Bacterial Infections in Hematopoietic Stem Cell Transplant Recipients
Elisa Balletto and Małgorzata Mikulska
Division of Infectious Diseases, IRCCS San
Martino University Hospital – IST, Genoa, Italy. Department of
Health Sciences, University of Genoa, Genoa, Italy
Corresponding author: Małgorzata Mikulska, M.D., PhD. Division of
Infectious Diseases, IRCCS San Martino University Hospital – IST. L.go
R. Benzi, 10 – 16132 Genoa, Italy. Tel: +39 010 5554654; Fax: +39 010
3537680. E-mail:
m.mikulska@unige.it
Published: July 1, 2015
Received: April 7, 2015
Accepted: June 30, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015045, DOI
10.4084/MJHID.2015.045
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Bacterial infections are major
complications after Hematopoietic Stem Cell Transplant (HSCT). They
consist mainly of bloodstream infections (BSI), followed by pneumonia
and gastrointestinal infections, including typhlitis and Clostridium
difficile infection. Microbiological data come mostly from BSI.
Coagulase negative staphylococci and Enterobacteriaceae are the most
frequent pathogens causing approximately 25% of BSI each, followed by
enterococci, P. aeruginosa and viridans streptococci. Bacterial
pneumonia is frequent after HSCT, and Gram-negatives are predominant.
Clostridium difficile infection affects approximately 15% of HSCT
recipients, being more frequent in case of allogeneic than autologous
HSCT.
The epidemiology and the prevalence of resistant strains
vary significantly between transplant centres. In some regions,
multi-drug resistant (MDR) Gram-negative rods are increasingly
frequent. In others, vancomycin-resistant enterococci are predominant.
In the era of increasing resistance to antibiotics, the efficacy of
fluoroquinolone prophylaxis and standard treatment of febrile
neutropenia have been questioned. Therefore, a thorough evaluation of
local epidemiology is mandatory to decide the need for prophylaxis and
the choice of the best regimen for empirical treatment of febrile
neutropenia. For the latter, individualised approach has been proposed,
consisting of either escalation or de-escalation strategy.
De-escalation strategy is recommended since resistant bacteria should
be covered upfront, mainly in patients with severe clinical
presentation and previous infection or colonisation with a resistant
pathogen.
Non-pharmacological interventions, such as screening
for resistant bacteria, applying isolation and contact precautions
should be put in place to limit the spread of MDR bacteria.
Antimicrobial stewardship program should be implemented in transplant
centres.
|
Introduction
Bacterial
infections are among the major complications of hematopoietic stem cell
transplant (HSCT). The most frequent clinical entities are bloodstream
infections (BSI), pneumonia and gastrointestinal infections, which
include typhlitis and infections due to Clostridium difficile.
Infections due to Gram-negative rods used to be the main cause of
infection-related mortality during neutropenia. Fortunately, over the
decades numerous successful strategies have been developed to limit the
negative impact of these infections. In fact, with the universal use of
prompt empirical antibiotic therapy in case of fever during neutropenia
and, in some settings, antibiotic prophylaxis, the fatality rate
dropped significantly.[1]However,
the recent emergence and spread of multidrug-resistant (MDR) bacteria,
particularly Gram-negatives, threaten to nullify all the progress made
in the field of preventing and treating bacterial infections, since the
pathogens that are resistant to all antimicrobials commonly used as
empirical treatment are becoming more and more frequent in HSCT
recipients worldwide.[2,3]This
review will focus on recent changes in the epidemiology of bacterial
infections, mostly BSI, after HSCT, highlighting the epidemiology of
MDR pathogens such as methicillin-resistant staphylococci, vancomycin
resistant enterococci (VRE), Enterobacteriaceae producing
extended-spectrum beta-lactamases (ESBLs), MDR Enterobacteriaceae,
mostly carbapenemase-producing K. pneumoniae (KPC - K. pneumoniae) and MDR P. aeruginosa. The epidemiology of C. difficile
infections will be briefly reviewed. Additionally, advances in the
management of the MDR infections, such as a new approach to empirical
therapy and antimicrobial stewardship will be discussed.
Epidemiology
The most common bacterial infections after HSCT are BSI, pneumonia
and gastrointestinal infections. Urinary tract infections are
infrequent and usually associated with the presence of the urinary
catheter. The reliable data on the aetiology of bacterial infections in
the setting of HSCT come mainly from the results of blood cultures. In
fact BSI is the most frequent microbiologically documented infection,
whereas microbiological documentation is significantly less frequent in
case of pneumonia or typhlitis.
Bloodstream infections
BSI
affects approximately 5-10% of autologous and 20-30% of allogeneic HSCT
recipients, with significant variations between centres and between
patients undergoing different transplantation procedures, e.g. type of
conditioning regimen. The incidence of BSI is the highest during the
pre-engraftment neutropenia and depends mainly on the extent of oral
and enteric mucositis and the presence of a central venous catheter.
During later non-neutropenic phases, BSIs are more frequent in case of
Graft-versus-Host-Disease (GvHD), the presence of hypoglobulineamia or
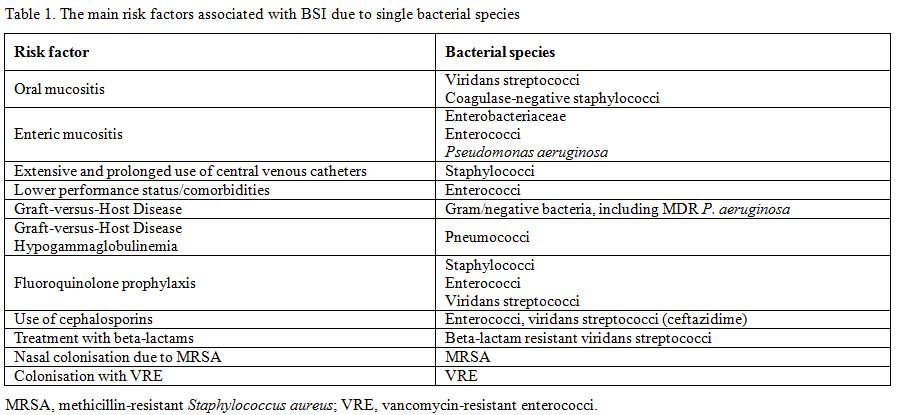
central venous catheter. The main risk factors associated with BSI due
to single bacterial species are reported in Table 1.
|
|
Table 1. The main risk factors associated with BSI due to single bacterial species |
Following a growing body of data on the emergence of resistant Gram-negative rods, 4th
European Conference on the Infections of Leukemia (ECIL-4) in 2011
addressed the issue of bacterial infections in this setting. In order
to understand the extent of the problem, a review of the literature was
performed and a questionnaire was sent to participating centres
focusing of the current epidemiology, resistant patters and recommended
empirical therapy.[4] Additionally, a prospective observational study
on Gram-negative BSI in HSCT recipients is ongoing (registered as
ClinicalTrials.gov Identifier: NCT02257931).The
review of the literature published after 2005 yielded 29 reports from
13 countries concerning autologous (14 reports) and allogeneic (19
reports) HSCT.[4] The median year of observation was 2001, ranging from
1987 to 2009. The Gram-positive to Gram-negative ratio was 60% vs. 40%,
respectively, with some centres reporting the ratio of 85% vs. 15%,
while, others 26% vs. 74%. The ECIL-4 questionnaire included answers
from 33 centres from 18 countries (autologous HSCT in 32 and allogeneic
HSCT in 30 centres), with the median year of observation of 2008
(range, 1998-2010). These more recent data indicated a further decrease
in Gram-positive to Gram-negative ratio (55% vs. 45%), with similar
huge differences between the centres from 85% vs. 15% in some to 30%
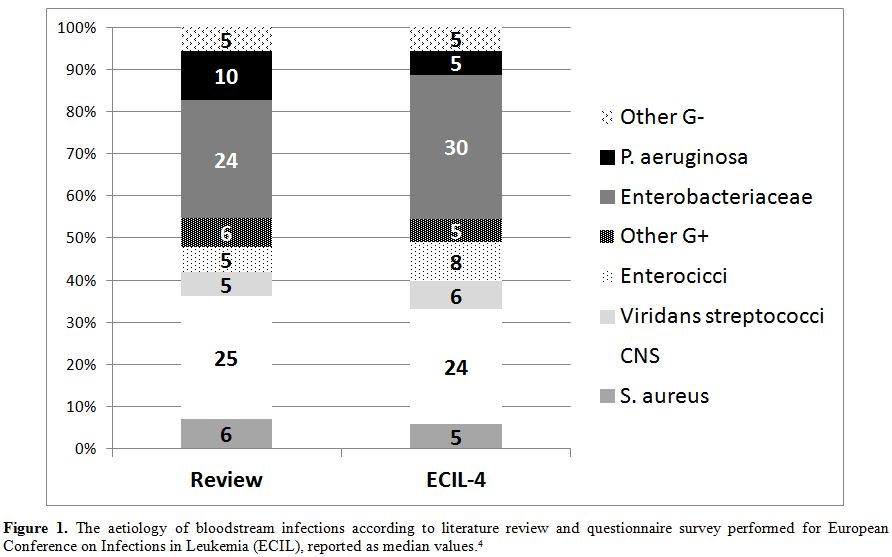
vs. 70% in others.More in detail, Enterobacteriaceae and coagulase-negative staphylococci were the most frequently isolated pathogens (Figure 1). Compared to published data, in the ECIl-4 questionnaire the incidence of P. aeruginosa was lower, but the incidence of enterococci was higher.[4]
|
|
Figure 1. The aetiology of bloodstream infections
according to literature review and questionnaire survey performed for
European Conference on Infections in Leukemia (ECIL), reported as
median values.[4] |
Staphylococci:
Staphylococci are the most frequent pathogens isolated during BSI. They
are mostly coagulase-negative (approx. 25% of all BSI), while S. aureus,
a species significantly more virulent, is associated only with smaller
proportion of infections (approx. 5%).[4] This high rate might be in
part explained by the fact that not all the studies and centres
regarded coagulase-negative staphylococci as a true cause of BSI only
if isolated in two consecutive blood cultures.As
far as resistance pattern is concerned, in ECIL centres more than half
of isolated coagulase-negative staphylococci were resistant to
methicillin while the rate of methicillin-resistance in S. aureus
has been reported lower.[4] In the literature review,
methicillin-resistance was also more frequent among coagulase-negative
staphylococci than S. aureus,
with respective median resistance rates of 80% and 56%.[4] Of note, the
resistance to methicillin has been reported lower in children than in
the adult population. Although the overall incidence of methicillin-resistant S. aureus
(MRSA) BSI is low in HSCT setting, concerns about increased mortality
have been raised. In particular, in two cases of MRSA outbreak, the
attributable mortality was very high. In the UK outbreak, it was
probably over 20% while in an Australian outbreak
in 41 neutropenic patients, the attributable fatality rate was
50%.[5,6] Hopefully, outside an outbreak setting, the outcome of MRSA
infections is more favourable, particularly in centres where
methicillin-resistant staphylococci are regularly seen, and
glycopeptides are frequently used in empirical therapy. Infection
control measures, found effective against MRSA, include alcohol-based
hand hygiene, nasal screening, universal or selective decolonization,
improvement in central line management, and a reduction in the use of
fluoroquinolones, and are all currently recommended by international
guidelines.[7]Good
news concerning MRSA infections is that, for reasons that remain yet to
be fully investigated, since 2004 a worldwide confirmed decline in MRSA
has been noted in the US, and in several European and Far East
countries, despite different infection-control approaches
undertaken.[8,9]Finally,
several new therapeutic options active against MRSA have been
introduced in the last five years, including anti-MRSA cephalosporins
such as ceftaroline or ceftobiprole, lipoglycopeptides such as
