Role of Biomarkers as Predictors of Infection and Death in
Neutropenic Febrile Patients after Hematopoietic Stem Cell
Transplantation
Karin Massaro1 and Silvia Figueiredo Costa1,2
1 Department of Infectious Diseases, Faculty of Medicine, University of Sao Paulo, Sao Paulo, Brazil
2 Laboratory of Bacteriology-LIM54, Hospital das Clinicas, University of Sao Paulo, Sao Paulo, Brazil
Corresponding author: Silvia F Costa, MD, PhD. Mailing Address: Av. Dr.
Eneas de Carvalho Aguiar, 470 – Sao Paulo, 054030¬-000, Sao Paulo,
Brazil. Tel. +55 11 3061-7030. E-mail:
costasilviaf@ig.com.br
Published: October 15, 2015
Received: June 18, 2015
Accepted: October 2, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015059, DOI
10.4084/MJHID.2015.059
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
An ideal marker in the neutropenic
population after HSCT is the one which positivetes at the onset of
fever, or at most up to 24 hours after its onset, the patients at
potential risk for infection due to bacterial and fungi and mortality.
Several biomarkers have been used in HSCT patients in the last decade.
However, it seems that C-RP and Il-6 are the most useful markers to
early detected infection and risk for death. |
Introduction
The number of hematopoietic stem cell transplantations has increased
significantly over the past decade. The morbidity and mortality due to
infectious complications are the major clinical issue in HSCT
recipients.[1,2] However, the identification of these infectious
complications is still based on clinical criteria, though, mainly in
the occurrence of fever.
In patients after HSCT, it's hard to
set infection apart from other causes of fever, such as acute Graft
versus host diseases (GVHD), or veno-occlusive disease (VOD) and
sinusoidal occlusion syndrome.[3] The detection of these major
transplantation-related complications is essential for the early and
proper introduction of antibiotics, immunomodulators or hemostatic
treatment. The diagnosis and the evolution of infectious complications
may be optimized with the help of early sensitive and specific markers
of bacterial and fungal infections. An ideal marker should preferably
either precede significant microbiological findings or justify an
additional intensive search for an infection focus even in afebrile.[4]
The early prediction of serious bacteremia helps to identify those
patients who are more likely to benefit from a combination of drugs and
reduce the unnecessary toxicity of additional treatments when there is
no need. At the same time, it helps the identification of patients at
low risk of complications, which may be treated at outpatient
units.[5,6]
Main Biomarkers
IL-6.
Interleukin-6 is a pro-inflammatory cytokine produced by several types
of cells, including monocytes, macrophages and endothelial cells. The
main form of IL-6 in human plasma consists of a biologically active 45
kDa molecule.[7]Interleukin-6
(also called hepatocyte stimulating factor), as previously mentioned,
is involved with the production of proteins of the acute phase, such as
C-reactive protein (CRP).[8] The production and secretion of IL-6 may
be induced by a great variety of stimuli, including infection by
Gram-positive and Gram-negative bacteria, viruses, lipopolysaccharides,
TNF-α, interleukin 1β, gamma interferon and platelet-derived growth
factor.[9-11]The kinetics of this cytokine is very fast (induction in
less than 1-2 hours), but concentrations may decline within very short
time.IL-6
does not react specifically to an infectious stimulus (it increases
both in viral infections and bacterial ones, and in other situations,
such as autoimmune disease and tissue trauma) and presents considerable
fluctuations in daily levels, suggesting temporary activation or
suppression of the immune reaction.[12]C-reactive protein.
The CRP is an acute phase protein, whose serum concentration is
remarkably increased right after the occurrence of aggression to the
body. Its plasma concentrations are usually below 10 mg/L.[13] It is
formed by a complex constituted by five polypeptide subunits
synthesized by the liver, not covalently bonded, with an approximate
molecular weight between 115 kDa and 140 kDa. The
main stimulus mediator to the production of CRP is IL-6; however, other
cytokines, such as IL-1 and TNF-α are also involved in the
process.[14-15] Since IL-6 is the main response mediator of the acute
phase, many clinical conditions, besides inflammation, may cause a rise
in the CRP. Additionally, CRP has the disadvantage of not raising above
its reference top level, prior to 8-12 hours after the onset of the
inflammatory process.[16]Procalcitonin.
