Comparison of Methicillin Resistant Staphylococcus Aureus in
Healthy Community Hospital Visitors[CA-MRSA] and Hospital Staff
[HA-MRSA]
Nirmal A Pathare1, Sara Tejani1, Harshini Asogan1, Gaitha Al Mahruqi1, Salma Al Fakhri1, Roshna Zafarulla1 and Anil V. Pathare2*
1Oman Medical College and 2Sultan Qaboos University Hospital, Muscat, Oman
Corresponding author: *Dr Anil Pathare, MD, FCPS, FIMSA, Ph.D. Sultan Qaboos University Hospital, PO Box 35, PC 123, Muscat, OMAN. E-mail:
pathare@squ.edu.om
Published: October 7, 2015
Received: August 7, 2015
Accepted: September 18, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015053, DOI
10.4084/MJHID.2015.053
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Background: The prevalence of community-associated methicillin-resistant Staphylococcus aureus [CA-MRSA] is unknown in Oman.
Methods:
Nasal and cell phones swabs were collected from hospital visitors and
health-care workers on sterile polyester swabs and directly inoculated
onto a mannitol salt agar containing oxacillin, allowing growth of
methicillin-resistant microorganisms. Antibiotic susceptibility tests
were performed using Kirby Bauer’s disc diffusion method on the
isolates. Minimum inhibitory concentration (MIC) was determined for
vancomycin and teicoplanin against the resistant isolates of MRSA by
the Epsilometer [E] test. A brief survey questionnaire was requested be
filled to ascertain the exposure to known risk factors for CA-MRSA
carriage.
Results:
Overall, nasal colonization with CA-MRSA was seen in 34 individuals
(18%, 95% confidence interval [CI] =12.5%-23.5%), whereas, CA-MRSA was
additionally isolated from the cell phone surface in 12 participants
(6.3%, 95% CI =5.6%-6.98%). Nasal colonization prevalence with
hospital-acquired [HA] MRSA was seen in 16 individuals (13.8%, 95%
confidence interval [CI] =7.5%-20.06%), whereas, HA-MRSA was
additionally isolated from the cell phone surface in 3 participants
(2.6%, 95% CI =1.7-4.54). Antibiotic sensitivity was 100% to linezolid
and rifampicin in the CA-MRSA isolates. Antibiotic resistance to
vancomycin and clindamycin varied between 9-11% in the CA-MRSA
isolates. Mean MIC for vancomycin amongst CA- and HA-MRSA were 6.3 and
9.3 μg/ml, whereas for teicoplanin they were 13 and 14 μg/ml
respectively by the E-test. There was no statistically significant
correlation between CA-MRSA nasal carriage and the risk factors
(P>0.05, Chi-square test).
Conclusions:
The prevalence of CA-MRSA in the healthy community hospital visitors
was 18 % (95% CI, 12.5% to 23.5%) as compared to 13.8% HA-MRSA in the
hospital health-care staff. Despite a significant prevalence of
CA-MRSA, these strains were mostly sensitive. Recommendation: The
universal techniques of hand washing, personal hygiene and sanitation
are thus warranted.
|
Introduction
Methicillin resistant Staphylococcus aureus [MRSA] has emerged as a
virulent pathogen and is a leading cause of nosocomial infections.[1-3]
Although first reported in 1972, there are increasing number of
hospital outbreaks with increased mortality, morbidity and health care
costs.[4] Furthermore, since 1990s, MRSA has also emerged as cause of infection in the community.[5,6]
Community-acquired MRSA [CA-MRSA] is usually seen in subjects with well
recognized risk factors such as intravenous drug usage, debilitating
co-morbid conditions like diabetes mellitus, malignancies,
cardiovascular or renal failure, etc.[7-11] However, the first reported CA-MRSA was in Australian aboriginals and native Canadians in the 1990s.[12]
The first reported cases of CA-MRSA in the USA were seen with no
contact to health care system in native Americans from Minnesota, North
Dakota and Nebraska as well as in Los Angeles and San Francisco.[13,14]
The
emergence of CA-MRSA in the community is a significant public health
concern as transmission from individual to individual is a primary
health care concern leading to the spread of microorganisms of
significant potential for morbidity and mortality. However, not the
mere presence of CA-MRSA but its antibiotic sensitivity-resistance
pattern plays a significant role in the risk assessment.
