Received: August 20, 2014
Accepted: December 12, 2014
Mediterr J Hematol Infect Dis 2015, 7(1): e2015009, DOI 10.4084/MJHID.2015.009
This article is available on PDF format at:

Adel A Hagag1 and Nahla A Nosair2
1 Pediatric Department, Faculty of Medicine, Tanta University, Egypt.
2 Clinical Pathology Department, Faculty of Medicine, Tanta University, Egypt.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Background: Neuropilins
are transmembrane glycoproteins that act as receptors for vascular
endothelial growth factors and are involved in the process of tumor
angiogenesis. Objective: The aim of this work was to study the
prognostic value of Neuropilin-1 (NRP-1) expression in Egyptian
children with B-lineage acute lymphoblastic leukemia (ALL). Patients and methods: This study was conducted on fifty children with newly diagnosed B-lineage ALL, admitted to Oncology Unit, Pediatric Department, Tanta University Hospitals in the period from August 2010 to March 2014. This series included 32 males and 18 females with ages ranging from 3-17 years and a mean value of 9 ± 3.5 years. Twenty healthy children, age and sex matched, were also included in this study as a control group. For all patients, the following examens were done: Bone marrow aspiration, cytochemistry, immunophenotyping and estimation of Neuropilin-1 expression on blast cells by flow cytometry. Results: The present study revealed highly significant differences in Neuropilin-1 expression between B-lineage ALL lymphoblasts and control lymphocytes. A significant higher Neuropilin-1 expression was found in pre-B ALL (74.04%) compared with early pre-B (23.55%). Neuropilin-1 positive expression was associated with significantly higher white blood cells count (Mean = 69.3±18.53 x103/mm3 versus 32.5±11.64 x103/mm3 and p=0.003), bone marrow blasts percentage (Mean=76.12±21.4 % versus 41.2±19.71% and p= 0.003), serum lactate dehydrogenase levels (Mean=1992.2 ± 58.6 unit/L versus 955.1± 234.7 unit/L and p=0.001) at diagnosis compared with negative Neuropilin-1 expression. The levels of Neuropilin-1 on BM blasts at diagnosis were higher in patients who subsequently relapsed (Mean=53.8 ± 27.1) or later died (Mean=81.51 ± 9.94) during the period of follow-up compared to those who achieved and maintained complete remission (Mean=18.17 ± 10.4) with p value of 0.001. Furthermore, patients with higher Neuropilin-1 expression had significantly shorter overall survival (Median 27.99 months and p= 0.0133) and disease-free survival (Median=10.23 months and p= 0.0002) than patients with low Neuropilin-1 expression (Median disease-free survival was 38.7 months). Conclusion: Our findings suggest that Neuropilin-1 is a poor prognosis factor in children with B-lineage ALL and so we recommend the inclusion of Neuropilin-1 as a prognostic marker in children with B-lineage ALL. Its presence at high levels suggests a poor prognosis, and the necessity of intensive therapeutic intervention. |
Introduction
Acute lymphoblastic leukemia (ALL) is the most common childhood
malignancy, representing nearly one-third of all pediatric cancers.[1] With the advent of aggressive multimodality therapy, it has become a curable disease in more than 80% of patients.[2]
More than 75% of patients survive free of leukemia recurrence at least
5 years from diagnosis with current treatments that incorporate
systemic chemotherapy and specific central nervous system preventive
therapy,[3-6] however, the treatment of ALL results in a significant morbidity and mortality.[2] The use of risk-adapted treatment protocols has improved cure rates while limiting the toxicity of therapy.[7]
Angiogenesis
is an important requirement for the development and progression of
hematological malignancies including leukemia and lymphoma.[8]
Vascular endothelial growth factor (VEGF) is an important cytokine that
contributes to disease evolution in various neoplasms. In particular,
VEGF has been described as a mediator of leukemia associated
angiogenesis as well as an autocrine growth regulator in leukemic
cells.[9]
Neuropilin-1 (NRP-1/BDCA4/CD304) is a transmembrane C-type lectin found on plasmacytoid dendritic cells (pDCs).[10] It was initially identified as a receptor for class III semaphorins (SEMA3s) mediating neuronal guidance and axonal growth.[11]
It was subsequently found to bind to VEGF that is a critical
pro-angiogenic factor that induces proliferation and migration of
endothelial cells to tumor vasculature.[12]
Neuropilin-1 expression is reported to be specific for pDCs in humans[13]
and has been found to be highly expressed in diverse solid tumors, as
prostate, breast, pancreatic, lung, ovarian and gastrointestinal
carcinomas.[14,15] Increased expression of Neuropilin-1 has been correlated with tumor growth and invasiveness.[16]
Furthermore,
Neuropilin-1 expression is increased in representative human leukemia
and lymphoma cell lines and in a panel of bone marrow specimens
obtained from patients with acute lymphoblastic leukemia or acute
myeloid leukemia compared with normal bone marrow.[17]
Neuropilin-1 also has been reported to be overexpressed in leukemic
lymphocytes in patients with chronic lymphocytic leukemia (CLL).[18] Therefore, NRP-1 could potentially be used as a target for ligand-directed therapy in leukemia and lymphoma.[17]
Aim of the Work
The objective of this work was to study the prognostic value of Neuropilin-1 expression in Egyptian children with B-lineage ALL.Patients and Methods
The current study was carried out on fifty children after ethical
committee approval and written consent of the parents in the Oncology
Unit, Pediatric Department, Tanta University Hospitals from August 2010
to March 2014. This series included 32 males and 18 females with an age
at diagnosis ranging from 3-17 years and mean value of 9 ± 3.5 years.