Procalcitonin (PCT) is a 14 kDa protein, coded by gene Calc-1, together
with calcitonin and katacalcin (KC). It consists of 114 to 116 amino
acids. It is usually found in the C cells of the thyroid, as a
pre-hormone of calcitonin. However, in 1993, it was found that serious
bacterial infections caused a dramatic release of PCT in the
extracellular space. The concentrations of the soluble protein in the
serum or plasma, in the normal population, are usually below 0.1 ng/mL
(normal range). In case of levels above 0.5 ng/mL, the diagnosis of
sepsis must be considered.[17] In a study in which we provided dosages
of PCT and CRP in 52 inpatients, with hemopathies and febrile
neutropenia, the PCT average was significantly higher in cases with
serious infection (6.7 ng/mL versus 0.6 ng/mL).[18] By using a cut-off
value of PCT, above 0.245 ng/mL, we observed a 100% of sensitivity and
69.2% of specificity in serious infection, suggesting the use of PCT as
a diagnostic marker for severe systemic infection in this population,
to the detriment of CRP. This cut-off value was lower than that of the
study by Giamarellou et al. (0.5 ng/mL) in 2004.[19] The
pharmacokinetic properties of PCT enable its early use (within six
hours), as well as its follow-up (from 24 hours on) as infection and
inflammation marker. Another interesting characteristic of this
molecule is that its half-life is independent of the renal function.[20]IL-8.
IL-8 is known as a pro-inflammatory cytokine, which is involved in
local and systemic inflammatory reactions. Short and high peaks were
observed a few days after VOD.[21] IL-8 can be released by endothelial
cells activated in response to TNF-α and it is a potent activator of
neutrophils, which may contribute to tissue damage.[22] Studies of Biomarkers of Infection in Febrile Neutropenia after HSCT
PCT, IL-6 and CRP cannot be utilized to differentiate Systemic
Inflammatory Response Syndrome (SIRS) from infection, in patients who
receive ATG or similar within up to three days after the application of
the drug. PCT, CRP and IL-6 have limited value in the diagnosis of
infection during the administration of ATG or other anti T-cell
antibodies, such as OKT-3.[23] On the other hand, Blijlevens et al.
(2000)[24] found increased levels of PCT in isolated cases of GVHD.
Procalcitonin.
There can be a slight induction of PCT after HSCT, as when it occurs in
chemotherapy, with levels rarely above 0.5 to 1 ng/mL. That was
observed, for instance, in children with ALL, AML, NHL with B and LH
cells.[25] In cases of serious infections or sepsis, these patients may
also induce high levels of PCT. If neutropenia is severe, the induction
of PCT is reduced; however, the synthesis is not totally
suppressed.[26-27] Some considerations must be made to justify the
different results in two of the studies mentioned. In the study by
Blijlevens et al. (2000),[24] the limited number of patients harmed the
statistical analysis of the results. Zintl et al. (1996)[28] showed, in
a study with patients submitted to HSCT with prior myeloablative
chemotherapy, that PCT increases in systemic bacterial infections and
is strictly related to the septic shock and also that higher levels
indicate bad prognosis. A study that evaluated PCT in neutropenic
hematological patients with mucositis revealed that it represents an
important tool to predict the occurrence of major infections in
patients with febrile neutropenia, even in the presence of associated
complicating conditions, such as mucositis and GVHD.[29] A lower
threshold value (e.g. PCT > 0.25 ng/mL) increases the diagnostic
reliability in case of a serious infection, even in patients with
neutropenia.[30-31] This reduced increase may happen since the adhering
monocytes, among other factors, are necessary for the induction of PCT.