Methicillin-resistant strains became more common than
methicillin-susceptible strains, first in hospitals [HA-MRSA] and later
in the community.[3,15] Prevalence
of CA-MRSA is variable, being low in some European countries, whereas,
there is increasing evidence that it is significantly higher in many
other parts of the world.[16,17] Some studies from India have reported a prevalence of CA-MRSA in the range of 4.6–10.6% from a rural setting,[18,19] whereas others like Gaud et al reported CA-MRSA prevalence of 16.4% in an urban setting from Bangalore, in India.[20]
Thus,
in view of the rising trend of the increasing prevalence of CA-MRSA,
and its propensity to develop resistance, it is imperative not only to
study the prevalence of CA-MRSA in Oman, but also its antibiotic
susceptibility and resistance pattern. Unfortunately, the prevalence of
CA-MRSA in Oman is unknown.
Aim of this study
We
initiated this study to screen for CA-MRSA by per nasal and cell phone
swabs as it will give an additional perspective to the Omani health
initiative. Participants were also asked to fill a brief survey
questionnaire to record their age, gender, history of infections, if
any, frequency of hospital visits, as well as the associated co-morbid
conditions like diabetes, hypertension or recent skin/wound infections
and antibiotic exposure.
Patients and Methods
Study design and subjects:
The study design was a prospective cross-sectional cohort study and was
approved by the institutional research and ethics committee.
Participants were enrolled after a written informed consent. The
hospital visitor community and health-care workers from the hospital,
as well as private clinics, were enrolled in the study. Nasal and cell
phones swabs from all participants were inoculated onto a selective
mannitol salt agar with oxacillin with minimum time lapse that would
allow growth of only methicillin-resistant microorganisms. Demographic
data collected included age, gender, and nationality. To assess any
possible risk for MRSA carriage, further data including hospital
exposure, exposure to antibiotics, co-morbidities like diabetes
mellitus, hypertension and skin and soft tissue wounds, etc. was also
collected and recorded. Sample collection and transportation:
Samples were collected from both anterior nares using sterile polyester
swabs with a standard rotating technique. Similarly, the surface of
participant’s personal cell phones were also swabbed using swabs
pre-moistened with sterile saline.[21] These swabs
were used for inoculation of mannitol salt agar containing oxacillin
with minimum time lapse. Colony characteristics on the culture plates
and Gram-staining were used to confirm further the identity of Staphylococcus aureus
that grew on this MRSA selective medium. Gram staining helped to
ascertain that there were no other airborne contaminants by confirming
the characteristic morphology of Staphylococcus aureus. Growth of any other microorganisms were noted but was not included in this analysis. Antibiotic susceptibility tests were performed on Mueller-Hinton agar using Kirby Bauer’s disc diffusion method,[22] according to the Clinical and Laboratory Standards Institute (CLSI) guidelines. S. aureus ATCC 25923 was used as a control strain. The following antibiotics were used: erythromycin (15 μg), clindamycin (2 μg), rifampicin (2 μg), doxycycline (30 μg), vancomycin (30 μg), linezolid (30 μg) and teicoplanin (30 μg).
MIC for vancomycin and teicoplanin were further tested by the
Epsilometer [E] test (Ezy MIC Strip, HIMEDIA India) against resistant
MRSA strains. MIC values were read as per the manufacturers
recommendation and interpretation made as per CLSI criteria.[23] Statistical Analysis:
All the data was analyzed using IBM-SPSS ver 19.0. The prevalence of
MRSA was estimated with 95% confidence intervals. Continuous variable
are reported as mean ±
SD with 95% Confidence Intervals. The correlation between categorical
variables was determined by Chi-Square test for significance.
