholestasis was highly
suggestive of primary HLH; whereas high C-reactive protein levels was
more in favor of a secondary HLH. The other parameters such as
ferritin, triglyceride, PT, APTT were not statistically different
between the two groups.[29] All the 3 patients in our
series satisfied the HLH-2004 criteria and had hyperbilirubinemia
(marked in case 1) with biochemical evidence of cholestasis (direct
bilirubin fraction greater than indirect), two had raised transaminases
and all three had coagulation abnormality in the form of prolonged PT,
APTT, or both (Table 1). One
patient (case 1) had “sky high” ferritin levels (>30,000 ng/ml),
high procalcitonin levels suggestive of sepsis, and evidence of marked
degree of histiocytic hemophagocytosis in bone marrow. During the
clinical course, she progressed to DIC with hypofibrinogenemia leading
to MODS.
Serological diagnosis of scrub typhus is usually possible
after 5 to 10 days following onset of symptoms. Conventionally,
Weil-Felix test based on heterophile antigen of Proteus Vulgaris (OX-2, and OX-19) and Proteus mirabilis (OX-K) has been used widely. An agglutinating titer of >320 with OX-K is suggestive of scrub typhus.[30] However, several Indian studies have shown a lower cut-off titer at ≥ 80 to indicate a possible infection with O. tsutsugamushi, thus making the test even more non-specific.[31,32]
Poor sensitivity and specificity of Weil-Felix is well established.
Recently, IgM ELISA and IgM Capture ELISA techniques have shown better
predictive value as diagnostic tests in scrub typhus. PCR-based tests
have overcome the drawbacks of serological tests, in early detection
using specific primers;[33] and multiplex PCR has further improved diagnostic criteria in endemic areas.[34]
In all the reported cases of scrub typhus associated HLH, the diagnosis
of rickettsial disease was serologically confirmed. The following
serological methods were used for the diagnosis: Weil-Felix (N=5), IgM
ELISA (N=6), IgM antibodies by indirect haemagglutination (IHA) (N=1),
antibody titres by immunofluorescence (N=3), IgM antibody by
immunochromatography (N=1), and IgM anti O. tsutsugamushi Gilliam antibody (N=1).
Scrub
typhus responds more readily to antibiotics than other rickettsial
diseases, with most patients becoming afebrile within 24 to 36 hours
after beginning antibiotic therapy. A recent study by Japanese group
had shown that age was an independent risk factor for mortality;
furthermore patients with ≥ 2 days delay in treatment with
tetracyclines had a significantly higher risk of complications compared
to those without delay.[35] In another study from
South Korea, factors such as old age, presence of co-morbidities, and
high serum osteopontin (>100ng/ml) were important risk factors of
disease severity; though delay in treatment and strain type (Boryong,
Taguchi, or Kanda/Kawasaki) did not contribute to disease severity.[36]
Therapeutic and follow-up data were available In 17 patients with scrub
typhus associated HLH, ten of them received oral antibiotics in the
form of doxycyclin and/or clarithromycin/minocyclin; six patients
received immunotherapy in addition to oral antibiotic therapy (two of
them used HLH-2004),[12,13] and one patient refused any definitive therapy.[15] Barring two patients (one with residual neurological impairment,[12] and other with fatal outcome,[15] all 15 had a dramatic recovery from their illness without any residual impairment.
Though
the HLH protocol has been well established in the management of primary
HLH, its utility in the setting of secondary HLH has been
controversial.[2] High ferritin level has been
reported to be a diagnostic and prognostic marker in patients with HLH,
and a rapid rate of fall of ferritin levels following therapy
initiation associated with decreased mortality.[37]
However, Park et al. in their cohort of 23 patients with secondary HLH
found that high fibrinogen at the time of diagnosis, not the rate of
decline in ferritin, was associated with prolonged survival.
Furthermore, in patients with severe disease and/or associated sepsis
or multiple organ failure at the time of diagnosis, it may be difficult
to use cytotoxic agents such as etoposide. In such circumstances,
immunosuppression with corticosteroids and/or cyclosporine remains the
foundation of early management as it can control systemic inflammation.[38]
In view of the limited number of cases of HLH at our institute;
etoposide has not been widely used; hence limiting our experience. A
very high ferritin (>30,000 ng/ml), in conjunction with other
criteria, was highly characteristic of HLH in one of our patients (case
1). During the course of her illness, she developed MODS secondary to
sepsis and DIC (prolonged PT, aPTT, and increased fibrin degradation
product) (Table 1). She was
managed initially with vasopressor drugs, high-dose corticosteroids,
and intravenous broad-spectrum antibiotics. Doxycyclin was added
following the serological diagnosis of scrub typhus. Once her clinical
conditions improved, etoposide was added in consultation with
hematologist; however, it was later withdrawn after restoration of
normal hematological parameters.
Summary
HLH though rare, should be considered in severe cases of scrub typhus especially if associated with cytopenias, liver dysfunction, and coagulation abnormalities. Furthermore, wherever possible, a diagnosis of primary HLH should always be excluded in these cases by appropriate mutation analysis studies. As observed in our three patients and supported by available literature, early diagnosis and initiation of definitive antibiotic therapy may completely reverse the clinical course of the disease. Further studies are needed to understand whether an immunosuppressive and/or immunomodulator therapy such as treatment with corticosteroids, etoposide or cyclosporine could be beneficial in those cases which do not respond promptly to tetracycline therapy.
Author Contribution
References

[TOP]