telavancin, dalbavancin or oritavancin, or a new oxazolidinone:
tedizolid.[10] Although none of these drugs has been approved for
empirical or targeted treatment of infections in neutropenic patients,
they offer much needed alternatives for better management of
methicillin-resistant infections. Among them, cephalosporins might be
particularly attractive due to their historically known efficacy and
safety while some novel lipoglycopeptides might revolutionise
outpatient treatment allowing for once weekly administration.Enterobacteriaceae: Enterobacteriaceae, and in particular E. coli,
are the second most common pathogen in BSI, being only slightly less
frequent than staphylococci. The mortality associated with infections
due to Enterobacteriaceae is directly associated with the time to the
onset of an effective antibacterial therapy. As demonstrated in the
comparison between ESBL-positive and ESBL-negative BSIs due to E. coli,
the time to the appropriate empirical therapy was longer, and the
outcome was poorer, in case of ESBL-producing strains.[11-13]In most of the European countries, over 10% of all invasive infections caused by E. coli in 2012 were due strains unsusceptible to 3rd
generation cephalosporins and the prevalence of ESBL producing strains
in patients with haematological malignancies varies, being for example
13% in Spain and 48% in Japan.[11,14] The ECIl-4 literature review
reported that in median 34% of Enterobacteriaceae were ESBL-positive,
ranging from 16% to 44% in different centres; whereas according to
ECIL-4 questionnaire over 60% of centres reported that only less than
25% of Enterobacteriaceae were ESBL-producers, including 20% of centres
with the prevalence of ESBL-producers of < 5%.[4] In
another experience from Spain in patients with haematological
malignancies, MDR Gram-negatives (including ESBL-producing strains)
represented 11% of all Gram-negatives, and a significant increase has
been observed compared to the previous observation period (11% vs.
3%).[15,16]Carbapenem-resistant
Enterobacteriaceae are the most recent and rapidly spreading threat,
and in Europe they consist mainly of carbapenem-resistant K. pneumoniae. In fact, in 29 European countries the mean incidence of carbapenem resistance in K. pneumoniae
was 6%, ranging from 0 to 61%,[8] and single-centre outbreaks and
national epidemics have been reported in Greece and Italy, which are
now considered endemic for KPC - K. pneumoniae.[8,17] Until recently, few reports focused exclusively on patients with hematologic malignancy and KPC - K. pneumoniae BSI,
but the reported attributable mortality rates were 38%, 56% and
67%.[17] Therefore, multidisciplinary intensive programs that address
the issue of limiting the spread of these bacteria are warranted.Last
but not least, the issue of resistance of Gram-negatives to
fluoroquinolones is worrisome. Interestingly, in several centres, the
rate of fluoroquinolone resistance in E. coli
increased irrespectively of the use of prophylaxis by the transplant
centre. For example in Sweden, despite the absence of fluoroquinolone
prophylaxis, the resistance in E. coli increased significantly from 2% in years 1995-2001 to 16% in 2002-2008.[18] In Japan, there were no E. coli
resistant to fluoroquinolones during the years 2003-2005 when the
prophylaxis was in place, but in years 2006-2009, when fluoroquinolone
prophylaxis was not prescribed, over 60% of E. coli
tested were resistant.[19] These results might reflect a worldwide
trend in the general increase in fluoroquinolone resistance in
Enterobacteriaceae.[8] Since fluoroquinolone prophylaxis is recommended
and widely used in neutropenic adults receiving allogeneic HSCT, it is
not recommended for empirical treatment of febrile neutropenia.[1,20]
Thus, the rate of fluoroquinolone resistance among Gram-negatives does
not influence significantly therapeutic choices, but it may have severe
implications for the prophylactic strategy in neutropenic HSCT
recipients. In fact, the benefit of fluoroquinolone prophylaxis is
considered uncertain when the prevalence of fluoroquinolone-resistance
in Gram-negative rods exceeds 20%.[21] Therefore, abolishing any
antibiotic prophylaxis might be reasonable in the era of multidrug
resistance, despite the fact that an increase in Gram-negative BSI was
observed in some centres where prophylaxis was
discontinued.[14,15]Enterococci:
Enterococci have emerged as the third most frequent group of bacterial
pathogens in BSI, affecting even 10%-12% of all transplant
patients.[22-26]Compared
to other pathogens, enteroccocal BSI usually occurs later after
transplant, for example, the median day for pre-engraftment BSI was day
+4 for viridans and +11 for enterococci.[27] In many centres, E. faecium almost completely replaced E. faecalis, with important therapeutic consequences since E. faecium is frequently resistant to ampicillin.[24,28,29]In some centres, the shift from E. faecalis to E. faecium has
been also accompanied by an important increase in the rate of
resistance to vancomycin. In a multicentre Australian study VRE
increased from approximately 8% in 2001-2004 period to 64% in years
2007-2010.[24] The problem of vancomycin-resistance is important in
HSCT recipients since few therapeutic options are available, and high
mortality in patients infected with VRE has been reported.[30,31] In
general, there is a low incidence of VRE in European centres with less
than 5% of enterococci, being VRE in 67% haematology centres in the
ECIL-4 questionnaire, in accordance with the general European data
reporting low prevalence of VRE in most countries in Western
Europe.[4,8,22,27-29] On the contrary, in the US up to 80% of E. faecium are
VRE.[25,26,30] In fact, these are mostly the reports from the US
centers that highlight an important mortality in patients with VRE
infection.However,
it remains debatable if the resistance to vancomycin is to blame for
this poor outcome. In fact, enterococci are low virulence pathogens and
numerous concomitant clinical problems are usually present in patients
with enterococcal BSI.[32] Moreover, evaluating the directly
attributable mortality of enteroccocal sepsis in patients with multiple
clinical problems is subjective, and arbitrary even if universally
high; furthermore the 30-day overall mortality might simply indicate
that VRE could be a marker of clinical severity.[25,26,29,30,33]This
view is supported by several clinical experiences. In one study, a
delayed use of adequate antibiotics in case of VRE infection resulted
in no difference in 30-day mortality compared to vancomycin-susceptible
infections in neutropenic patients, and only underlying severity of
medical condition predicted outcome.[34] In another study, Brasilian
authors found that empirical treatment of neutropenic fever with
linezolid had no effect on survival (54% vs. 42%) in 100 haematology
patients who were colonised with VRE, while the mortality was
associated only with the persistence of neutropenia and GvHD.[35]Finally,
in our experience in a cohort of 67 adult allogenic HSCT recipients
with enterococcal BSI, of whom only 13% had VRE infection, 30-day
mortality for vancomycin-susceptible and VRE was respectively, 26% and
11%, whereas 1-year overall survival was 24% for both groups compared
to 65% in patients with no enterococcal BSI.[36] These results were
compared with an experience of a US transplant center, where 66% of
patients with enterococcal BSI had VRE; 30-day mortality was 38% for
both vancomycin-susceptible and resistant enterococci; while 1-year
overall survival was 48% for vancomycin-susceptible enterococci, 23%
for VRE and 63% for patients with no enterococcal BSI.[37]Treatment
of VRE is based on the use of linezolid, for which satisfactory
efficacy data in this setting have been reported. Of note, hematologic
side effects, which are particularly important in HSCT recipients, have
not been reported significant; in particular time to neutrophil and
platelet engraftment has been not found different in 33 cases who
received more than 7 days of linezolid treatment during pre-engraftment
phase, compared to controls.[38] Resistance of enterococci to linezolid
is rare and usually mediated by mutations 23S rRNA target.[39] It has
been associated with previous linezolid therapy, although nosocomial
acquisition of resistant enterococci has been also reported.[39-41]
Resistance mechanisms were first described for E. faecium and S. aureus, and later also for E. faecalis,
but they remain rare, affecting less than 1% of all strains, as
documented in a surveillance study of 7608 clinical isolates of
enterococci from years 2004–2012 collected in the USA.[42]Daptomycin,
for which in vitro activity has been documented but clinical data are
limited in HSCT setting, is another important therapeutic option
against VRE.[43] Several meta-analyses and systematic reviews have
addressed the comparison of outcomes of VRE BSI treated with linezolid
and daptomycin.[44-46] With the evident limit of the low quality of
studies included (mostly retrospective, no randomised trials), the
mortality rates were found slightly higher in case of daptomycin,
compared to linezolid.[44-46] Other options are quinopristin-dalfopristin, which is active only against E. faecium, and not E. faecalis,
and tigecycline, with the well-known limit of low blood
levels.[47] Novel cephalosporins seem inactive against
enterococci while novel glycolipopetides such as telavancin and
dalbavancin seem active only against some (VanB) strains.In conclusion, enterococci are increasingly frequent in HSCT setting, E. faecium
is the predominant species, but resistance to vancomycin varies
significantly between geographical regions. Enterococcal infections,
both due to VRE and vancomycin-susceptible E. faecium, could be
regarded as a marker of poor clinical status and important
comorbidities.[29]Pseudomonas aeruginosa: Pseudomonas aeruginosa
is a Gram-negative pathogen traditionally associated with the highest
mortality rate, both during neutropenia and later after HSCT.