Statistical significance was identified as p<0.05.
Results
The hospital visitor community comprised of 189 subjects, with a
mean age of 25.43±17.5 years old; most of the subjects were female
(63.5%). The hospital health- care workers comprised of 116 subjects,
with a mean age of 33.23±8.9 years old; the majority of the persons in
this cohort were females (67.2%) (Table 1a).
There was no statistically significant correlation between CA- and HA-
MRSA isolates and the demographic characteristics or the risk factors
namely gender, underlying co-morbidities like diabetes, hypertension,
skin/soft tissue infections, skin ulcers/wounds, recent exposure to
antibiotics, or hospital exposure (Table 1b; P>0.05, Chi-square test).
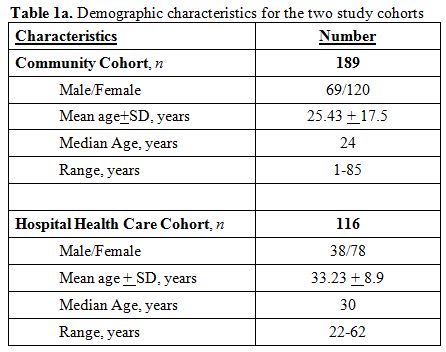 |
Table 1a. Demographic characteristics for the two study cohorts. |
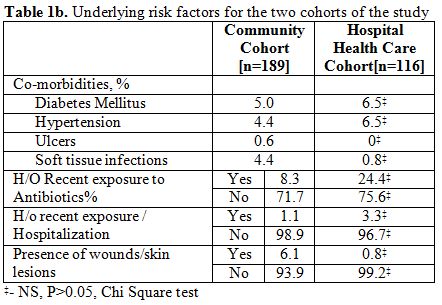 |
Table 1b. Underlying risk factors for the two cohorts of the study |
Overall, in the hospital visitor community, CA-MRSA were
isolated in 34 individuals from their nasal vestibules giving a
carriage rate of 18.0% (95% CI=12.5% to 23.5%). (Table 2)
CA-MRSA was also isolated from the cell phone surfaces in 12
individuals yielding a carriage rate of 6.3% (95% CI=5.6% to 6.98%). In
2 participants (1.06%), CA-MRSA was isolated both from nasal vestibules
and from their cell phone swabs. In the hospital health workers, the
nasal carriage [HA-MRSA] was observed in 16 individuals with a
colonization rate of 13.8% (95% CI=7.5% to 20.06%) and in 3
individuals, cell phone swabs grew HA-MRSA giving a colonization rate
of 2.6% (95% CI=1.7% to 4.54%). However, none of the hospital health
workers showed positive MRSA isolation from nose and cell-phone from
the same individual.