Even if the immune response is overall weakened in neutropenic
patients, and also by the use of corticosteroids or cyclosporine for
the treatment of autoimmune diseases or after transplantation, the
induction of PCT is not totally suppressed.[32] In case of neutropenia,
the severity of the systemic inflammatory response cannot often be
evaluated, since the “fever” symptom is weakly associated with the
gravity of the sepsis or prognosis of the disease. In an international
multicentric study, 158 patients with neutropenia and fever were
evaluated.[19] A cut-off value of 5 ng/mL determined a sensitivity and
specificity for the diagnosis of severe sepsis of 83% and 100%
respectively. In concentrations below 0.5 ng/mL, the severe infection
would be unlikely. In case of fungal infections, the levels of PCT were
1.17 ± 0.44 ng/mL on the first day of diagnosis, with a quick downward
trend. Twelve patients died. On the first day of fever, they had levels
of PCT of 20.45 ± 4.48 ng/mL (average, standard deviation). Similar
data were reported in other studies. [24,26,33] A study that compared
the value of PCT, neopterin, CRP, IL-6 and IL-8, as diagnostic markers
for such purpose, showed an area under the ROC curve in the distinction
of bacteremia by Gram-negative from all the other causes of fever of
0.863 (IC 95% 0.74-0.98) and results not significant for the other
markers.[34]
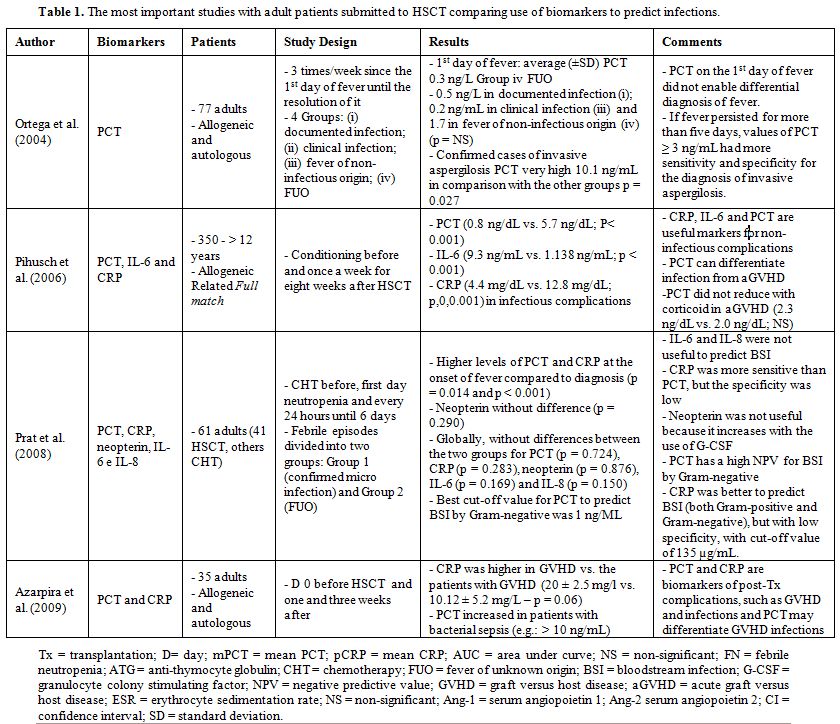
Ortega et al. (2004)[35] showed PCT levels in
patients after HSCT with FUO of 0.3 ± 0.2 ng/mL (average, standard
deviation), and with infections microbiologically documented in the
range of 0.5 ± 0.7 ng/mL. In cases of extended fever (over five days)
and on suspicion of aspergillosis, the levels of PCT were even higher
(10.1 ± 6.7 ng/mL).
In a recent study that evaluated the
relevance of ultrasensitive CRP and PCT levels in patients after HSCT,
it was verified that the ultrasensitive CRP was higher in the patients
with aGVHD and also in the cases of sepsis. The increased levels of PCT
were associated only with a bacterial infection. Only the levels of PCT
could be used to differentiate infection from other complications
related to transplantation.[36] In the study mentioned, PCT, besides
not increasing in GVHD, did not increase in fungal infections, although
the bias of that study was the size of the sample (n = 35).
C-reactive protein.
A study with adult patients submitted to allogeneic HSCT (n = 137)
showed that the pre transplantation CRP and serum ferritin levels can
be predictors of bacterial complications.[37] This study has the
limitations of being retrospective, without standardization of
different hematological diseases and limited number of samples.
Likewise, Pihusch et al. (2006)[38] found high CRP levels both in
infections after HSCT and in aGVHD cases. In this study, which analyzed
the levels of PCT, CRP, and IL-6, prospectively, in 350 patients after
HSCT, conditioning of some patients included anti-thymocyte globulin
(ATG). It is well known that ATG, which is a pool of heterologous
antibodies against T-cells of direct form (opsonization and lysis via
complement activation), causes early increase of TNF-α, CRP, IL-6 and
PCT (few minutes after administration).[23,39]
Interleukin-6 (IL-6).
Some studies show that IL-6 is a sensitive marker for acute infections
in febrile neutropenia and it can be used as a marker of unfavorable
results in this situation.[40-42]
The values of IL-6 (measured
by the Enzyme-linked immunosorbent assay [ELISA] method) for febrile
neutropenia vary in several studies. In the study by Steinmetz et al.