Fortunately, currently its prevalence in infections of European
haematology centres is lower than reported in published reports
(respectively, 5% and 10%), although in some centres it may cause up to
30% of all BSI.[4] Along with high virulence, P. aeruginosa
is characterised by numerous intrinsic or acquired resistance
mechanisms, including adaptive mechanisms, which make numerous
antibiotic options ineffective.[48] In particular, it is characterised
by high intrinsic resistance due to low outer membrane permeability,
which limits antibiotic penetration, beta-lactamase production and
efflux pump overexpression. Additionally, adaptive resistance
mechanisms such as genes expression changes lead to further efflux
increase and enzyme production. Finally, intrinsic mechanisms can be
potentiated by acquired resistance mechanisms which include single or
numerous mutations, or, less frequently, horizontal transfer of
resistance determinants leading to reduced uptake and efflux pump
overexpression.[48] In
fact, the resistance to carbapenems is high, with the mean value in
Europe of 17%, and national estimates between 3% and 51%.[8] In a
multicentre Italian experience from years 2009-2010, 71% of P. aeruginosa strains
causing BSI were MDR, with 60% of them being resistant to
carbapenems.[49] The 30-day mortality was clearly associated with the
resistance: 40% for MDR strains and 9% for susceptible ones.[49]
Similar high resistance rates were reported in India, where 77% of
Pseudomonas strains were MDR.[50] Although most of the cases of MDR P. aeruginosa infections in HSCT recipients stem from in vivo induction of resistance mechanisms, outbreaks of P. aeruginosa
infections have been reported in HSCT units.[51,52] These outbreaks,
similarly to that occurring in other settings, in particular adult or
neonatal intensive care units (ICU), might have environmental source of
infections (e.g. devices, soap or cleaning solutions, etc.), and might
be long lasting, difficult to control and burdened with high morbidity
and mortality.[51-54] Along with outbreaks documenting the clonal
origin of the infective strains, outbreaks not originating from a
common source warrant attention since P. aeruginosa
may be a water-borne pathogen; thus, such outbreaks may be associated
with breaches in proper management of central venous catheters.[55,56]
European guidelines for the management of the infection control
measures to reduce transmission of multidrug-resistant Gram-negative
bacteria in hospitalized patients have been recently published.[57] Colistin remains the cornerstone of the treatment of MDR P. aeruginosa, with the uncertainties concerning the optimal dosing, the need for combination therapy and the rate of toxicity.[58]Acinetobacter baumannii: A. baumannii
is a non-fermentative coccobacillus that is widely distributed in
nature and characterized by frequent MDR due to multiple
mechanisms.[59,60] Recently, BSI due to MDR A. baumannii has
emerged as a major cause of health care-associated infections,
especially in critically ill population, including immunocompromised
patients.[61] It is generally associated with a high crude mortality
rate, ranging between 17% and 52%.[62] Risk factors for infections with
MDR A. baumannii in the
immunocompromised include previous colonization, comorbid conditions,
recent major surgical procedures, prolonged broad-spectrum
antimicrobial therapy, prolonged hospitalization, admission to ICU and
mechanical ventilation.[63]Little
is known regarding the incidence and risk factors for this infection in
HSCT recipients.[60,64] In the aforementioned ECIL-4 literature review
and questionnaire, A. baumannii
was responsible for a median of 2% of all BSIs, being absent in some
centres but rising up to as high as 12% of all BSIs in others.[4] In a
retrospective case-control study Kim et al. found that the total
incidence of MDR A. baumannii BSI was 0.52 cases/10,000 patient-days,
with a mortality rate of 95%. The interval between admission and HSCT
and a history of care in ICU after HSCT were independent risk factors
for the development of A. baumannii
infection.[65] These features suggest that this infection affects
predominantly patients who require intensive and invasive support,
particularly ICU care and mechanical ventilation therapy after HSCT. Of
note, in almost 90% of cases BSI developed after engraftment and lungs
were the origin of infection in all the patients.[65] Antimicrobial agents that are potentially effective against A. baumannii include carbapenems, beta-lactam inhibitors such as sulbactam, piperacillin–tazobactam and 3rd generation cephalosporins. New options for MDR A. baumannii
infections are old polypeptide antibiotics such as colistin or
polymyxin B, minocycline derivatives such as tigecycline, new
carbapenems such as doripenem, and new generation cephalosporins such
as ceftobiprole and ceftaroline.[59,63] In uncomplicated infections,
the use of a single active beta-lactam may be justified, while
definitive treatment of complicated infections in critically ill
individuals may require drug combinations such as colistin and
rifampicin or colistin and carbapenem.[60]In conclusion, MDR A. baumannii
BSI in HSCT recipients is a fatal infectious complication with no
controlled trials to guide the therapeutic choices. As in case of
others MDR pathogens, an approach which stratifies the risk of
developing infection, and a prompt administration of active
antimicrobial therapy, chosen on the basis of local epidemiology and
previous colonization, may hopefully lead to better clinical outcomes.Viridans streptococci: Viridans streptococci have been traditionally associated with oral mucositis in course of chemotherapy (see Table 1).
Although usually susceptible to beta-lactams, the risk of developing
septic shock and acute distress respiratory syndrome (ARDS) has been
reported as high, varying from 7% to 39%.[66] Given high mortality
rates reported in early studies, administration of corticosteroids to
neutropenic patients with viridans streptococci BSI who develop early
signs of respiratory failure have been studied with the aim of
preventing the progression to ARDS and improving the survival.[67-69]Nowadays, viridans streptococci are responsible for approximately 5% of all BSI. Streptococcus mitis
is the most frequently isolated species, and it is also the species
associated more frequently with resistance to penicillin and
fluoroquinolones.[70] The association between high penicillin MIC
values, clinical outcome and the need for vancomycin treatment has been
elegantly discussed in a recent editorial.[66]
Pneumonia
Most of the studies describing infectious complications in HSCT patients show a high frequency of pneumonia,[71-73] with an incidence reported in retrospectives studies ranging between 15% and 25%.[74,75]Numerous
acute pulmonary complications may occur in this population including
both infectious and non-infectious causes, hence it is often difficult
to obtain an aetiological diagnosis. The clinical setting and
microbiological analyses, such as cultures of blood samples, sputum and
bronchoalveolar lavage fluid, can be used to provide clues for
interpreting abnormal CT finding but infections with more than one
pathogens (e.g. bacterial and viral) and coexistence of infectious and
non-infectious processes (e.g. viral and immunological) further hamper
the precise description of epidemiology in this setting.Therefore,
the results of a nationwide prospective study referring to data
collected by the Spanish Research Network of Transplant (RESITRA) are
particularly interesting.[76] From July 2003 to April
2005 427 HSCT recipients were followed with standardized diagnostic
protocol for pneumonia. There were 112 episodes of pneumonia and 72
(64%) of them were microbiologically defined. Bacterial pneumonia
(n=32, 44%) was more frequent than fungal (n=21, 29%) and viral
pneumonia (n=14, 19%). The most frequent pathogens isolated in each
group were: Escherichia coli (n=7, 9%), CMV (n=12, 15%), and Aspergillus spp. (n=12, 15%). Among bacteria, the most common aetiologies were E. coli and P. aeruginosa, as previously reported in other studies,[71,77] whereas S. pneumoniae caused only 5% of pneumonias and this finding was possibly associated with the routine use of immunization and prophylaxis. The
median time of pneumonia diagnosis after transplantation was 66.5 days.
Even if bacterial pneumonia is usually reported during the neutropenic
phase soon after HSCT, in this study the pneumonias caused by
Gram-negative bacilli appeared significantly later than pneumonia
caused by moulds (p=0.02), possibly because P. aeruginosa pneumonia may occur later in the post-transplant period in patients developing GvHD.[77]The
global mortality rate in allogeneic HSCT recipients that had at least
one pneumonia episode was 46% (n=44) compared to 13% (n=43) in those
without any pneumonia episode (p<0.01; RR 3.37; 95%CI: 2.43–4.68).
Clinical factors increasing the mortality rate in HSCT recipients
developing a pulmonary complication were invasive fungal infection,
acute or chronic GvHD, developing pneumonia in the first 100 days after
transplantation, acute respiratory failure and septic shock.The
results of this prospective multicentre study confirm that pneumonia
remains a frequent infectious complication after HSCT, contributing to
significant mortality.
Clostridium difficile infection
In
last decade, there has been a growing interest in Clostridium difficile
infection (CDI) because of the increasing rate of this infection. This
epidemiological change has been ascribed to the emergence of an
epidemic strain of C. difficile known as NAP-1, which has been
associated with an increased frequency and severity of the disease.