 |
Table 2. Prevalence of CA-MRSA and HA-MRSA isolates in the Community and Health Care staff . |
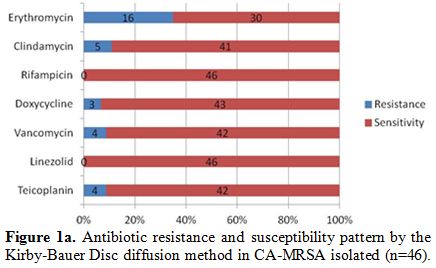
A total of 46 and 19 isolates were respectively obtained and
confirmed as CA-MRSA and HA-MRSA from the culture characteristics and
Gram staining in the community hospital visitors and the hospital
health-care workers. Amongst the CA-MRSA isolates antibiotic resistance
with erythromycin and clindamycin varied between 11-35%, whereas, most
isolates were sensitive to rifampicin, doxycycline, vancomycin,
linezolid, and teicoplanin. (Figure 1a)
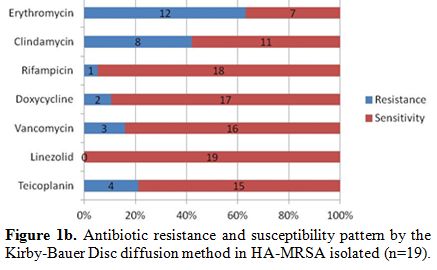
However,
amongst the HA-MRSA isolates, a significantly higher antibiotic
resistance was seen with both erythromycin and clindamycin, varying
between 42-63%, whereas, the sensitivity of HA-MRSA isolates to
rifampicin, doxycycline, vancomycin, and linezolid was 95%, 89%, 84%,
and 100% respectively (Figure 1b). Overall, there was no significant differences in the resistance pattern between the nasal and cell phone CA-MRSA isolates [Table 3;
p>0.05, Chi-square test] Overall, the vancomycin-resistant CA-MRSA
were 2.1%. Mean MIC by the E test for vancomycin amongst CA-MRSA
isolates [n=4] was 6.5 μg/ml with a range between 6 to 8, whereas,
amongst the HA-MRSA isolates [n=3] it was 9.3 μg/ml with a range
between 8 to 12. Mean MIC by the E test for teicoplanin amongst CA-MRSA
isolates [n=4] was 13 μg/ml with a range between 12 to 16, whereas
amongst the HA-MRSA isolates [n=4] it was 14 μg/ml with a range between
12 to 16.
|
|
Figure 1a. Antibiotic resistance and susceptibility pattern by the Kirby-Bauer Disc diffusion method in CA-MRSA isolated (n=46). |
|
|
Figure 1b. Antibiotic resistance and susceptibility pattern by the Kirby-Bauer Disc diffusion method in HA-MRSA isolated (n=19). |
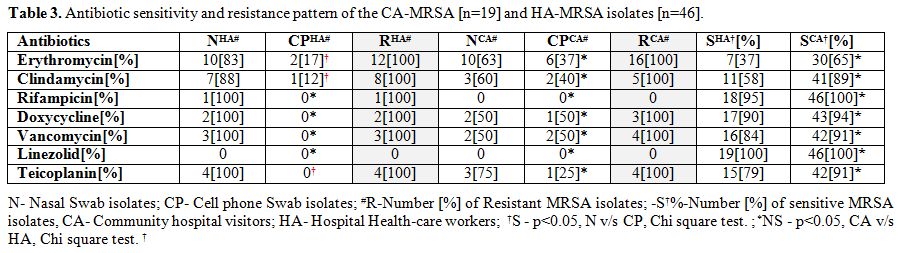 |
Table 3. Antibiotic sensitivity and resistance pattern of the CA-MRSA [n=19] and HA-MRSA isolates [n=46]. |
Discussion
The
prevalence of MRSA in Oman is unknown. This study showed a relatively
higher overall prevalence of CA-MRSA nasal carriage in an urban setting
of 18% as compared to HA-MRSA nasal colonization of 13.8%. Thus,
although the exposure of hospital environment should have led to an
increased prevalence, yet the impact of ongoing hospital infection
control policies and other related activities, like hand washing and
personal hygiene, could have resulted in this relative lower prevalence
over community CA-MRSA nasal carriage. Furthermore, the higher
incidence of CA-MRSA amongst hospital visitors also makes it more
likely to have been acquired in an out of hospital setting. This is in
keeping with the fact that although CA-MRSA is known to be associated
with co-morbidities such as diabetes mellitus, malignancies,
cardiovascular or renal failure,[7-11] is has been also reported in subjects with no contact to health care system.[13,14]
However, the more disconcerting fact is that the vancomycin MIC values
for HA-MRSA by the E-test were much higher than those seen in the
CA-MRSA resistant isolates. All this could have important implications
in the setting of community-acquired nosocomial infections. Literature
review on the prevalence data of CA-MRSA shows an almost 2-fold
increase in prevalence rates in our study in comparison to previous
Indian studies reporting a prevalence of CA-MRSA to range between 4.6%
to10.6%[18,19]. However these reports were from a rural setting in the Indian state of Karnataka, whereas, Gaud et al[20]
reported a CA-MRSA prevalence of 16.4% from an urban setting in
Bangalore, from India. Therefore, it seems that rural CA-MRSA
prevalence is much lower than the urban setting as corroborated by the
prevalence data from our study from an urban setting. In