(1995),[8] the level of detection threshold was of 3 pg/mL, with
intratest variations of < 15% (in the 3-100 pg/mL range) and <
20% for values > 100 pg/mL. A significant increase of IL-6 was
considered as an increase higher than 20 pg/mL or 30% for levels <
100 pg/mL and ≥50 pg/mL or 20% for levels > 100 pg/mL. A cut-off
value of IL-6 of 297 pg/mL presented sensitiveness of 62%, positive
predictive value (PPV) of 50% and negative predictive value (NPV) of
70% (p = 0.016) for the identification of infection in neutropenic
patients.[33]
Interleukin-8 (IL-8).
The rapid increase of IL-6 and IL-8, quickly detectable on the first
days after the HSCT, may either be the mere reflection of the severity
of the inflammatory response or it may indicate the deleterious
synergic effect of these cytokines on tissues. In the study by
Schots,[22] the multivariate analysis showed that the increase of these
cytokines, especially IL-8, was associated with a fatal result in HSCT.
There is also a study that relates IL-8 to the adult respiratory
distress syndrome.[43]
The study by Prat et al. evaluated
several biomarkers (PCT, CRP, neopterin, IL-6 and IL-8) in 61 adults
(with 41 submitted to HSCT, and the other ones only under
chemotherapy). IL-6 and IL-8 did not prove useful to prevent
bloodstream infection before chemotherapy, on the first day of
neutropenia nor subsequent days.[34]
|
|
Table 1. The most important studies with adult patients submitted to HSCT comparing use of biomarkers to predict infections. |
Studies of Inflammation Marker and Poor Prognosis (Death) Related to HSCT
An ideal death marker in the neutropenic population after HSCT is
the one that indicates, at the onset of fever, or at most up to 24
hours after, the patients under potential risk of death
transplant-related. There are few studies in literature to help the
prediction of the prognosis of patients submitted to HSCT and the
existing studies evaluate a small number of subjects. The following
table shows the main studies that evaluated death predictors after HSCT
(Table 2). The studies
published about the prognosis in patients after HSCT are divided into
allogeneic or autologous. Despite the advance in supporting treatment,
the allogeneic HSCT still presents high toxicity, with mortality
related to transplantation between 10-50% due to major complications
during the first months after transplantation (infections, VOD, GVHD
and pneumonitis).
|
|
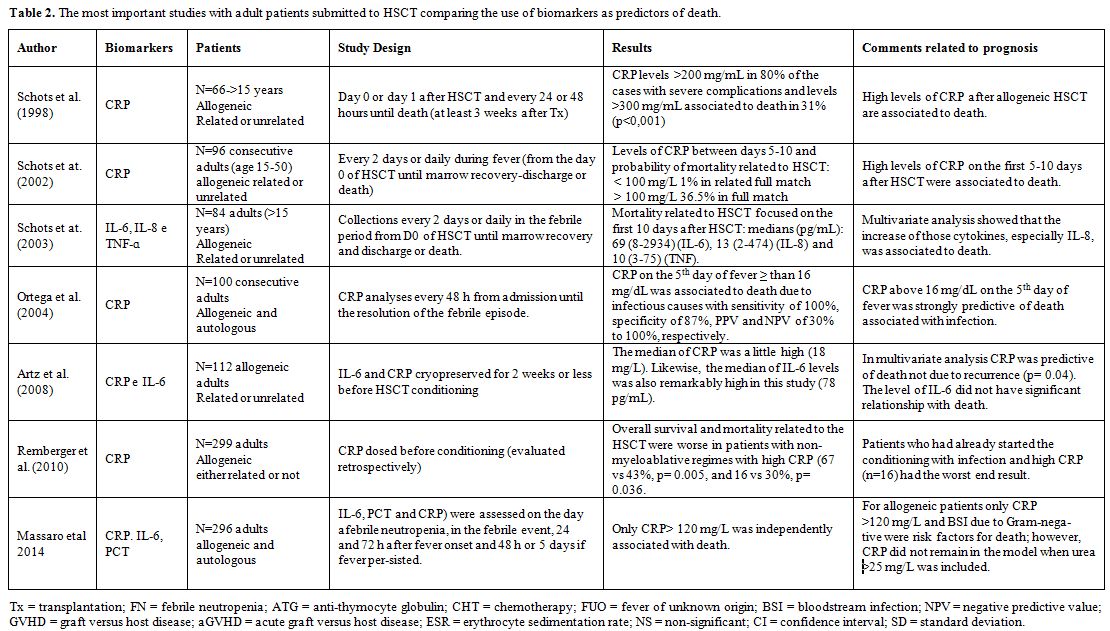
Table 2. The most important studies with adult patients
submitted to HSCT comparing the use of biomarkers as predictors of
death. |
In a prospective study of 296 patients submitted to HSCT at
our university hospital, IL-6, PCT and CRP were evaluated on the day of
confirmed neutropenia, on the day of the febrile event, 24 and 72 hours
after its onset, and 48 hours or 5 days, in case the fever,
persisted.[44] The patients were evaluated after the discharge or death
within 30 days from the HSCT. Only CRP ≥120 mg/L was independently
associated with death. The other risk factors associated with death in
the multivariate analysis were: type of transplantation (allogeneic and
unrelated), bloodstream infection by Gram-negative, LDH≥390 IU/L and
urea ≥25 mg/dL. For allogeneic patients, only CRP≥120mg/L and
bloodstream infection by Gram- negative were risk factors for death. No
independent risk factor was evidenced for the subgroup of autologous