This study was conducted on fifty patients with newly diagnosed
B-lineage ALL attendants to. Twenty healthy children, age and sex
matched, serving as a control group, were also included in the study to
estimate the expression of Neuropilin-1 on peripheral blood lymphocyte.
ALL
patients were diagnosed on the basis of the clinical presentation,
morphological and cytochemical evaluation of blood and marrow smears,
together with immunophenotyping. Diagnosis was based on the presence of
20% or more blast cells in bone marrow (BM), according to WHO proposal
and the immunophenotyping results consistent with ALL[19] with exclusion of Philadelphia chromosome-positive ALL cases from this study.
The
laboratory examinations included: complete blood count, serum LDH
levels, bone marrow aspiration, cytochemistry with Sudan black and
Myeloperoxidase, immunophenotyping and estimation of Neuropilin-1
expression on blast cells by flow cytometry. The studied patients were
treated according to standard protocols for B- lineage ALL[20] and were monitored during the period of follow-up that lasted for 42 months.
Flow Cytometry:
Immunophenotyping was performed on gated blast cells from bone marrow
samples by flow cytometry using an extensive panel of Fluorescein
Isothiocyanate [FITC] and Phycoerythrin [PE] conjugated monoclonal
antibodies [MoAbs]. The immunophenotyping of ALL included T-cell
lymphoid markers (CD2, CD3, CD5, CD7, CD4, CD8), B-cell markers (CD10,
CD19, CD22 and cyto-immunoglobulin) and Myeloid cell markers (CD13,
CD33, cyto-MPO).[21] All MoAbs were purchased from
(BD Science, San Jose, CA) while PE-conjugated Neuropilin-1 MoAbs were
supplied by (Ancell Corporation, USA). The results of Neuropilin-1 were
expressed as a percentage of positively stained cells within the gated
blast population. A case was defined as Neuropilin-1 positive if 20% or
more of the gated cells expressed it (Figure 1).[17]
Statistical analysis.
Data were analyzed using SPSS version 20. Quantitative data were
expressed in the form of mean and standard deviation while qualitative
data were described in the form of number and percentage. Differences
between groups were evaluated with student t-test for quantitative data
and Chi-square test and ANOVA for qualitative data. The statistics and
survival analysis were carried out according to Kaplan-Meier product
limit estimates.
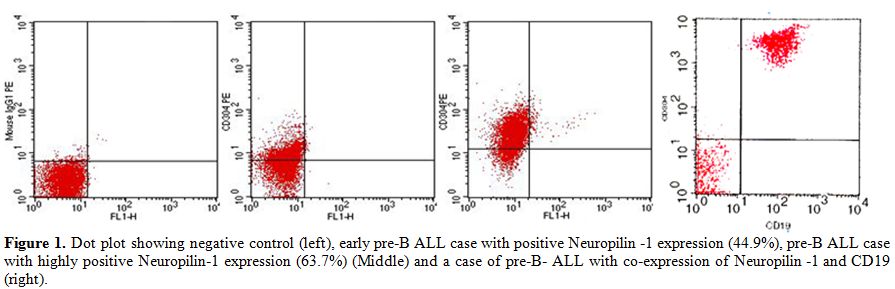 |
Figure 1. Dot plot showing negative control (left), early pre-B ALL case with positive Neuropilin -1 expression (44.9%), pre-B ALL case with highly positive Neuropilin-1 expression (63.7%) (Middle) and a case of pre-B- ALL with co-expression of Neuropilin -1 and CD19 (right). |
Results
There were 31 patients (62% of total) with positive NRP-1 expression
(Neuropilin- present in ≥ 20% of blast population) and 19 patients (38%
of total) with negative Neuropilin-1 expression (< 20% of BM blasts
expressing Neuropilin-1) (Table 1).