contrast, the prevalence of cell phone carriage of HA-MRSA was almost
half of the CA-MRSA at 2.3% v/s 6.3% in our study. Lower cell phones
carriage of HA-MRSA was especially important as it indicates the need
to reinforce an awareness campaign in the community to take adequate
care and precautions regarding the universal techniques of hand
washing, personal hygiene, and sanitation. Moreover, contaminations of
inanimate objects like cell phones should also be reduced to minimize
the risk of transmitting CA-MRSA as these organisms are generally
spread by a person to person transmission. Furthermore, the incidence
and nature of antibiotic resistance patterns of CA-MRSA will be a
pivotal issue for further risk assessment and management of these
isolates. Although Staphylococcus aureus
is a commensal organism, it is the most common cause of skin and soft
tissue infections and nosocomial infections and antibiotic resistance
is an ever increasing concern. Furthermore, an outcome of these events
is often pneumonia, wound sepsis, arthritis, endocarditis, or
osteomyelitis leading to an increasing morbidity and mortality.[11,12] The antimicrobial susceptibility profile of S. aureus
and MRSA usually differs depending on the local settings, as seen in
several reports depending on the resistance profiles observed.[3-5,8,19,21,22]
In this study, antibiotic susceptibility tests revealed that a majority
of the CA-MRSA isolates were sensitive to most of the commonly
prescribed antibiotics (Figures 1a and 1b),
and especially as compared to HA-MRSA isolates. However, there was a
significantly high rate of resistance to erythromycin [63%],
clindamycin [42%] and Teicoplanin [21%] amongst the HA-MRSA isolates as
compared to CA-MRSA isolates of 35%, 11% and 9% respectively. Moreover,
it was also noticed that most of this resistance was associated with
the per nasal isolates amongst the HA-MRSA isolates (Table 3).
Most of the HA-MRSA and CA-MRSA isolates were sensitive to rifampicin
[95 v/s 100%], doxycycline [89 v/s 94%], vancomycin [84 v/s 91%] and
linezolid [100% in both]. Only one strain of HA-MRSA showed resistance
to rifampicin and was isolated from the nasal swab in a health care
worker. The four strains of vancomycin resistance in the CA-MRSA
isolates were equally distributed between the nose and cell phones.
However, all the three strains of vancomycin resistance seen in the
HA-MRSA isolates were obtained from a nasal swab of the hospital
health-care staff, and this is a worrisome issue. Overall, the
relatively higher prevalence of resistant HA-MRSA isolates amongst the
hospital health-care staff is significant and needs to be addressed by
the respective hospital infection control committees and protocols. It
is prudent that immediate action is required to reduce the prevalence
of these asymptomatic subjects with resistant HA-MRSA nasal
colonization to protect unsuspecting and unfortunate hospital patients
from being passively exposed and being at risk of possible transmission
of nosocomial MRSA organisms. MRSA nosocomial infection outbreaks can
also be thus prevented by appropriate immediate action and following
the recommended infection control guidelines in the matter in these few
identified cases with resistant MRSA nasal colonization. Fortunately,
the study did not find any multi-drug resistant HA-MRSA isolates.Although no risk factors were identified when CA-MRSA was initially reported,[13,14] several risk factors are generally associated with HA-MRSA isolates.[12,23]
In this study, we also explored several demographic as well as
co-morbid risk factors, but there were no statistically significant
correlations between HA-MRSA and CA-MRSA isolates and the risk factors.