Nowadays CDI is the leading cause of infectious diarrhoea in
hospitalized patients, and HSCT recipients appear to be one of the
highest risk populations for this infection. In fact, Chopra et al.
found that among all hospitalized patients in a non-outbreak setting,
CDI rates in HSCT recipients were nine-fold higher than those in
general patients and 1.4-fold higher than those in other patients with
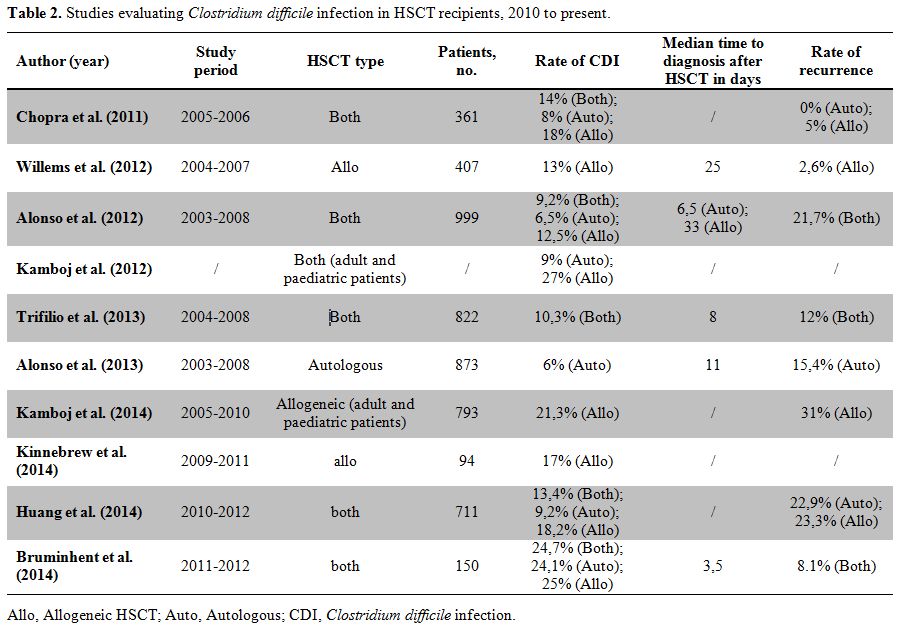
cancer.[78] Therefore, a brief review of the available studies on CDI in HSCT recipients has been performed and is outlined in Table 2.
|
|
Table 2. Studies evaluating Clostridium difficile infection in HSCT recipients, 2010 to present. |
Referring to the reviewed literature, CDI affects between 5.7%[79] and 24.7%[80]
of adult HSCT recipients during the first year after transplant, with
the highest rates reported by the most recent studies. The same
literature review showed that most CDI cases occur in the early
post-transplant period with median time to diagnosis ranging between
3.5 days[80] and 33 days after HSCT (Table 2).[81]
Some authors observed that CDI is more likely to occur in the early
phase of HSCT if recipients are pre-colonized with toxigenic C.
difficile.[80,82] Many studies
reported high rates of infection due to NAP-1 strain, but Alonso et al.
found that overall rates of CDI was not significantly different between
the two centres involved in the study, despite differences in NAP-1
endemicity.[79] Risk factors for CDI in hematopoietic
transplant recipients are poorly understood. The difficulties in
identifying unique risk factors for CDI in HSCT population may arise
from the ubiquity of traditional risk factors for CDI in this
population. In fact, most patients, if not all, receive broad spectrum
antibiotics, have a prolonged hospital stay, have an altered integrity
of the intestinal mucosa, and all are severely ill and
immunocompromised. Furthermore, the use of allogeneic HSCT has expanded
progressively to older patients due to the development of reduced
intensity conditioning regimens. Thus, both older age and the presence
of comorbidities are increasingly frequent in HSCT setting.Many
studies focused on risk factors for CDI in HSCT population, and several
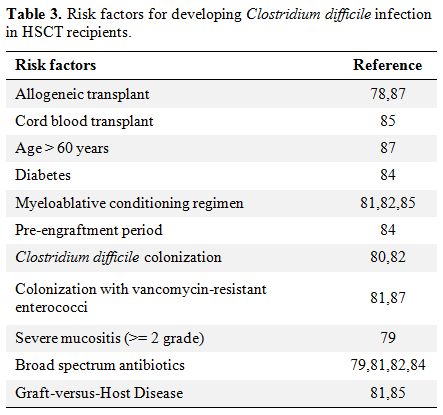
risk factors have been identified. They are reported in Table 3.
Some authors found that CDI occurred significantly more often in
allogeneic recipients (incidence 12.5%-21.3%) than in the autologous
recipients (incidence 5.7%-9.2%).[78,83]
On the contrary, a recent prospective study by Bruminhent et al. showed
no difference in the incidence of CDI in patients receiving autologous
and allogeneic HSCTs (24% versus 25%, respectively).[80] Other possible risk factors for developing CDI are use of broad-spectrum antimicrobials,[79,81,82,84] and acute GvHD,[81,85] while myeloablative conditioning regimen increased the risk in some,[81,82,85] but not all cohorts.[86] The only variable associated with a reduced risk of CDI was the use of growth factors.[84] Interestingly, Bruminhent et al. analysed the relationship between prior C. difficile
colonization and CDI. In this prospective study at least 10.7% of
patients admitted for HSCT were colonized with a toxigenic strain and
nearly all of them (87.5%) developed CDI, compared to 17.2% of patients
with negative colonization status at hospital admission (p < 0.01).[80]
|
|
Table 3. Risk factors for developing Clostridium difficile infection in HSCT recipients. |
The
most controversial issue is a potentially important interplay between
CDI and gastrointestinal GvHD. Whereas some studies showed a strong
relationship between early CDI and subsequent development of
gastrointestinal GvHD in the first year following allogeneic HSCT,[81,84,87] this association has not been confirmed by other studies.[80,82,85,86]As
far as clinical course of CDI is concerned, the disease in most studies
was uniformly mild, irrespective of the rate of infections due to NAP-1
strain,[86] and no differences in the mortality rates were observed in patients with or without CDI.[78,79,81,82,85]
The low percentage of complications in this patients population may be
due to a decreased inflammation from immunosuppression related to
transplantation.[79] In fact, only one study found
that HSCT recipients with CDI were more likely to develop GvHD, BSIs
and had lower survival rate when compared to controls.[84]
In contrast to other studies reporting little impact of CDI on
mortality in HSCT recipients, a recent Brazilian experience of 64
patients with CDI, including 31 cases after allogeneic and 14 after
autologous HSCT, demonstrated a significant impact of CDI on survival.
In particular, a severe form of CDI developed in 23% of allogeneic HSCT
recipients, and all of them died.[88] Of note, 89% of
patients in this cohort received initial treatment with metronidazole
that might have influenced the clinical course of CDI.One
of the main problems of CDI in the immunocompromised is a high rate or
recurrent infections. In fact, in HSCT recipients recurrence rates
ranged between 2.6%[85] and 31%,[86]
and they were more frequent in those patients who received
metronidazole monotherapy compared to those who received
vancomycin-containing regimens.[81] Other risk factors for recurrent disease were neutropenia at the onset of CDI8 and infection due to NAP-1 strain.[86]
The frequent use of proton pump inhibits might also contribute to
recurrences, as recently demonstrated in a general patient population.[89]The
management of CDI is based on prompt diagnosis, effective treatment and
strict application of contact precautions which do not differ between
HSCT recipients and other vulnerable.[90]In
conclusion, CDI is one of the most frequent causes of infectious
diarrhoea in HSCT recipients, and it occurs early in the
post-transplant period. Updated diagnostic and treatment algorithms for
CDI should be put in place. Since many of the risk factors for CDI are
not easily modifiable in this population, the predisposing role of
pre-transplant colonization with C. difficile warrants further studies.
Although CDI represent an important cause of morbidity for this
population, non-severe forms of CDI are predominant, and associated
mortality seems low.
Recent advances in the management of bacterial infections
Since
any delay in starting an effective antibiotic therapy for the treatment
of bacterial infections (particularly due to Gram-negatives) has been
associated with an increased mortality, empirical therapy directed
against Enterobacteriaceae and P. aeruginosa has been a cornerstone of managing bacterial infections during neutropenia for decades.[1] Ceftazidime, cefepime, piperacillin/tazobactam or carbapenems are listed as suitable options.[1]The
only recent trial on empirical therapy reported on the use of oral
moxifloxacin in low risk patients with febrile neutropenia, and found
it non inferior to the standard oral option of amoxicillin/clavulanate
and ciprofloxacin.[91] However, this novel regimen is
unsuitable for HSCT recipients since they are usually high risk
patients and frequently receive fluoroquinolone prophylaxis during
neutropenia. In
the times when resistant pathogens are seen on a daily basis in many
centres, the main advance in the management of bacterial infections in
HSCT is a novel individualised approach to the empirical antibiotic
therapy.[92] In fact, ECIL-4 recommendations on the
empirical therapy of febrile neutropenia propose two different
approaches based on clinical presentation and the risk for infection
due to a resistant strain.[92] The classical escalation strategy is defined as starting an antibiotic which covers susceptible Enterobacteriaceae and P. aeruginosa, but not ESBL-producers, carbapenem-resistant K. pneumoniae
or other MDR strains. Then, if patient’s clinical conditions
deteriorate, or if a resistant pathogen is isolated, therapy is
escalated to cover suspected or isolated resistant bacteria. Its
advantages include: 1) limiting early use of a combination therapy or a
broadest spectrum antibacterial, such as carbapenem, 2) low toxicity,
3) usually lower costs, and 4) hopefully, less selection of resistant
strains. Anti-pseudomonal cephalosporins, such as cefepime or
ceftazidime, or piperacillin/tazobactam are the most frequently used
treatment options. The novelty in approaching empirical antibiotic
therapy in neutropenia consists of introducing a strategy that has been
used widely so far in the intensive care unit setting. De-escalation
approach means starting upfront a regimen covering the most
dangerous resistant pathogens, i.e. ESBL-producers, MDR P. aeruginosa
etc.[92] The main point of using a de-escalation
strategy is to start active treatment of a suspected resistant
Gram-negative, hopefully resulting in reduced mortality. Its main limit
is a frequently unnecessary routine use of broad spectrum molecules or
a combination therapy with nephrotoxic agents such as aminoglycosides
or colistin. The
most difficult clinical decision is establishing which patients might
benefit from a de-escalation approach and which may still be
confidently treated with a classical escalation approach. From the
review of the literature and personal experience, the most frequent
risk factors for infection with resistant bacteria are: prior infection
or colonisation with a non-susceptible strain and being admitted to or
coming from a centre where resistant bacteria are frequent.[92]
De-escalation treatment is usually administered to subjects with one of
the aforementioned risk factors who develop sepsis or septic shock
during neutropenia. The management of infections caused by antibiotic
resistant Gram-negative bacteria in HSCT recipients has been recently
reviewed.[93]
Infection control measures
Non-pharmacological
management of bacterial infections is of outmost importance in the era
of increasing bacterial resistance. It includes screening for resistant
bacterial and applying infection control measures in case of
transmissible pathogens. Of note, these include not only MDR
Gram-negatives or VRE, but also C. difficile.