There
were no statistically significant differences between Neuropilin-1
positive and Neuropilin-1 negative patients regarding age, sex,
lymphadenopathy, hepatosplenomegaly, CNS involvement, hemoglobin levels
or platelets count, while there were statistically significant
differences between Neuropilin-1 positive and Neuropilin-1 negative
expression regarding leukocytes count, percentage of BM blast cells and
serum LDH levels with higher leucocytes count, percentage of BM blasts
and serum LDH in Neuropilin-1 positive patients (Table 2).
The
studied patients were categorized on the basis of immunophenotyping
into early pre-B ALL (32 cases, 64%) and pre-B ALL (18 cases, 36%).
Neuropilin-1 was significantly higher in pre-B compared with early
pre-B ALL patients (Table 3).
Thirty
patients (60%) achieved and maintained complete remission (CR) till the
end of the study; 12 patients (24%) suffered from relapse and eight
patients died either during induction or maintenance therapy. A greater
number of patients with complete remission were Neuropilin-1 negative
than Neuropilin-1 positive (17/30). Most of ALL patients who relapsed,
were Neuropilin-1 positive (10/12) with a mean expression percentage of
53.8±27.12 and all patients who died were positive for Neuropilin-1 at
diagnosis (8 cases). Neuropilin-1 expression was significantly higher
in relapsed patients and in patients who died during therapy when
compared to patients who achieved complete remission (Table 4).
 |
Table 1. Comparison between Neuropilin-1 positive and negative groups of patients regarding Neuropilin-1 expression. |
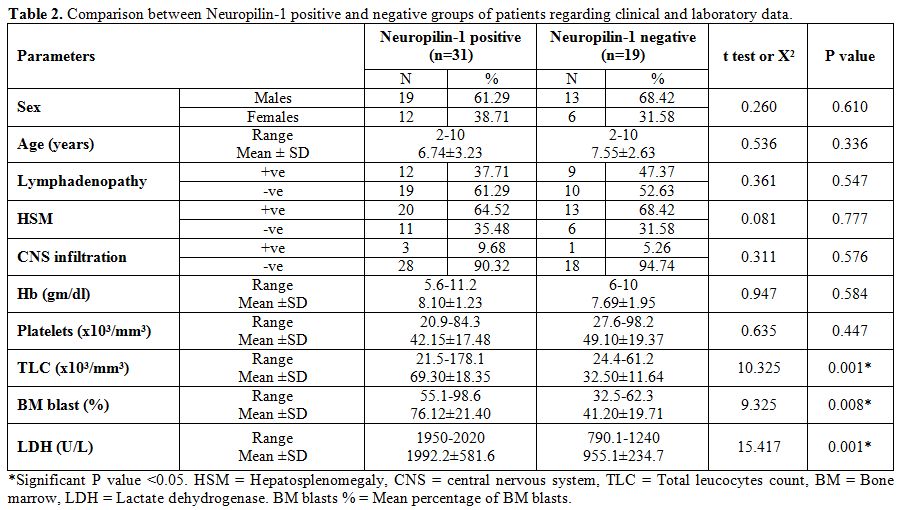 |
Table 2. Comparison between Neuropilin-1 positive and negative groups of patients regarding clinical and laboratory data. |
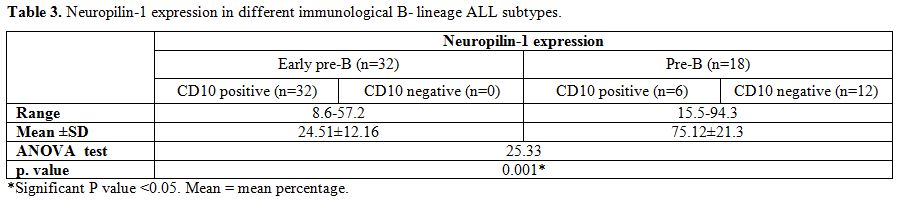 |
Table 3. Neuropilin-1 expression in different immunological B- lineage ALL subtypes. |
 |
Table 4. Neuropilin-1 expression in relation to outcome of ALL. |
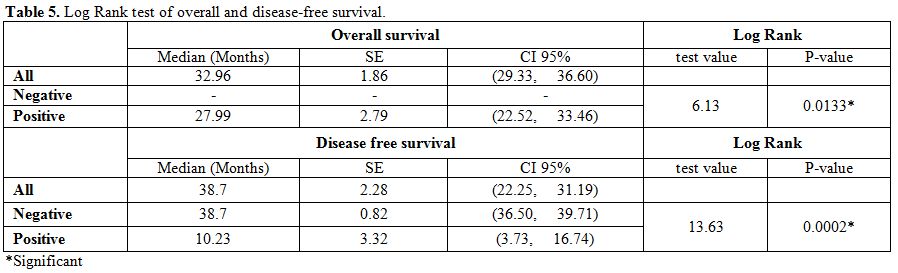 |
Table 5. Log Rank test of overall and disease-free survival. |
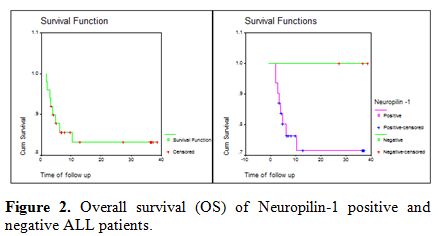 |
Figure 2. Overall survival (OS) of Neuropilin-1 positive and negative ALL patients. |
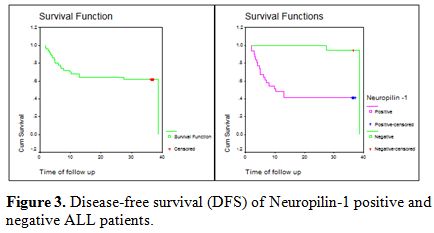 |
Figure 3. Disease-free survival (DFS) of Neuropilin-1 positive and negative ALL patients. |
Discussion
Acute lymphoblastic leukemia (ALL) is the most common childhood
malignancy, representing nearly one-third of all pediatric cancers.[1]
With the advent of aggressive multimodality therapy, it has become a
curable disease in over than 80% of patients, however, the treatment of
ALL results in a significant morbidity and mortality.[2] The use of risk-adapted treatment protocols has improved cure rates while limiting the toxicity of therapy.[7]
The
present study measured Neuropilin-1 surface expression on BM blasts in
50 children with newly diagnosed B-cell ALL compared to normal
peripheral blood lymphocytes from 20 healthy controls by flow
cytometry.
Neuropilin-1 was expressed in all patients with
B-lineage ALL included in this study with variable degrees of