Specifically, we could not demonstrate any association between isolates
of HA- and CA-MRSA and an underlying risk factor for diabetes,
hypertension, skin/soft tissue infection, skin ulcer/wound, recent
exposure to antibiotic, or hospital visit, etc.(P>0.05, Chi-square
test). In
summary, the prevalence of asymptomatic nasal carriage of CA-MRSA was
higher than noted in several previous reports involving community
studies. No risk factors were significantly associated with this high
prevalence. Although limited by the small sample size, a majority of
the CA-MRSA isolates were relatively sensitive as compared to the
HA-MRSA isolates. The very fact that prevalence of cell phone carriage
in the community cohort is substantially higher compared to the health
care worker cohort is a public health concern. It is therefore
recommended that universal measures of hand washing, personal
sanitation and hygiene need utmost attention, especially in the
community and awareness campaign programs need to be implemented
robustly. Acknowledgements
The authors wish to thank Dean, Oman Medical College for providing
necessary research facilities. This work was supported by a FURAP grant
in August 2013 from the ‘The Research Council’ [TRC] of the Sultanate
of Oman. (Grant No. FRP/OMC/13/001).
References
- Appelbaum, P.C, Microbiology of antibiotic
resistance in Staphylococcus aureus. Clinical Infectious Diseases,
2007, Sep 15;45 Suppl 3:S165-70. http://dx.doi.org/10.1086/519474 PMid:17712742

- Popovich
K. J. and Hota B., Treatment and prevention of
community-associated methicillin-resistant Staphylococcus aureus skin
and soft tissue infections, Dermatologic Therapy, 2008:
May-Jun;21(3):167-79
- David
M. Z. and Daum R. S., Community-associated methicillin-resistant
Staphylococcus aureus: epidemiology and clinical consequences of an
emerging epidemic, Clinical Microbiology Reviews, 2010: Jul;23(3):616-87 .
- Tiwari
S, Sahu M, Rautaraya B, Karuna T, Mishra SR, Bhattacharya S, Prevalence
of methicillin resistant Staphylococcus aureus and its antibiotic
susceptibility pattern in a tertiary care hospital, J Indian Med Assoc
2011;109(11):800-1. PMid:22666934
- Dulon
M, Haamann F, Peters C, Schablon A, Nienhaus A. MRSA prevalence in
European healthcare settings: a review. BMC Infect Dis, 2011; May
20;11:138. http://dx.doi.org/10.1186/1471-2334-11-138 PMid:21599908 PMCid:PMC3128047
- Ahmad
Y, Khandelwal S, Nicolson AM, Simms MH. MRSA screening in the vascular
day-case population. Ann R Coll Surg Engl, 2011; Jan;93(1):44-8. Epub
2010 Sep 22,
- Embil
J., Remotar K., Romance L. et al. MRSA in tertiary care institutions on
the Canada prairies 1990-1992. Infect Control Hosp Epidemiol 1994;
Oct;15(10):646-51. http://dx.doi.org/10.2307/30145275
- Saravolatz
L.D., Pohlod D.J., Arking L.M. Community acquired MRSA infections: a
new source of nosocomial outbreaks. Ann Intern Med 1982;97(3):325-9. http://dx.doi.org/10.7326/0003-4819-97-3-325 PMid:7114629
- Saravolatz
L.D., Markowitz N., Arking L., et al. MRSA. Epidemiological
observations during a community acquired outbreak. Ann Intern Med
1982;96(1):11-6. http://dx.doi.org/10.7326/0003-4819-96-1-11 PMid:7053683
- Mulligan
M.E., Murray-Leisure K.A., Standiford H.C. et al. Methicillin-resistant
S. aureus: a consensus review. Am J Med 1993;94(3):313-28. http://dx.doi.org/10.1016/0002-9343(93)90063-U
- Moreno
F., Crisp C., Jorgensen J.H., Patterson J.E. Methicillin-resistant
Staphylococcus aureus as a community organism. Clin lnfect Dis 1995;
Nov;21(5):1308-12
- Ribeiro
J, Boyce JM, Zancanaro PQ, Prevalence of Methicillin-Resistant
Staphylococcus aureus(MRSA) among patients visiting the emergency room
at a tertiary hospital in Brazil. Brazil J. Infect. Dis., 2005;
Feb;9(1):52-5. Epub 2005 Jun 6. http://dx.doi.org/10.1590/S1413-86702005000100009 PMid:15947847
- Herold
B.C., Immergluck L.C., Maranan M.C., et al. Community-acquired
methicillin-resistant Staphylococcus aureus in children with no
identified predisposing risk. JAMA 1998; Feb 25;279(8):593-8. http://dx.doi.org/10.1001/jama.279.8.593 PMid:9486753
- Public
Health Dispatch: Outbreaks of community associated
methicillin-resistant Staphylococcus aureus skin infections - Los
Angeles County, California, 2002-2003. MMWR 2003;52:88.