patients. We could not demonstrate the association between IL-6 and PCT
and death. Other authors demonstrated similar results, however, in
studies with a smaller number of cases and or without multivariate
analyzes or testing only one or two biomarkers.[21,22,35,37] Artz et
al.[42] utilized multivariate analysis, however, with a smaller number
of patients (n = 112) and only analyzed two markers (CRP and IL-6) in
allogeneic HSCT. In their study, the median of CRP was 18 mg/L, and of
IL-6 was 78 pg/mL, showing that high levels of CRP, but not of IL-6,
before the conditioning for HSCT, were independent predictors of death
related to allogeneic transplantation. The study of Remberger et al.
(2010),[21] despite including a large number patients, 299, was
retrospective, without multivariate analysis and, likewise the two
previous ones, evaluated only CRP in allogeneic HSCT before the
conditioning. The authors showed that mortality related to
transplantation was lower in patients with non-myeloablative regimens
with high CRP (67 vs 43%, p = 0.005, and 16 vs 30%, p = 0.036).
Finally, the study by Ortega et al. (2004)[35] analyzed only CRP, did
not utilize multivariate analysis and the number of 100 (smaller than
that of the present study), in autologous and allogeneic patients, and
showed that CRP on the 5th day of
fever ≥ 16 mg/dL was associated with death, due to infectious causes
with a sensitivity of 100%, a specificity of 87%, PPV and NPV of 30 and
100%, respectively.
Schots et al. (2002)[22] monitored the levels
of CRP and other variables in 96 consecutive adults submitted to
allogeneic HSCT, dosing from day 0 to +5. Only the high levels of CRP
(> 50 mg/L) (p < 0.001) and type of allogeneic donor (p = 0.02)
were the independent factors for mortality related to transplantation.
The retrospective study of Remberger et al. (2010)[21], evaluated the
clinical impact of CRP in allogeneic HSCT patients, before the
conditioning (n = 205) and after the not-myeloablative and
myeloablative conditioning regimens (n = 299). There was a significant
correlation between CRP levels in both groups with overall survival and
mortality related to transplantation increased in individuals who had
received non-myeloablative conditioning. Early death by infection
(within 100 days) resulted in 25 and 8.7% of patients with high CRP
with and without documented infection, respectively (p < 0.001 and p
= 0.04), compared to patients with normal CRP, where early death by
infection occurred in 2.3% of patients. Remberger et al. (2010)[21]
concluded that CRP may be utilized as a prognostic factor because it
enables the identification of infection in earlier stages, as also
observed in our results. In the studies by Pihusch et al., the serum
levels of CRP (5.2 mg/dL vs 7.8 mg/dL, p < 0.001), IL-6 (147 ng/mL
vs 494 ng/mL; p < 0.001) and PCT (2.1 ng/mL vs 4.0 ng/mL; p = 0.003)
were high until week +2 in the group of patients who died of
complications related to transplantation, compared to the group that
survived.
Perspectives
The
treatment of febrile neutropenic patients after HSCT requires proper
and early diagnosis. Thus, biomarkers can be very useful to control the
antibiotic use in this setting. Sensitive and specific lab markers in
differentiating the infectious and non-infectious origin of the fever
may help the proper use of antibiotics, thus leading to cost reduction.
