Received: August 4, 2015
Accepted: August 24, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015052, DOI 10.4084/MJHID.2015.052
This article is available on PDF format at:

Agustin Avilés
Oncology Research Unit. Oncology Hospital National Medical Center, IMSS, México DF, Mexico.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Nasal natural killer/T-cell lymphoma
(nasal NKTCL), is a rare presentation of extranodal lymphoma in
North-America and Europe, but in some countries, as China and Korea,
nasal NKTCL occurred in 20 to 46 % of T-cell
lymphomas. Some studies, analyzing the incidence in Latin-America,
observed some differences between the various populations. However,
this comparison included Argentina and Chile, Peru, and other
Latin-America but not the Mexico. Thus, we performed a retrospective
analysis of the patients diagnosed and treated as nasal, NKTCL, in our
institution that is an academic tertiary national reference hospital of
Mexico. From 1988 to 2014, we diagnosed and treated 14,816 cases of non-Hodgkin’s lymphoma, 10,957 (73%) were of B-cell histology and 3822 (26%) were of T-cell histology. Nasal, NKTCL, was the most frequent of the T-cell histology: 40%. We compared our results with those of other countries and observed that nasal, NKTCL have a small number of cases in North-America, and in some countries of Latin-America, as Argentina, Brazil, and Chile. However, the number of NKTCL cases found in Mexico was similar to that found in Guatemala and Peru, and also in China and Korea. Our study suggests that this neoplasm could have a racial basis, but environmental factors should also be considered. |
Introduction
Nasal NK/T-cell lymphoma (NKTCL), is a rare presentation
of malignant lymphoma with protean clinical features,
characterized by destruction of the upper
respiratory tract, in particular of the nasal cavity,
nasal and paranasal sinuses, and hard palate.[1]
It is more common in Asia, and in some countries of Latin America, as Guatemala and Peru than in Western countries.[1]
Mexico
is a country that geographically and politically is part of
North-America, but with racial differences, that can reflect the
differences in some neoplasm, specifically NK/TCL. Although some
environmental factors have to be considered as part of these
differences, until now, the racial differences appear mostly to be the
cause of the high proportion of these special setting of patients in
Mexico.
Thus, we performed a retrospective analysis of patients
with NK/TCL, which were diagnosed and treated at our Hospital. The
Oncology Hospital at National Medical, is a tertiary national reference
center for patients with cancer, in the Mexican Institute of Social
Security. Although our institution has a national coverage with
53,000,000 of people; we cannot considered these study as a national
study. Subsequently, we searched for reports of NKTCL, in other
countries. Some of these patients have been previously reported.[2-7]
Patients and Methods
We, while searching clinical records of the patients from 1988 to
2014 with a diagnosis of Non-Hodgkin lymphoma, separated patients with
a confirmed diagnosis, according to the criteria of the
World Health Organization. From 2009 to 2012, our Pathology
Department performed a revision of all T-cell lymphomas, which were
reclassified according to the World Health Organization.
Entry
criteria were as follow: age >18 years without upper limit; no
gender differences; at the immunohistochemical studies, all
lymphomas were CD2+, cytoplasm CD3epsilon+, CD56+, and expressing
perforin enzyme B, TIA. Evidence of Epstein-Barr virus was shown
by in situ hybridization. Prognostic factors were evaluated according
to the International Prognostic Index (IPI) and the Korean
proposal. Staging studies were performed as previously mentioned;[7] positive emission tomography (PET) was added since available in our institution (2008).
Treatment was made as previously reported,[5]
and was based on the administration of combined therapy, chemotherapy
and radiotherapy, most cases as the “sandwich“ technique, that at
present is considered the treatment of choice in our institution.
Results
From 1988 to 2014, we diagnosed 14,816 cases of non-Hodgkin
lymphoma, 10958 (73%) were of B-cell histology; and 3822 (26%) were of
T-cell histology. In 36 cases, the type of cell was not identified,
because the slides were not available for revision, and these cases
were not included in this paper.
Table 1,
shown the histopathology of the T-cell lymphoma, most cases (40%), were
NKTCL, followed by peripheral T-cell non-specified, other T-cell
lymphomas were rare.
Table 2
shows the clinical and laboratory characteristics of the NKTCL
patients. According the stage, the early stages were more frequent.
Also according the clinical risk, the low and intermediate forms
evaluated by IPI, and the groups 0 and 1, by Korean prognostic model
for nasal NK/T-cell lymphoma were more frequently found.
As
expected, patients with advanced stages: III and IV, had poorer
prognosis factors, a clinical high risk in both systems and a poor
performance status. Curiously, of the advanced stages, only 21 patients
(2.7%) were at stage III.