expression ranging from 7.9% to 92.1% of BM blasts. 31 patients
presented high Neuropilin-1 expression ≥ 20% (range: 20.5-92.1)
(Neuropilin-1 positive group) and 19 patients low expression, less than
20% of BM blasts (range: 7.9-14.5) (Neuropilin-1 negative group), while
expression in peripheral blood normal lymphocytes did not exceed 3.4%.
A highly significant statistical difference in levels of Neuropilin-1
expression was found between ALL patients and controls and between
positive and negative Neuropilin-1 expression groups of patients.
This is in agreement with Karjalainen et al 2011[17]
who examined Neuropilin-1 in patients with acute leukemia and
demonstrated its expression, above baseline bone marrow levels, in all
B-cell ALL samples and in two thirds of AML samples with stronger
expression in blast cells of B-cell ALL than AML blast cells.[17] Similarly, Meyerson et al 2012[22]
found that Neuropilin-1 is frequently expressed on B-ALL blasts (71%),
whereas its expression is less frequent on AML blasts (22.9%) and
consistently absent on peripheral blood lymphocytes.[22]
The
present study revealed that the mean percentage of expression of
Neuropilin-1 in bone marrow blasts in B-lineage ALL patients was 36.86%
overall. Neuropilin-1 expression was significantly higher in patients
with pre-B acute lymphoblastic leukemia (74.04%) than patients with
early pre-B ALL (23.55%).
This datum is in agreement with Meyerson et al 2012[22]
who found that Neuropilin-1 is frequently expressed on B-ALL blasts,
and weakly expressed in normal bone marrow B-cell progenitors, while
gradually decreasing during maturation, to be completely lost at later
stages of B-cell. The expression of Neuropilin-1 on B-cell progenitors
may explain its frequent higher expression in precursor B-ALL than
mature ALL.[22]
In our study, Neuropilin-1
expression was significantly associated with higher white blood cells
count; BM blasts percentage and serum LDH levels at diagnosis. There
were significantly higher levels of Neuropilin-1 expression on bone
marrow blasts at diagnosis in patients who subsequently relapsed or
died during the period of follow-up compared to those who achieved and
maintained complete remission. Also, patients with higher Neuropilin-1
expression had significantly shorter overall survival and disease-free
survival than patients with low Neuropilin-1 expression. These results
indicate that higher Neuropilin-1 expression levels correlated with
disease severity and biologic progression in children with B-Lineage
ALL. This datum is in agreement with previous studies establishing the
poor prognostic impact of Neuropilin-1 expression also on AML.[9,23,24,25]
Importance
of Neuropilin-1, as marker of disease in pediatric acute
lymphoblastic leukemia, is further stressed by Beesley et al[26]
who identified Neuropilin-1 as a part of gene expression signature
associated with relapse and adverse clinical outcome, and by Solly et
al.[27] who consider Neuropilin-1 an useful marker of minimal residual disease.
Conclusions
References

[TOP]