Until now, however, the role of biomarkers as tools in the conduction
of the febrile neutropenia is questionable. The latest guide from the
Infectious Disease Society of America (IDSA) does not recommend the use
of those biomarkers.[
45] Therapeutic decisions are still based on the
combination of anamnesis, physical examination and microbiological
tests. An ideal marker is the one that can be easily obtained from
clinical specimens, before the development of severe sepsis. It should
not be influenced by cytopenias or inflammatory states associated with
the underlying disease.
Besides, it is always hard to correlate
laboratory findings and clinical events, mainly in such peculiar
population. An ideal marker should be easily detected in blood samples
obtained before the development of more severe sepsis and should not be
influenced by cytopenias, drugs, or by the inflammatory reaction to the
underlying disease. IL-8 is also a marker studied quite often but does
not have these characteristics.
References
- Ochs L, Shu XO, Miller J, Enright H, Wagner J,
Filipovich A. Late infections after allogeneic bone marrow
transplantation: comparison of incidence in related and unrelated donor
transplant recipients. Blood. 1995; 86: 3979-86.

- Sorely JS, Shea TC. Prevention of infections in bone marrow transplant recipients. Infect Dis Clin North Am. 1997; 11:459-77. http://dx.doi.org/10.1016/S0891-5520(05)70365-2
- Südhoff
T, Giagounidis A, Karthaus M. Evaluation of neutropenic fever: value of
serum and plasma parameters in clinical practice. Chemotherapy. 2000;
46: 77-85. http://dx.doi.org/10.1159/000007259
- Belesso
M, Costa SF, Chamone DAF, Dorlhiac-Llacer PE. Triagem para o tratamento
ambulatorial da neutropenia febril. Rev Bras Hematol Hemoter. 2010;
32(5):402-8. http://dx.doi.org/10.1590/S1516-84842010000500014
- Kern WV. Risk assessment and treatment of low-risk patients with febrile neutropenia. Clin Infect Dis. 2006; 42:533-40. http://dx.doi.org/10.1086/499352
- Matsuda
T, Hirano T, Nagasawa S. Identification of alpha2-macroglobulin as a
carrier protein for IL-6. J Immunol. 1989; 142:148-52.
- Steinmetz
HT, Herbertz A, Bertram M, Diehl V. Increase in interleukin-6 serum
level preceding fever in granulocytopenia and correlation with death
from sepsis. J Infect Dis. 1995; 171(1):225-8. http://dx.doi.org/10.1093/infdis/171.1.225 PMid:7798669
- Lowry
SF, Moldawer LL. Cytokines and cytokines antagonists in sepsis and
critical illness. In: Vincent JL (ed). Yearbook on intensive care and
emergency medicine. Berlin, Springler Verlag, 1992, pp 36-43. http://dx.doi.org/10.1007/978-3-642-84734-9_4
- Johnson
K, Choi Y, De Groot E. Potential mechanisms for a proinflammatory
vascular cytokine response to coagulation activation. J Immunol. 1998;
160:5130-5 .
- Van Snick J. Interleukin-6: An overview. Ann Rev Immunol. 1990; 8: 253-78. http://dx.doi.org/10.1146/annurev.iy.08.040190.001345
- Oberhoffer
M, Karzai W, Meier-Hellmann A, Bogel D, Fabetabinder J, Reinhart K.
Sensitivity and specitivity of various markers of inflammation for the
prediction of tumor necrosis factor-alpha and interleukin-6 in patients
with sepsis. Crit Care Med. 1999; 27(9):1-10. http://dx.doi.org/10.1097/00003246-199909000-00018
- Pepys
MB, Baltz ML. Acute phase proteins with special reference to C-reactive
protein and related proteins (pentraxins) and serum amyloid A protein.
Adv Immunol. 1983; 34:141-212. http://dx.doi.org/10.1016/S0065-2776(08)60379-X
- Sim
JE, March CD, Cosman D. cDNA expression cloning of the IL-1 receptor, a
member of the immunoglobulin super-family. Science. 1988; 241:585-9. http://dx.doi.org/10.1126/science.2969618
- Castell
JV, Gomes-Lechon MJ, David M. Hepatology 1990; Acute phase response of
human hepatocytes: regulation of acute-phase protein synthesis by
inteleukin-6. Hepatology. 1990; 12:1179-86. http://dx.doi.org/10.1002/hep.1840120517 PMid:1699862
- Meisner
M, Tschaikowsky K, Palmers T. Procalcitonin and CRP in septic shock:
Inflammatory parameters with different kinetics. Abstr. Intensive Care
Med. 1996; 22:14. http://dx.doi.org/10.1007/BF01921188
- Meisner M. Procalcitonin- biochemistry and clinical diagnosis. Bremen: UNI-MED Verlag AG, 2010.