Table 3
shows that, in early stages, radiotherapy attained a complete response
(RT) of 73%, of patients, but the relapse, especially outside the
radiation site, was frequent. Salvage chemotherapy rescued more
patients, but the overall survival (OS) was low when compared to
combined therapy. We did not treat advanced stages with radiotherapy
alone. The best results were achieved with the use of combined therapy;
“sandwich technique” is considered the best combination. Taking into
consideration the poor results with chemotherapy alone in early and
advanced stages, we did not recommend chemotherapy alone in this type
of lymphoma.
Table 4 shows a comparative analysis of patients from different countries.[8-18]
NKTCL, nasal type, is a rare disease in Europe and North-America, also
in the Latin-American countries, with a high proportion of
European-migration, as Chile and Argentina.
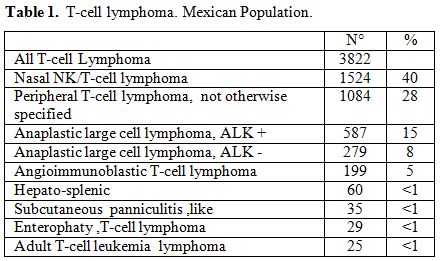 |
Table 1. T-cell lymphoma. Mexican Population. |
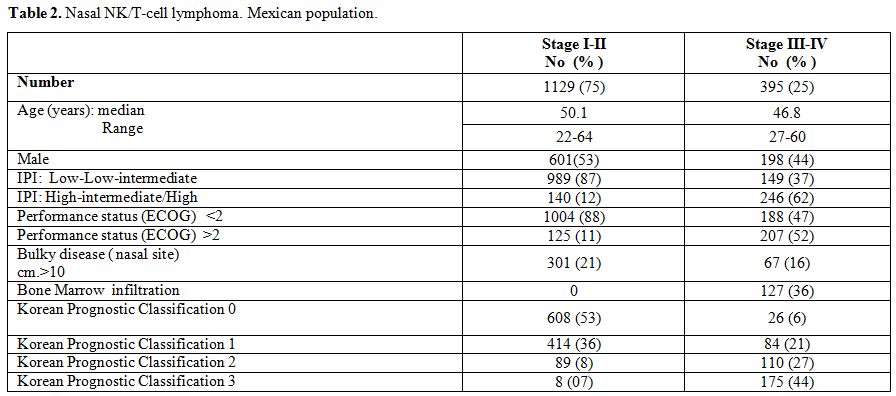 |
Table 2. Nasal NK/T-cell lymphoma. Mexican population. |
 |
Table 3. The outcome from Nasal NK/T-cell lymphoma in the Mexican population. |
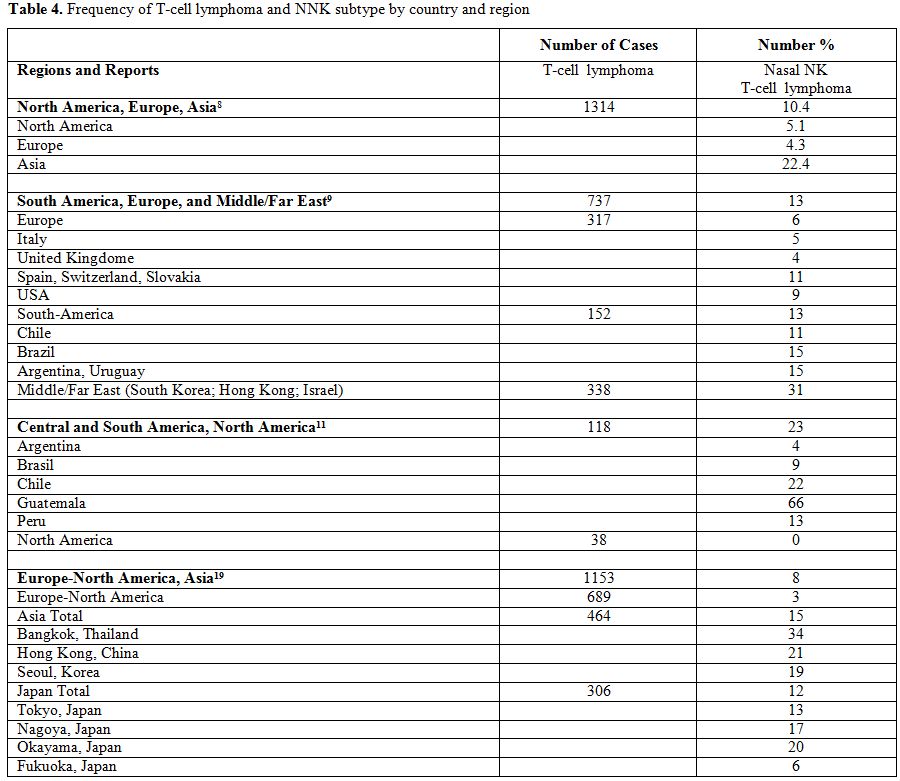 |
Table 4. Frequency of T-cell lymphoma and NNK subtype by country and region |
Discussion
In Mexico, NKTCLs represent the 40% of all T-cell lymphomas, and 10%
of all malignant lymphomas, diagnosed in our hospital. The
International T-cell Project was the first attempt to explore the
geographic variations about the T-cell lymphomas; and specifically of
NKTCL. These results showed that the NKTCLs represent about 10% of the
total of T-cell lymphomas found in North America, Europe, and Asia.[8]
The percentage ranged from 4.3% in Europe to “2.4% in Asia. In the USA,
the percentage was 5.1%. Some years, ago, the study was
repeated in another countries, with small variations In a
subsequent study, also made in the USA, Bellesi et al.[9]
reported that the NKTCLs were the 13% of all 737
cases of T-cell lymphomas, with a percentage ranging from 6% in
Europe and 31% in the Middle/Far East. In the USA, the percentage was
the 9%. Recently Dubal et al., performed a retrospective analysis
of cancer of head and neck in the USA, and found 1382 cases of
sino-nasal lymphomas, but only 328 (23%) were considered that were
NKTCL. Moreover, the analysis for a general population showed that
NKTCLs in the USA represent only 0.032/100,00 habitants.[10] The T-cell Project report that the frequency in European countries, the presence of NKCTLs is rare, 4.3 % of 1314 cases,[8] and subsequently 6.0% of 737 patients.[9] Isolated reports from some European countries has been published: Italy: 26 cases;[12] Portugal: 12 patients, which were analyzed the molecular changes found in these patients.[13]