Hand hygiene and contact precautions (gloves and gown) are the most
effective infection control strategies that apply to the prevention of
the spread of any pathogens.Surveillance
cultures for MDR bacteria identify patients colonised with resistant
strains. This knowledge, not only allows to avoid actively transmission
to other HSCT recipients by applying contact precautions, but may also
suggest which antibiotics might be appropriate for empirical treatment.
Another theoretical possibility is to pursuit decontamination of the
colonised patients, although the data on decolonisation in HSCT setting
are almost inexistent, and the results are far from promising.
Additionally, the risk of inducing resistance to the last available
treatment option in case of MDR Gram-negative rods should be
counterbalance with an evident long-term benefit of decontamination.[93]
Antimicrobial stewardship
Last
but not least, the management of bacterial infections in HSCT should
include a formal program on antimicrobial stewardship.[94]
Its main objectives are to improve the outcome of infections and to
reduce inappropriate use of antimicrobials (e.g. discontinue if not
necessary, promote the use of correct dosage). Additional aims include
reducing side effects of antibiotic therapies, i.e. direct toxicity or
influence on local epidemiology, and hopefully, but not automatically,
reducing costs of antibiotic treatments (by withholding antibiotic
treatment if not necessary, de-escalation to narrow spectrum agents if
possible, etc.). Running
a successful antimicrobial stewardship program is based on a
multidisciplinary approach, with a dedicated team that includes, among
others, infectious diseases specialist, microbiologist, clinical
pharmacologist and infection control specialist, and on approval and
endorsement of hospital authorities, which enable to allocate necessary
resources.One
of important points of reviewing antibiotic prescriptions are clinical
audits to identify the critical areas for antibiotic use in HSCT unit
(e.g. inappropriate indications, incorrect dosage, routine
prescriptions off-label, too long therapies, no intravenous to oral
switch, etc.) and a thorough knowledge of local epidemiology of the
most frequent pathogens, the rate of resistance to various
antimicrobials, and clinical outcome of these infections. Conclusions
Bacterial infections continue to be one of the most frequent
complications after HSCT. The incidence of Gram-negative bacteria and
the rate of resistance to antibiotics have been steadily increasing in
many centres. However, important differences in the epidemiology of
bacterial infections exist among transplant centres worldwide.
Therefore, the knowledge of local epidemiology is crucial and should
guide the approach to antibiotic prophylaxis, empirical therapy and
management of infections. Numerous interesting issues such as the role
of surveillance cultures for guiding empirical therapy, the benefits of
protocols for screening for resistant bacteria, decolonisation and the
current role of antibiotic prophylaxis in HSCT setting await to be
addressed in future clinical studies.
References
- Freifeld AG, Bow EJ, Sepkowitz KA, Boeckh MJ,
Ito JI, Mullen CA, Raad, II, Rolston KV, Young JA, Wingard JR,
Infectious Diseases Society of A. Clinical practice guideline for the
use of antimicrobial agents in neutropenic patients with cancer: 2010
update by the infectious diseases society of america. Clin Infect Dis.
2011 52: 4:427-431. http://dx.doi.org/10.1093/cid/ciq147 PMid:21205990

- Boucher
HW, Talbot GH, Bradley JS, Edwards JE, Gilbert D, Rice LB, Scheld M,
Spellberg B, Bartlett J. Bad bugs, no drugs: No eskape! An update from
the infectious diseases society of america. Clin Infect Dis. 2009 48:
1:1-12. http://dx.doi.org/10.1086/595011 PMid:19035777
- Bow
EJ. There should be no eskape for febrile neutropenic cancer patients:
The dearth of effective antibacterial drugs threatens anticancer
efficacy. J Antimicrob Chemother. 2013 68: 3:492-495. http://dx.doi.org/10.1093/jac/dks512 PMid:23299574
- Mikulska
M, Viscoli C, Orasch C, Livermore DM, Averbuch D, Cordonnier C, Akova
M, Fourth European Conference on Infections in Leukemia Group
ajvoEEIELN, Esgich/Escmid. Aetiology and resistance in bacteraemias
among adult and paediatric haematology and cancer patients. J Infect.
2014 68: 4:321-331. http://dx.doi.org/10.1016/j.jinf.2013.12.006 PMid:24370562
- Shaw
BE, Boswell T, Byrne JL, Yates C, Russell NH. Clinical impact of mrsa
in a stem cell transplant unit: Analysis before, during and after an
mrsa outbreak. Bone Marrow Transplant. 2007 39: 10:623-629. http://dx.doi.org/10.1038/sj.bmt.1705654 PMid:17384657
- Quilty
S, Kwok G, Hajkowicz K, Currie B. High incidence of
methicillin-resistant staphylococcus aureus sepsis and death in
patients with febrile neutropenia at royal darwin hospital. Intern Med
J. 2009 39: 8:557-559. http://dx.doi.org/10.1111/j.1445-5994.2009.02003.x PMid:19732205
- Liu
C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL,
Karchmer AW, Levine DP, Murray BE, M JR, Talan DA, Chambers HF,
Infectious Diseases Society of A. Clinical practice guidelines by the
infectious diseases society of america for the treatment of
methicillin-resistant staphylococcus aureus infections in adults and
children. Clin Infect Dis. 2011 52: 3:e18-55.
- ECDC.
European centre for disease prevention and control. Antimicrobial
resistance surveillance in europe 2012. Annual report of the european
antimicrobial resistance surveillance network (ears-net). Stockholm:
Ecdc; available at: Http://ecdc.Europa.Eu/en/publications/publications/antimicrobial-resistance-surveillance-europe-2012.Pdf. 2013
- Livermore DM. Fourteen years in resistance. Int J Antimicrob Agents. 2012 39: 4:283-294. http://dx.doi.org/10.1016/j.ijantimicag.2011.12.012 PMid:22386741
- Rodvold
KA, McConeghy KW. Methicillin-resistant staphylococcus aureus therapy:
Past, present, and future. Clin Infect Dis. 2014 58 Suppl 1: S20-27. http://dx.doi.org/10.1093/cid/cit614 PMid:24343828
- Gudiol
C, Calatayud L, Garcia-Vidal C, Lora-Tamayo J, Cisnal M, Duarte R,
Arnan M, Marin M, Carratala J, Gudiol F. Bacteraemia due to
extended-spectrum beta-lactamase-producing escherichia coli (esbl-ec)
in cancer patients: Clinical features, risk factors, molecular
epidemiology and outcome. J Antimicrob Chemother. 2010 65: 2:333-341. http://dx.doi.org/10.1093/jac/dkp411 PMid:19959544
- Trecarichi
EM, Tumbarello M, Spanu T, Caira M, Fianchi L, Chiusolo P, Fadda G,
Leone G, Cauda R, Pagano L. Incidence and clinical impact of
extended-spectrum-beta-lactamase (esbl) production and fluoroquinolone
resistance in bloodstream infections caused by escherichia coli in
patients with hematological malignancies. J Infect. 2009 58: 4:299-307.
http://dx.doi.org/10.1016/j.jinf.2009.02.002 PMid:19272650
- Kang
CI, Chung DR, Ko KS, Peck KR, Song JH, Korean Network for Study of
Infectious D. Risk factors for infection and treatment outcome of
extended-spectrum beta-lactamase-producing escherichia coli and
klebsiella pneumoniae bacteremia in patients with hematologic
malignancy. Ann Hematol. 2012 91: 1:115-121. http://dx.doi.org/10.1007/s00277-011-1247-7 PMid:21556875
- Chong
Y, Yakushiji H, Ito Y, Kamimura T. Clinical impact of fluoroquinolone
prophylaxis in neutropenic patients with hematological malignancies.
Int J Infect Dis. 2011 15: 4:e277-281. http://dx.doi.org/10.1016/j.ijid.2010.12.010 PMid:21324723
- Gudiol
C, Bodro M, Simonetti A, Tubau F, Gonzalez-Barca E, Cisnal M,
Domingo-Domenech E, Jimenez L, Carratala J. Changing aetiology,
clinical features, antimicrobial resistance, and outcomes of
bloodstream infection in neutropenic cancer patients. Clin Microbiol
Infect. 2013 19: 5:474-479. http://dx.doi.org/10.1111/j.1469-0691.2012.03879.x PMid:22524597
- Gudiol
C, Tubau F, Calatayud L, Garcia-Vidal C, Cisnal M, Sanchez-Ortega I,
Duarte R, Calvo M, Carratala J. Bacteraemia due to multidrug-resistant
gram-negative bacilli in cancer patients: Risk factors, antibiotic
therapy and outcomes. J Antimicrob Chemother. 2011 66: 3:657-663. http://dx.doi.org/10.1093/jac/dkq494 PMid:21193475
- Satlin
MJ, Jenkins SG, Walsh TJ. The global challenge of carbapenem-resistant
enterobacteriaceae in transplant recipients and patients with
hematologic malignancies. Clin Infect Dis. 2014 58: 9:1274-1283. http://dx.doi.org/10.1093/cid/ciu052 PMid:24463280 PMCid:PMC4038783
- Kjellander
C, Bjorkholm M, Cherif H, Kalin M, Giske CG. Hematological: Low
all-cause mortality and low occurrence of antimicrobial resistance in
hematological patients with bacteremia receiving no antibacterial
prophylaxis: A single-center study. Eur J Haematol. 2012 88: 5:422-430.
http://dx.doi.org/10.1111/j.1600-0609.2012.01768.x PMid:22335785
- Chong
Y, Yakushiji H, Ito Y, Kamimura T. Clinical impact of fluoroquinolone
prophylaxis in neutropenic patients with hematological malignancies.