- Massaro
KS, Costa SF, Leone C, Chamone DA. Procalcitonin (PCT) and C-reactive
protein (CRP) as severe systemic infection markers in febrile
neutropenic adults.BMC Infect Dis. 2007 Nov 22;7:137. http://dx.doi.org/10.1186/1471-2334-7-137 PMCid:PMC2217552
- Giamarellou
H, Giamarellos-Bourboulis EJ, Repoussis P, Galani L, Anagnostopoulos N,
Grecka P. Potential use of procalcitonin as a diagnostic criterion in
febrile neutropenia: experience from a multicentre study. Clin
Microbiol Infect. 2004; 10:628-33. http://dx.doi.org/10.1111/j.1469-0691.2004.00883.x PMid:15214875
- Meisner
M, Schmidt J, Huttner H, Tschaikowsky K. The natural elimination rate
of procalcitonin in patients with normal and impaired renal function.
Intensive care Med. 2000; 26(Suppl. 2):S212-6. http://dx.doi.org/10.1007/s001340051146
- Remberger
M, Ringden O. Serum levels of cytokines after bone marrow
transplantation: increased IL-8 levels during severe veno-occlusive
disease of the liver. Eur J Haematol 1997; 59:254-262. http://dx.doi.org/10.1111/j.1600-0609.1997.tb00985.x PMid:9338624
- Schots
R, Kaufman L, Van Riet I, Lacor P, Trullemans F, De Waele M, Van, Camp
B. Monitoring of C-reactive protein after allogeneic bone marrow
transplantation identifies patients at risk of severe
transplant-related complications and mortality. Bone Marrow
Transplantation 1998; 22:79-85. http://dx.doi.org/10.1038/sj.bmt.1701286 PMid:9678800
- Brodska
H, Drabek T, Malickova K, Kazda A, Vitek A, Zima T, Markova M. Marked
increase of procalcitonin after the administration of anti-thymocyte
globulin in patients before hematopoietic stem cell transplantation
does not indicate sepsis: a prospective study. Crit Care. 2008;
13(2):1-7.
- Blijlevens
NMA, Donnelly JP, Meis FGM, De Keizer MH, De Pauw BE. Procalcitonin
does not discriminate infection from inflammation after allogeneic bone
marrow transplantation. Clin Diagn Lab Immunol. 2000; 7(6):889-92. http://dx.doi.org/10.1128/cdli.7.6.889-892.2000
- Fleischhack
G, Kambeck I, Cipic D, Hasan C, Bode U. Procalcitonin in paediatric
cancer patients: its diagnostic relevance is superior to that of
C-reactive protein, interleukin 6, interleukin 8, soluble interleukin 2
receptor and soluble tumour necrosis factor receptor II. Br J Haematol.
2000; 111(4):1093-102. http://dx.doi.org/10.1046/j.1365-2141.2000.02458.x PMid:11167745
- Hambach
L, Eder M, Dammann E, Schrauder A, Sykora KW, Dieterich C. Diagnosis
value of procalcitonin serum levels in comparison with C-reactive
protein in allogeneic stem cell transplantation. Haematologica. 2002;
87:643-51. PMid:12031922
- Sauer
M, Tiede K, Fuchs D, Gruhn B, Berger D, Zintl F. Procalcitonin,
C-reactive protein, and endotoxin after bone marrow transplantation:
identification of children at high risk of morbidity and mortality from
sepsis. Bone Marrow Transplantation. 2003; 31:1137-42. http://dx.doi.org/10.1038/sj.bmt.1704045 PMid:12796793
- Zintl
F, Sauer M, Fuchs D, Hermann J, Reinhart K. High serum procalcitonin
(PCT) concentrations in children and adults after hemopoietic stem cell
transplantation (HSCT) - An indicator for poor prognosis in severe
infections. Blood. 1996; 88 (suppl. 1):266.
- Sarmati
L, Beltrame A, Dori L, Maffongelli, Cudillo L, De Angels G, Picardi A,
Ottaviani L, Cefalo MG, Venditti A, Amadori S, Arcese W, Andreoni M.
