Received: March 16, 2014
Accepted: April 6, 2014
Mediterr J Hematol Infect Dis 2015, 7(1): e2015036, DOI 10.4084/MJHID.2015.036
This article is available on PDF format at:

Sanjeev Kumar Sharma, Dharma Choudhary, Anil Handoo, Gaurav Dhamija, Gaurav Kharya, Vipin Khandelwal, Mayank Dhamija and Sweta Kothari
Department of Hemato-Oncology and Bone Marrow Transplantation, BLK Superspeciality Hospital, New Delhi, India.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
Although severe anemia can theoretically result in anemic hypoxia
and can then lead to hypoxic encephalopathy, it is not a primary cause
of encephalopathy. More frequently anemia can contribute with other
multiple causes of encephalopathy such as infection, metabolic
abnormalities, trauma, hepatic dysfunction, hypertension, toxins,
etc. We present here an interesting case of recent onset anemia
that was associated with an encephalopathy of unusual cause.
Case
Clinical history:
A 49-years-old non-hypertensive, non-diabetic male was admitted to the
hospital with the complaints of progressive weakness lasting three
months. For the last two weeks, the patient also had drowsiness. The
patient was hospitalized in the neurology ward for evaluation of
encephalopathy. The patient became increasingly confused during his
hospital stay. There was no history of fever, bleeding from any site,
jaundice, head trauma or drug abuse. He was a non-vegetarian,
non-alcoholic and non-smoker. Patient had a history of deep vein
thrombosis one year back and was treated with warfarin.
Clinical examination:
On examination he had pallor; there was no icterus, cyanosis, pedal
edema and lymphadenopathy. On per abdominal examination, there was no
abdominal distension and no dilated veins over the abdomen. He did not
have hepatosplenomegaly or ascites, and bowel sounds were normal.
Central nervous system evaluation revealed him in altered sensorium
with irritability and
restlessness. There was no neck rigidity,
and bilateral planters were flexor. Bilateral pupils were normal in
size and well reacting to light. Examination of his respiratory and
cardiovascular systems did not reveal any abnormality.
Initial laboratory investigations: His hemogram showed pancytopenia with hemoglobin 7.6 g/dl, total leukocyte count 3.1x109/l and platelet count 108x109/l
with normal differential count on peripheral smear. Mean corpuscular
volume was 85 fl. His liver and kidney function tests were normal
except for total serum protein 5.79 g/dl and albumin of 2.6 g/dl with
reversal of albumin globulin ratio. His serum electrolytes including
calcium and magnesium were in normal range. The workup for altered
sensorium including cerebrospinal fluid examination and magnetic
resonance imaging (MRI) of the brain was inconclusive. The screening
for viral infections including HIV/Hepatitis-B virus/Hepatitis-C virus
was negative. Blood culture was sterile. Peripheral smear did not show
malarial parasites or schistocytes. His antinuclear antibody (ANA) and
serum vitamin B12 and folate levels were also within the standard
range. The thyroid stimulating hormone (TSH) was within normal range.
Differential diagnosis:
1.
Infective causes of altered consciousness were evaluated and ruled out.
Moreover, the patient did not have a fever and cerebrospinal fluid, and
MRI findings were inconclusive. Also, the screening for infection
including bacterial, malarial and viral pathogens was negative.
2. There was no vitamin deficiency/drug abuse/toxin or heavy metal exposure/head trauma.
3. Since the patient had a history of deep vein thrombosis, he was evaluated for paroxysmal nocturnal hemoglobinuria.
4. Bone marrow examination was planned considering myelodysplastic syndrome as a possibility.
Further workup:
Study for paroxysmal nocturnal hemoglobinuria (PNH) did not reveal any
PNH clone. His bone marrow done for evaluation of cytopenias revealed
sheets and clusters of plasma cells suggestive of multiple myeloma (Figure 1).
Serum protein electrophoresis showed M band of 0.4 g/dl. Serum
immunofixation electrophoresis showed kappa light chain only. Serum
free light assay showed kappa-lambda ratio of 165. CT pulmonary
angiography, performed for breathlessness and history of deep vein
thrombosis, showed no evidence of pulmonary embolism, but the ribs
showed multiple lytic lesions. A diagnosis of multiple myeloma was
made. Liver-function tests and abdominal CT showed no evidence of
hepatic dysfunction. Because of increasing altered sensorium and
restlessness the patient required sedation and prophylactic intubation.
Electrolytes, blood urea nitrogen, creatinine and calcium levels were
unremarkable. Though the patient had multiple myeloma, the cause of
altered sensorium could not be found, as all the usual causes of
encephalopathy had been ruled out.
Further evaluation of encephalopathy showed that serum ammonia levels were high, 170 µg/dl (normal range 25-95 µg/dl).