- Griffiths
C., Lamagni T. L., Crowcroft N. S., Duckworth G., and Rooney C.,
"Trends in MRSA in England and Wales: analysis of morbidity and
mortality data for 1993–2002,"Health Statistics Quarterly, 2004;
Spring;(21):15-22. PMid:15615149
- Stefani
S., Chung D. R., Lindsay J. A. et al., "Methicillin resistant
Staphylococcus aureus (MRSA): global epidemiology and harmonization of
typing methods," International Journal of Antimicrobial Agents, 2012;
Apr;39(4):273-82. Epub 2012 Jan 9 http://dx.doi.org/10.1016/j.ijantimicag.2011.09.030 PMid:22230333
- Skov
R., Christiansen K., Dancer S. J. et al., "Update on the prevention and
control of community-acquired methicillin resistant Staphylococcus
aureus (CA-MRSA)," International Journal of Antimicrobial Agents, 2012;
Mar;39(3):193-200. Epub 2012 Jan 9. http://dx.doi.org/10.1016/j.ijantimicag.2011.09.029 PMid:22226649
- Nagaraju
U., Bhat G., Kuruvila M., Pai G. S., Jayalakshmi A., and Babu R. P.,
"Methicillin-resistant Staphylococcus aureus in community-acquired
pyoderma," International Journal of Dermatology, 2004; Jun;43(6):412-4.
http://dx.doi.org/10.1111/j.1365-4632.2004.02138.x PMid:15186220
- Song
J. H., Hsueh P. R., Chung D. R. et al., "Spread of
methicillin-resistant Staphylococcus aureus between the community and
the hospitals in Asian countries: an ANSORP study,"
Journal of Antimicrobial Chemotherapy, 2011; May; 66(5):1061-9. Epub
2011 Feb 20. http://dx.doi.org/10.1093/jac/dkr024 PMid:21393157
- Goud
R., Gupta S., Neogi U. et al., "Community prevalence of methicillin and
vancomycin resistant Staphylococcus aureus in and around Bangalore,
southern India," Revista da Sociedade Brasileira de Medicina Tropical,
2011; 44, (3), 309–312. http://dx.doi.org/10.1590/S0037-86822011005000035 PMid:21901873
- Landers
TF, Hoet A, and Wittum TE, Swab Type, Moistening, and Preenrichment for
Staphylococcus aureus on Environmental Surfaces, J. clin. Microbial.,
2010, Jun;48(6):2235-6. Epub 2010 Apr 14
- Bauer,
A. W., D. M. Perry, and W. M. M. Kirby. Single disc antibiotic
sensitivity testing of Staphylococci. A.M.A. Arch. Intern. Med. 1959.
Aug;104(2):208-16.
- Clinical
and Laboratory Standards Institute. Performance standards for
antimicrobial susceptibility testing. 21st Informational Supplement.
(M100-S21). Wayne, Pa, USA: Clinical and Laboratory Standards
Institute; 2010.
[TOP]