Int J Infect Dis. 2009 15: 4:e277-281. http://dx.doi.org/10.1016/j.ijid.2010.12.010 PMid:21324723
- Tomblyn
M, Chiller T, Einsele H, Gress R, Sepkowitz K, Storek J, Wingard JR,
Young JA, Boeckh MJ, Center for International B, Marrow R, National
Marrow Donor p, European B, MarrowTransplant G, American Society of B,
Marrow T, Canadian B, Marrow Transplant G, Infectious Diseases Society
of A, Society for Healthcare Epidemiology of A, Association of Medical
M, Infectious Disease C, Centers for Disease C, Prevention. Guidelines
for preventing infectious complications among hematopoietic cell
transplantation recipients: A global perspective. Biol Blood Marrow
Transplant. 2009 15: 10:1143-1238. http://dx.doi.org/10.1016/j.bbmt.2009.06.019 PMid:19747629 PMCid:PMC3103296
- Bow EJ. Fluoroquinolones, antimicrobial resistance and neutropenic cancer patients. Curr Opin Infect Dis. 2011 24: 6:545-553. http://dx.doi.org/10.1097/QCO.0b013e32834cf054 PMid:22001945
- Cappellano
P, Viscoli C, Bruzzi P, Van Lint MT, Pereira CA, Bacigalupo A.
Epidemiology and risk factors for bloodstream infections after
allogeneic hematopoietic stem cell transplantion. New Microbiol. 2007
30: 2:89-99. PMid:17619251
- Mikulska
M, Del Bono V, Prinapori R, Boni L, Raiola AM, Gualandi F, Van Lint MT,
Dominietto A, Lamparelli T, Cappellano P, Bacigalupo A, Viscoli C. Risk
factors for enterococcal bacteremia in allogeneic hematopoietic stem
cell transplant recipients. Transpl Infect Dis. 2010 12: 6:505-512. http://dx.doi.org/10.1111/j.1399-3062.2010.00544.x PMid:20636482
- Macesic
N, Morrissey CO, Cheng AC, Spencer A, Peleg AY. Changing microbial
epidemiology in hematopoietic stem cell transplant recipients:
Increasing resistance over a 9-year period. Transpl Infect Dis. 2014
16: 6:887-896. http://dx.doi.org/10.1111/tid.12298 PMid:25298044
- Kamboj
M, Chung D, Seo SK, Pamer EG, Sepkowitz KA, Jakubowski AA, Papanicolaou
G. The changing epidemiology of vancomycin-resistant enterococcus (vre)
bacteremia in allogeneic hematopoietic stem cell transplant (hsct)
recipients. Biol Blood Marrow Transplant. 2010 16: 11:1576-1581. http://dx.doi.org/10.1016/j.bbmt.2010.05.008 PMid:20685257 PMCid:PMC3670412
- Tavadze
M, Rybicki L, Mossad S, Avery R, Yurch M, Pohlman B, Duong H, Dean R,
Hill B, Andresen S, Hanna R, Majhail N, Copelan E, Bolwell B, Kalaycio
M, Sobecks R. Risk factors for vancomycin-resistant enterococcus
bacteremia and its influence on survival after allogeneic hematopoietic
cell transplantation. Bone Marrow Transplant. 2014 49: 10:1310-1316. http://dx.doi.org/10.1038/bmt.2014.150 PMid:25111516
- Blennow
O, Ljungman P, Sparrelid E, Mattsson J, Remberger M. Incidence, risk
factors, and outcome of bloodstream infections during the
pre-engraftment phase in 521 allogeneic hematopoietic stem cell
transplantations. Transpl Infect Dis. 2014 16: 1:106-114. http://dx.doi.org/10.1111/tid.12175 PMid:24372809
- Mikulska
M, Del Bono V, Raiola AM, Bruno B, Gualandi F, Occhini D, di Grazia C,
Frassoni F, Bacigalupo A, Viscoli C. Blood stream infections in
allogeneic hematopoietic stem cell transplant recipients: Reemergence
of gram-negative rods and increasing antibiotic resistance. Biol Blood
Marrow Transplant. 2009 15: 1:47-53. http://dx.doi.org/10.1016/j.bbmt.2008.10.024 PMid:19135942
- Gudiol
C, Ayats J, Camoez M, Dominguez MA, Garcia-Vidal C, Bodro M, Ardanuy C,
Obed M, Arnan M, Antonio M, Carratala J. Increase in bloodstream
infection due to vancomycin-susceptible enterococcus faecium in cancer
patients: Risk factors, molecular epidemiology and outcomes. PLoS One.
2013 8: 9:e74734.
- Avery
R, Kalaycio M, Pohlman B, Sobecks R, Kuczkowski E, Andresen S, Mossad
S, Shamp J, Curtis J, Kosar J, Sands K, Serafin M, Bolwell B. Early
vancomycin-resistant enterococcus (vre) bacteremia after allogeneic
bone marrow transplantation is associated with a rapidly deteriorating
clinical course. Bone Marrow Transplant. 2005 35: 5:497-499. http://dx.doi.org/10.1038/sj.bmt.1704821 PMid:15640812
- DiazGranados
CA, Jernigan JA. Impact of vancomycin resistance on mortality among
patients with neutropenia and enterococcal bloodstream infection. J
Infect Dis. 2005 191: 4:588-595. http://dx.doi.org/10.1086/427512 PMid:15655783
- Caballero-Granado
FJ, Becerril B, Cuberos L, Bernabeu M, Cisneros JM, Pachon J.
Attributable mortality rate and duration of hospital stay associated
with enterococcal bacteremia. Clin Infect Dis. 2001 32: 4:587-594. http://dx.doi.org/10.1086/318717 PMid:11181122
- Dubberke
ER, Hollands JM, Georgantopoulos P, Augustin K, DiPersio JF, Mundy LM,
Khoury HJ. Vancomycin-resistant enterococcal bloodstream infections on
a hematopoietic stem cell transplant unit: Are the sick getting sicker?
Bone Marrow Transplant. 2006 38: 12:813-819. http://dx.doi.org/10.1038/sj.bmt.1705530 PMid:17057724
- Cho
SY, Lee DG, Choi SM, Kwon JC, Kim SH, Choi JK, Park SH, Park YJ, Choi
JH, Yoo JH. Impact of vancomycin resistance on mortality in neutropenic
patients with enterococcal bloodstream infection: A retrospective
study. BMC Infect Dis. 2013 13: 504. http://dx.doi.org/10.1186/1471-2334-13-504 PMid:24164924 PMCid:PMC3870976
- Lisboa
LF, Miranda BG, Vieira MB, Dulley FL, Fonseca GG, Guimaraes T, Levin
AS, Shikanai-Yasuda MA, Costa SF. Empiric use of linezolid in febrile
hematology and hematopoietic stem cell transplantation patients
colonized with vancomycin-resistant enterococcus spp. Int J Infect Dis.
2015 33: 171-176. http://dx.doi.org/10.1016/j.ijid.2015.02.001 PMid:25660090
- Mikulska
M, Del Bono V, Raiola AM, Signori A, Prinapori R, Ghiso A, Bacigalupo
A, Viscoli C. Enterococcal bloodstream infection after hematopoietic
stem cell transplant: Experience of a center with a low prevalence of
vancomycin-resistant enterococci. Clin Infect Dis. 2012 55: 12:1744.
- Vydra
J, Shanley RM, George I, Ustun C, Smith AR, Weisdorf DJ, Young JA.
Enterococcal bacteremia is associated with increased risk of mortality
in recipients of allogeneic hematopoietic stem cell transplantation.
Clin Infect Dis. 2012 http://dx.doi.org/10.1093/cid/cis550 PMid:22693346 PMCid:PMC3657510
- Cohen
N, Mihu CN, Seo SK, Chung D, Chou J, Heller G, Papanicolaou GA.
Hematologic safety profile of linezolid in the early periengraftment
period after allogeneic stem cell transplantation. Biol Blood Marrow
Transplant. 2009 15: 10:1337-1341. http://dx.doi.org/10.1016/j.bbmt.2009.05.021 PMid:19747643
- Ager
S, Gould K. Clinical update on linezolid in the treatment of
gram-positive bacterial infections. Infection and drug resistance. 2012
5: 87-102. PMid:22787406 PMCid:PMC3392139
- Pogue
JM, Paterson DL, Pasculle AW, Potoski BA. Determination of risk factors
associated with isolation of linezolid-resistant strains of
vancomycin-resistant enterococcus. Infect Control Hosp Epidemiol. 2007
28: 12:1382-1388. http://dx.doi.org/10.1086/523276 PMid:17994519
- Dobbs
TE, Patel M, Waites KB, Moser SA, Stamm AM, Hoesley CJ. Nosocomial
spread of enterococcus faecium resistant to vancomycin and linezolid in
a tertiary care medical center. Journal of clinical microbiology. 2006
44: 9:3368-3370. http://dx.doi.org/10.1128/JCM.00850-06 PMid:16954275 PMCid:PMC1594671
- Mendes
RE, Deshpande LM, Jones RN. Linezolid update: Stable in vitro activity
following more than a decade of clinical use and summary of associated
resistance mechanisms. Drug resistance updates: reviews and
commentaries in antimicrobial and anticancer chemotherapy. 2014 17:
1-2:1-12.