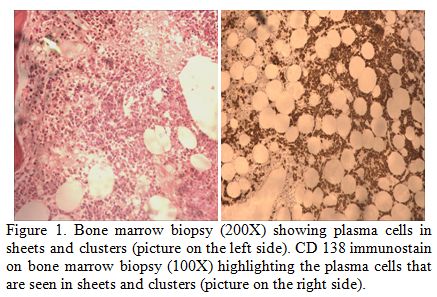 |
Figure 1. Bone marrow biopsy (200X) showing plasma cells in sheets and clusters (picture on the left side). CD 138 immunostain on bone marrow biopsy (100X) highlighting the plasma cells that are seen in sheets and clusters (picture on the right side). |
Treatment: He was started on anti-myeloma therapy with cyclophosphamide, bortezomib, and dexamethasone. Bortezomib was given 1.3 mg/m2 on day 1, 4, 8 and 11, dexamethasone 40 mg/m2
on day 1-4 and cyclophosphamide 500 mg once weekly. On fourth day
patient’s sensorium improved, and he was extubated. His repeat ammonia
levels done on day 4 of chemotherapy were 84 µg/dl and decreased to
50.6 µg/dl after three weeks of therapy. His karyotype showed
tetraploidy. With continued treatment, the patient showed complete
improvement in his sensorium and was discharged on day 22. His
hemoglobin was 11.4 g/dl, total leucocyte count 4.7x109/l and platelets 224x109/l
at the time of discharge. On day 60 of anti-myeloma therapy patient had
no M-band in serum protein electrophoresis and kappa-lambda ratio was
2.14.
Discussion
Central nervous system can be involved in various ways in multiple myeloma.[1,2]
Encephalopathy occurring in multiple myeloma is frequently due to
metabolic disturbances related to the underlying plasma cell disorder,
such as hypercalcemia and uremia.[1] In addition, a direct invasion of CNS and leptomenings by the myeloma cells has also been reported.[2]
In our case hypercalcemia, and renal insufficiency were excluded
by biochemical tests and MRI/CSF examination excluded CNS involvement
by myeloma. Therefore, we considered hyperammoniemia a possible cause
of encephalopathy. Hyperammonemia is involved mostly in the
pathogenesis of hepatic encephalopathy that may present with an
identical clinical syndrome, characterized by altered sensorium and
impaired counsciousness.[3] However, there were
hepatic causes of hyperammonemia in our patient. Although it is not
always possible to establish a right correlation between ammonemia
level and neurologic symptoms, severe acute hyperammonemia causes a
rapidly progressive, often fatal, encephalopathy with brain edema.
Chronic milder hyperammonemia causes a neuropsychiatric illness.[3] Therefore, prompt recognition can be lifesaving.[3]
Among the possible extra-hepatic causes of hyperammonemia, the
literature also reports adult-onset inborn error of metabolism (a urea
cycle disorder), carbamazepine or valproate use, and urinary tract
infection with a urea-hydrolysing organism. Though rare, the
underlying cause may be reversible, and potentially curable with the
appropriate therapy of underlying disease.[3,4]
Encephalopathy associated with hyperammonemia is a rare event in myeloma.[5-11] However, it is a life threatening condition with an overall mortality of 40-48%.[5,10,11]
The diagnosis needs a high level of suspicion, and treatment should
start as soon as possible. The cause of hyperammonemia in myeloma is
not known though excess of ammonia production has been found in human
myeloma cell lines,[12] but also concomitant features
could be significant. Chemotherapy directed against multiple myeloma is
the most efficient treatment to achieve an improvement of neurological
conditions in these patients. Thus, hyperammonemia should be considered
in any patient with multiple myeloma and a low level of consciousness.
Our patient presented with anemia and disturbance of consciousness. He
was diagnosed to have multiple myeloma with hyperammonemia, and there
was a dramatic and fast improvement in sensorium on treating him with
chemotherapy. The improvement was clearly associated with the rapid
decline in serum ammonia levels and progressive increase in hemoglobin
level (Figure 2). The reduction
in M band and free light chain ratio as well the rise of
hemoglobin were late and then could not have any correlation with
neurological improvement.
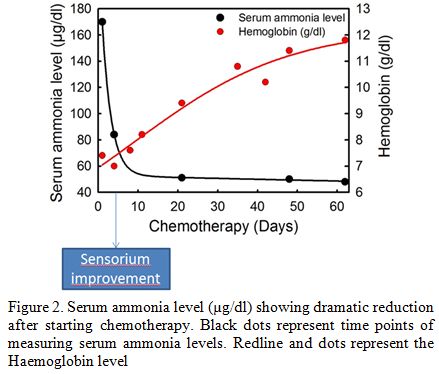 |
Figure 2. Serum ammonia level (µg/dl) showing dramatic reduction after starting chemotherapy. Black dots represent time points of measuring serum ammonia levels. Redline and dots represent the Haemoglobin level |
Conclusion
The more frequent causes of altered sensorium in multiple myeloma include infections, hypercalcemia, uremia or dyselectrolemia, but when none of those could be found then hyperammonemia should be suspected, and treatment for myeloma should be started immediately. Therefore ammonemia should be tested in any patient with myeloma having an altered sensorium. The presentation of this case was unusual and misleading because the patient had pancytopenia and altered sensorium, without any routine biochemical data and radiological imaging suggesting any causes of encephalopathy. Only the bone marrow infiltration of plasma cells and the presence of osteolysis, while making evident the diagnosis of myeloma, suggested checking ammonemia. Anti-myeloma therapy was able to retrieve cytopenias and, by reducing ammonemia, also the altered sensorium.
Acknowledgement
We are thankful to Ms. Bharti, Ms. Sujata, Ms. Ankita and Dr. Sandeep Kumar Sharma for formatting the manuscript.References
 . . . . . . . . . . . .
. . . . . . . . . . . . [TOP]