Marcos-Gragera in a retrospective survival analysis of a different form
of lymphoid neoplasms in European Countries reported that NKTCLs were
not present.[14]
Laurini et al. have presented the incidence of NKTCL in Central and South America in the confrontation with the USA.[11]
In this report these neoplasm represent 0% in the USA
and the 23 % of all T-cell lymphoma (27 cases in 118
cases of T-cell lymphoma) in Central/South America, respectively
13 %(4/31 cases) in Peru, 4.5% (1/22 cases) in Argentina, 9%
(2/18 cases) in Brazil, 22 % (5/22 cases) in Chile, 66% (15/25)
in Guatemala, 13% (4/31) in Perù.[11]
Bellesi et al. reported 9 cases (11%) in Chile, and 8 cases Brazil (15%) among 152 cases found in South America.[9]
Gualco et al. reported 122 Brazilian patients, but they only
analyzed the presence of the subtypes of EBV virus in patients
with NKTCL.[18] However, these differences could be considered to because they were performed in different populations.
The
high rate of frequency of NKTCL in Guatemala, Central America, is
also confirmed by the report of Van der Rijn et al..[15]
In the analysis of neoplasms of head and neck, these authors found that
17 cases (88%) were NKTCL, this search was also able to detect that
many patients were positive for EBV. Although, nasal NK/T-cell
lymphoma shown a higher prevalence of EBV seropositive, the role in the
pathogenesis of nasal NKTCL not has been defined. Other forms of the
chronic EBV-associated disease are not common in the Mexico. Ortega et
al..[16] reported a Mexican study, analyzed 264 cases
of non-Hodgkin’s lymphoma with the nodal and extranodal presentation.
In the extranodal presentation, 55 cases, 16 patients were considered
lymphoma of the midline or centrofacial with
angiocentricity. Thus, we considered that were NKTCLs, even if the
molecular profile was the most important task of this research.[16] Perry et al.[17]
in another report from Guatemala, analyzed 226 patients
with non-Hodgkin’s lymphoma, 25 cases were of T-cell origin,
and 18 (7.9 % of the total of cases) were NKTCL, no other dates
were included.
Conclusion
The number of NKTCL cases found in Mexico was similar to that
found in Guatemala and Peru, and also in China and Korea. Our
study suggests that this neoplasm could have a racial basis, but
environmental factors also had to be considered.
According our experience[5] and of others concomitant/sequential chemotherapy and radiotherapy is the standard treatment.[20] Radiotherapy alone, also for the first stages, is inadequate because of high systemic failure rate.
References