- Barber
KE, King ST, Stover KR, Pogue JM. Therapeutic options for
vancomycin-resistant enterococcal bacteremia. Expert Rev Anti Infect
Ther. 2015 13: 3:363-377. http://dx.doi.org/10.1586/14787210.2015.1001839 PMid:25661903
- Balli
EP, Venetis CA, Miyakis S. Systematic review and meta-analysis of
linezolid versus daptomycin for treatment of vancomycin-resistant
enterococcal bacteremia. Antimicrob Agents Chemother. 2014 58:
2:734-739. http://dx.doi.org/10.1128/AAC.01289-13 PMid:24247127 PMCid:PMC3910884
- Chuang
YC, Wang JT, Lin HY, Chang SC. Daptomycin versus linezolid for
treatment of vancomycin-resistant enterococcal bacteremia: Systematic
review and meta-analysis. BMC Infect Dis. 2014 14: 687. http://dx.doi.org/10.1186/s12879-014-0687-9 PMid:25495779 PMCid:PMC4269951
- Whang
DW, Miller LG, Partain NM, McKinnell JA. Systematic review and
meta-analysis of linezolid and daptomycin for treatment of
vancomycin-resistant enterococcal bloodstream infections. Antimicrob
Agents Chemother. 2013 57: 10:5013-5018. http://dx.doi.org/10.1128/AAC.00714-13 PMid:23896468 PMCid:PMC3811395
- Bradley JS. Which antibiotic for resistant gram-positives, and why? J Infect. 2014 68 Suppl 1: S63-75. http://dx.doi.org/10.1016/j.jinf.2013.09.016 PMid:24188585
- Breidenstein
EB, de la Fuente-Nunez C, Hancock RE. Pseudomonas aeruginosa: All roads
lead to resistance. Trends in microbiology. 2011 19: 8:419-426. http://dx.doi.org/10.1016/j.tim.2011.04.005 PMid:21664819
- Trecarichi
EM, Tumbarello M, Caira M, Candoni A, Cattaneo C, Pastore D, Fanci R,
Nosari AM, Vianelli N, Busca A, Spadea A, Pagano L. Multidrug resistant
pseudomonas aeruginosa bloodstream infection in adult patietns with
hematological malignancies. Haematologica. 2011 96: 1:e1-3. http://dx.doi.org/10.3324/haematol.2010.036640 PMid:21193424 PMCid:PMC3012771
- Sood
P, Seth T, Kapil A, Sharma V, Dayama A, Sharma S, Kumar S, Singh AK,
Mishra P, Mahapatra M. Emergence of multidrug resistant acinetobacter
blood stream infections in febrile neutropenia patients with
haematological cancers and bone marrow failure syndromes. Journal of
the Indian Medical Association. 2012 110: 7:439-444. PMid:23520666
- Fanci
R, Bartolozzi B, Sergi S, Casalone E, Pecile P, Cecconi D, Mannino R,
Donnarumma F, Leon AG, Guidi S, Nicoletti P, Mastromei G, Bosi A.
Molecular epidemiological investigation of an outbreak of pseudomonas
aeruginosa infection in an sct unit. Bone Marrow Transplant. 2009 43:
4:335-338. http://dx.doi.org/10.1038/bmt.2008.319 PMid:18850015
- Mudau
M, Jacobson R, Minenza N, Kuonza L, Morris V, Engelbrecht H, Nicol MP,
Bamford C. Outbreak of multi-drug resistant pseudomonas aeruginosa
bloodstream infection in the haematology unit of a south african
academic hospital. PLoS One. 2013 8: 3:e55985.
- Nagao
M, Iinuma Y, Igawa J, Saito T, Yamashita K, Kondo T, Matsushima A,
Takakura S, Takaori-Kondo A, Ichiyama S. Control of an outbreak of
carbapenem-resistant pseudomonas aeruginosa in a haemato-oncology unit.
J Hosp Infect. 2011 79: 1:49-53. http://dx.doi.org/10.1016/j.jhin.2011.04.018 PMid:21722990
- Knoester
M, de Boer MG, Maarleveld JJ, Claas EC, Bernards AT, de Jonge E, van
Dissel JT, Veldkamp KE. An integrated approach to control a prolonged
outbreak of multidrug-resistant pseudomonas aeruginosa in an intensive
care unit. Clin Microbiol Infect. 2014 20: 4:O207-215. http://dx.doi.org/10.1111/1469-0691.12372 PMid:24707852
- Rasmussen
BS, Christensen N, Sorensen J, Rosenvinge FS, Kolmos HJ, Skov MN.
Outbreak of pseudomonas aeruginosa bacteraemia in a haematology
department. Danish Medical Journal. 2015 62: 4:A5040.
- Dobbs
TE, Guh AY, Oakes P, Vince MJ, Forbi JC, Jensen B, Moulton-Meissner H,
Byers P. Outbreak of pseudomonas aeruginosa and klebsiella pneumoniae
bloodstream infections at an outpatient chemotherapy center. American
journal of infection control. 2014 42: 7:731-734. http://dx.doi.org/10.1016/j.ajic.2014.03.007 PMid:24969124
- Tacconelli
E, Cataldo MA, Dancer SJ, De Angelis G, Falcone M, Frank U, Kahlmeter
G, Pan A, Petrosillo N, Rodriguez-Bano J, Singh N, Venditti M, Yokoe
DS, Cookson B. Escmid guidelines for the management of the infection
control measures to reduce transmission of multidrug-resistant
gram-negative bacteria in hospitalized patients. Clin Microbiol Infect.
2014 20 Suppl 1: 1-55. http://dx.doi.org/10.1111/1469-0691.12427 PMid:24329732
- Martis
N, Leroy S, Blanc V. Colistin in multi-drug resistant pseudomonas
aeruginosa blood-stream infections: A narrative review for the
clinician. J Infect. 2014 69: 1:1-12. http://dx.doi.org/10.1016/j.jinf.2014.03.001 PMid:24631777
- Karageorgopoulos
DE, Kelesidis T, Kelesidis I, Falagas ME. Tigecycline for the treatment
of multidrug-resistant (including carbapenem-resistant) acinetobacter
infections: A review of the scientific evidence. J Antimicrob
Chemother. 2008 62: 1:45-55. http://dx.doi.org/10.1093/jac/dkn165 PMid:18436554
- Al-Anazi
KA, Al-Jasser AM. Infections caused by acinetobacter baumannii in
recipients of hematopoietic stem cell transplantation. Frontiers in
oncology. 2014 4: 186. http://dx.doi.org/10.3389/fonc.2014.00186
- Fournier
PE, Richet H. The epidemiology and control of acinetobacter baumannii
in health care facilities. Clin Infect Dis. 2006 42: 5:692-699. http://dx.doi.org/10.1086/500202 PMid:16447117
- Cisneros
JM, Rodriguez-Bano J. Nosocomial bacteremia due to acinetobacter
baumannii: Epidemiology, clinical features and treatment. Clin
Microbiol Infect. 2002 8: 11:687-693. http://dx.doi.org/10.1046/j.1469-0691.2002.00487.x PMid:12445005
- Maragakis
LL, Perl TM. Acinetobacter baumannii: Epidemiology, antimicrobial
resistance, and treatment options. Clin Infect Dis. 2008 46:
8:1254-1263. http://dx.doi.org/10.1086/529198 PMid:18444865
- Al-Anazi
KA, Abdalhamid B, Alshibani Z, Awad K, Alzayed A, Hassan H, Alsayiegh
M. Acinetobacter baumannii septicemia in a recipient of an allogeneic
hematopoietic stem cell transplantation. Case reports in
transplantation. 2012 2012: 646195.
- Kim
SB, Min YH, Cheong JW, Kim JS, Kim SJ, Ku NS, Jeong SJ, Han SH, Choi
JY, Song YG, Kim JM. Incidence and risk factors for carbapenem- and
multidrug-resistant acinetobacter baumannii bacteremia in hematopoietic
stem cell transplantation recipients. Scandinavian journal of
infectious diseases. 2014 46: 2:81-88. http://dx.doi.org/10.3109/00365548.2013.857042 PMid:24325335
- Freifeld
AG, Razonable RR. Viridans group streptococci in febrile neutropenic
cancer patients: What should we fear? Clin Infect Dis. 2014 59:
2:231-233. http://dx.doi.org/10.1093/cid/ciu264 PMid:24755859
- Shenep JL. Viridans-group streptococcal infections in immunocompromised hosts. Int J Antimicrob Agents. 2000 14: 2:129-135. http://dx.doi.org/10.1016/S0924-8579(99)00172-7
- Yacoub
AT, Mojica L, Jones L, Knab A, Alrabaa S, Greene J. The role of
corticosteroids in adult respiratory distress syndrome caused by
viridans group streptococci bacteremia in neutropenic patients.
Mediterranean Iournal of Hematology and Infectious Diseases. 2014 6:
1:e2014055.
- Dompeling
EC, Donnelly JP, Raemaekers JM, De Pauw BE. Pre-emptive administration
of corticosteroids prevents the development of ards associated with
streptococcus mitis bacteremia following chemotherapy with high-dose
cytarabine. Ann Hematol. 1994 69: 2:69-71. http://dx.doi.org/10.1007/BF01698484 PMid:8080881
- Han
XY, Kamana M, Rolston KV. Viridans streptococci isolated by culture
from blood of cancer patients: Clinical and microbiologic analysis of
50 cases. Journal of clinical microbiology. 2006 44: 1:160-165. http://dx.doi.org/10.1128/JCM.44.1.160-165.2006 PMid:16390964 PMCid:PMC1351950
- Yoo
JH, Lee DG, Choi SM, Choi JH, Park YH, Kim YJ, Kim HJ, Lee S, Kim DW,
Lee JW, Min WS, Shin WS, Kim CC. Infectious complications and outcomes
after allogeneic hematopoietic stem cell transplantation in korea. Bone
Marrow Transplant. 2004 34: 6:497-504. http://dx.doi.org/10.1038/sj.bmt.1704636 PMid:15286689
- Dettenkofer
M, Wenzler-Rottele S, Babikir R, Bertz H, Ebner W, Meyer E, Ruden H,
Gastmeier P, Daschner FD. Surveillance of nosocomial sepsis and
pneumonia in patients with a bone marrow or peripheral blood stem cell
transplant: A multicenter project. Clin Infect Dis. 2005 40: 7:926-931.
http://dx.doi.org/10.1086/428046 PMid:15824981
- Yamasaki
S, Heike Y, Mori S, Fukuda T, Maruyama D, Kato R, Usui E, Koido K, Kim
S, Tanosaki R, Tobinai K, Teshima T, Takaue Y. Infectious complications
in chronic graft-versus-host disease: A retrospective study of 145
recipients of allogeneic hematopoietic stem cell transplantation with
reduced- and conventional-intensity conditioning regimens. Transpl
Infect Dis. 2008 10: 4:252-259. http://dx.doi.org/10.1111/j.1399-3062.2007.00291.x PMid:18194371
- Forslow
U, Mattsson J, Ringden O, Klominek J, Remberger M. Decreasing mortality
rate in early pneumonia following hematopoietic stem cell
transplantation. Scandinavian journal of infectious diseases. 2006 38:
11-12:970-976.
- Gentile
G, Micozzi A, Girmenia C, Iori AP, Donati PP, Capria S, Martino P.
Pneumonia in allogenic and autologous bone marrow recipients. A
retrospective study. Chest. 1993 104: 2:371-375. http://dx.doi.org/10.1378/chest.104.2.371 PMid:8339620
- Aguilar-Guisado
M, Jimenez-Jambrina M, Espigado I, Rovira M, Martino R, Oriol A,
Borrell N, Ruiz I, Martin-Davila P, de la Camara R, Salavert M, de la
Torre J, Cisneros JM, Spanish Network for Research in Infectious D.
Pneumonia in allogeneic stem cell transplantation recipients: A
multicenter prospective study. Clinical transplantation. 2011 25:
6:E629-638. http://dx.doi.org/10.1111/j.1399-0012.2011.01495.x PMid:22150886
- Alangaden
GJ, Wahiduzzaman M, Chandrasekar PH, Bone Marrow Transplant G.
Aspergillosis: The most common community-acquired pneumonia with
gram-negative bacilli as copathogens in stem cell transplant recipients
with graft-versus-host disease. Clin Infect Dis. 2002 35: 6:659-664. http://dx.doi.org/10.1086/342061 PMid:12203161
- Chopra
T, Alangaden GJ, Chandrasekar P. Clostridium difficile infection in
cancer patients and hematopoietic stem cell transplant recipients.
Expert Rev Anti Infect Ther. 2010 8: 10:1113-1119. http://dx.doi.org/10.1586/eri.10.95 PMid:20954878
- Alonso
CD, Dufresne SF, Hanna DB, Labbe AC, Treadway SB, Neofytos D, Belanger
S, Huff CA, Laverdiere M, Marr KA. Clostridium difficile infection
after adult autologous stem cell transplantation: A multicenter study
of epidemiology and risk factors. Biol Blood Marrow Transplant. 2013
19: 10:1502-1508. http://dx.doi.org/10.1016/j.bbmt.2013.07.022 PMid:23916741 PMCid:PMC3806308
- Bruminhent
J, Wang ZX, Hu C, Wagner J, Sunday R, Bobik B, Hegarty S, Keith S,
Alpdogan S, Carabasi M, Filicko-O'Hara J, Flomenberg N, Kasner M,
Outschoorn UM, Weiss M, Flomenberg P. Clostridium difficile
colonization and disease in patients undergoing hematopoietic stem cell
transplantation. Biol Blood Marrow Transplant. 2014 20: 9:1329-1334. http://dx.doi.org/10.1016/j.bbmt.2014.04.026 PMid:24792871
- Alonso
CD, Treadway SB, Hanna DB, Huff CA, Neofytos D, Carroll KC, Marr KA.
Epidemiology and outcomes of clostridium difficile infections in
hematopoietic stem cell transplant recipients. Clin Infect Dis. 2012
54: 8:1053-1063. http://dx.doi.org/10.1093/cid/cir1035 PMid:22412059 PMCid:PMC3309884
- Kinnebrew
MA, Lee YJ, Jenq RR, Lipuma L, Littmann ER, Gobourne A, No D, van den
Brink M, Pamer EG, Taur Y. Early clostridium difficile infection during
allogeneic hematopoietic stem cell transplantation. PLoS One. 2014 9:
3:e90158.
- Huang
AM, Marini BL, Frame D, Aronoff DM, Nagel JL. Risk factors for
recurrent clostridium difficile infection in hematopoietic stem cell
transplant recipients. Transpl Infect Dis. 2014 16: 5:744-750. http://dx.doi.org/10.1111/tid.12267 PMid:25040545
- Dubberke
ER, Reske KA, Srivastava A, Sadhu J, Gatti R, Young RM, Rakes LC,
Dieckgraefe B, DiPersio J, Fraser VJ. Clostridium difficile-associated
disease in allogeneic hematopoietic stem-cell transplant recipients:
Risk associations, protective associations, and outcomes. Clinical
transplantation. 2010 24: 2:192-198. http://dx.doi.org/10.1111/j.1399-0012.2009.01035.x PMid:19624693 PMCid:PMC3390201
- Willems
L, Porcher R, Lafaurie M, Casin I, Robin M, Xhaard A, Andreoli AL,
Rodriguez-Otero P, Dhedin N, Socie G, Ribaud P, Peffault de Latour R.
Clostridium difficile infection after allogeneic hematopoietic stem
cell transplantation: Incidence, risk factors, and outcome. Biol Blood
Marrow Transplant. 2012 18: 8:1295-1301. http://dx.doi.org/10.1016/j.bbmt.2012.02.010 PMid:22387347
- Kamboj
M, Xiao K, Kaltsas A, Huang YT, Sun J, Chung D, Wu S, Sheahan A,
Sepkowitz K, Jakubowski AA, Papanicolaou G. Clostridium difficile
infection after allogeneic hematopoietic stem cell transplant: Strain
diversity and outcomes associated with nap1/027. Biol Blood Marrow
Transplant. 2014 20: 10:1626-1633. http://dx.doi.org/10.1016/j.bbmt.2014.06.025 PMid:24973628
- Trifilio
SM, Pi J, Mehta J. Changing epidemiology of clostridium
difficile-associated disease during stem cell transplantation. Biol
Blood Marrow Transplant. 2013 19: 3:405-409. http://dx.doi.org/10.1016/j.bbmt.2012.10.030 PMid:23219779
- Spadao
F, Gerhardt J, Guimaraes T, Dulley F, Almeida Junior JN, Batista MV,
Shikanai-Yasuda MA, Levin AS, Costa SF. Incidence of diarrhea by
clostridium difficile in hematologic patients and hematopoietic stem
cell transplantation patients: Risk factors for severe forms and death.
Revista do Instituto de Medicina Tropical de Sao Paulo. 2014 56:
4:325-331.
http://dx.doi.org/10.1590/S0036-46652014000400010 PMid:25076434 PMCid:PMC4131819 - McDonald
EG, Milligan J, Frenette C, Lee TC. Continuous proton pump inhibitor
therapy and the associated risk of recurrent clostridium difficile
infection. JAMA internal medicine. 2015 175: 5:784-791. http://dx.doi.org/10.1001/jamainternmed.2015.42 PMid:25730198
- Surawicz
CM, Brandt LJ, Binion DG, Ananthakrishnan AN, Curry SR, Gilligan PH,
McFarland LV, Mellow M, Zuckerbraun BS. Guidelines for diagnosis,
treatment, and prevention of clostridium difficile infections. The
American journal of gastroenterology. 2013 108: 4:478-498; quiz 499. http://dx.doi.org/10.1038/ajg.2013.4 PMid:23439232
- Kern
WV, Marchetti O, Drgona L, Akan H, Aoun M, Akova M, de Bock R, Paesmans
M, Viscoli C, Calandra T. Oral antibiotics for fever in low-risk
neutropenic patients with cancer: A double-blind, randomized,
multicenter trial comparing single daily moxifloxacin with twice daily
ciprofloxacin plus amoxicillin/clavulanic acid combination
therapy--eortc infectious diseases group trial xv. J Clin Oncol. 2013
31: 9:1149-1156. http://dx.doi.org/10.1200/JCO.2012.45.8109 PMid:23358983
- Averbuch
D, Orasch C, Cordonnier C, Livermore DM, Mikulska M, Viscoli C, Gyssens
IC, Kern WV, Klyasova G, Marchetti O, Engelhard D, Akova M, Ecil
ajvoEEIEE, Eln. European guidelines for empirical antibacterial therapy
for febrile neutropenic patients in the era of growing resistance:
Summary of the 2011 4th european conference on infections in leukemia.
Haematologica. 2013 98: 12:1826-1835. http://dx.doi.org/10.3324/haematol.2013.091025 PMid:24323983 PMCid:PMC3856957
- Mikulska
M. How to manage infections caused by antibiotic resistant
gram-negative bacteria - ebmt educational meeting from the severe
aplastic anaemia and infectious diseases working parties, Naples,
Italy, 2014. Current drug targets. 2015 http://dx.doi.org/10.2174/1389450116666150223162138 PMid:25706258
- Gyssens
IC, Kern WV, Livermore DM, Ecil ajvoEEI, ESCMID Eo. The role of
antibiotic stewardship in limiting antibacterial resistance among
hematology patients. Haematologica. 2013 98: 12:1821-1825. http://dx.doi.org/10.3324/haematol.2013.091769 PMid:24323982 PMCid:PMC3856956
[TOP]