Procalcitonin is a reliable marker of severe systemic infection in
neutropenic haematological patients with mucositis. Am J Hematol. 2010;
85(5):380-3. http://dx.doi.org/10.1002/ajh.21685
- Engel
A, Steinbach G, Kern P, Kern WV. Diagnostic value of procalcitonin
serum levels in neutropenic patients with fever: comparison with IL-8.
Scand J Infect Dis. 1999; 31:185-9. http://dx.doi.org/10.1080/003655499750006254
- Schüttrumpf
S, Binder L, Hagemann T, Berkovic D, Trümper L, Binder C.
Procalcitonin: a useful discriminator between febrile conditions of
different origin in hemato-oncological patients? Ann Hematol. 2003;
82:98-103.
- Rinaldi
S, Adembri C, Grechi S, De Gaudio R. Low-dose hydrocortisone during
severe sepsis: effects on microalbuminuria. Crit Care Med. 2006;
34:2334-9. http://dx.doi.org/10.1097/01.CCM.0000233872.04706.BB PMid:16850006
- von
Lilienfeld-Toal M, Dietrich MP, Glasmacher A, Lehmann L, Breig P, Hahn
C. Markers of bacteremia in febrile neutropenia patients with
hematologic malignancies: procalcitonin and IL-6 are more reliable than
CRP. J Clin Microbiol Infect Dis. 2004; 23:539-44.
- Prat
C, Sancho JM, Dominguez J, Xicoy B, Gimenez M, Ferra C. Evaluation of
procalcitonin, neopterin, C-reactive protein, IL-6 and IL-8 as a
diagnostic marker of infection in patients with febrile neutropenia.
Leuk Lymphoma. 2008; 49:1752-61. http://dx.doi.org/10.1080/10428190802258956
- Ortega
M, Rovira M, Filella X, Almela M, de la Bellacasa JP, Carreras E.
Prospective evaluation of procalcitonin in adults with febrile
neutropenia after hematopoietic stem cell transplantation. Brit J
Hematology. 2004; 126:372-8. http://dx.doi.org/10.1111/j.1365-2141.2004.05053.x
- Azarpira
N, Ramzi M, Aghdaie M, Daraie M. Procalcitonin and C-reactive protein
serum levels after hematopoietic stem-cell transplant. Exp Clin
Transplant. 2009; 2:115-8.
- Kanda
J, Mizumoto C, Ichinohe T, Kawabata H, Saito T, Yamashita K, Kondo T,
Takakura S, Ichiyama S, Uchiyama T, Ishikawa T. Pretransplant serum
ferritin and C- reative protein as predictive factors for early
bacterial infection after allogeneic hematopoietic cell
transplantation. Bone Marrow Transplant. 2010; 3:1-9.
- Pihusch
M, Pihusch R, Fraunberger P. Evaluation of C-reactive protein,
interleukin-6, and procalcitonin levels in allogeneic hematopoietic
stem cell recipients. Eur J Haematol. 2006; 76(2):93-101. http://dx.doi.org/10.1111/j.0902-4441.2005.00568.x
- Dornbusch
HJ, Strenger V, Kerl R, Lackner H, Schwinger W, Sovinz P, Urban C.
Procalcitonin and C-reactive protein do not discriminate between
febrile reaction to anti-T- lymphocyte antibodies and Gram-negative
sepsis. Bone Marrow Transplant. 2003; 32:941-5. http://dx.doi.org/10.1038/sj.bmt.1704265 PMid:14561996
- Tegg
EM, Griffiths AE, Lowenthal RM, Tuck DM, Harrup R, Marsden KA, Jupe
DML, Ragg S, Matthews JP. Association between high interleukin-6 levels
and adverse outcome after autologous haemopoietic stem cell
transplantation. Bone Marrow Transplantation 2001; 28:929-933. http://dx.doi.org/10.1038/sj.bmt.1703272 PMid:11753546
- Erten
N, Genc S, Besisik SK, Saka B, Karan MA, Tascioglu C. The predictive
and diagnostic values of procalcitonin and C-reactive protein for
clinical outcome in febrile neutropenic patients. J Chin Med Assoc.
2004; 67:217-21. PMid:15357107
- Artz
AS, Wickrema A, Dinner S, Godley LA, Kocherginsky M, Odenike O, Rich
ES, Stock W, Ulaszek J, Larson RA, van Besien K. Pretreatment
C-Reactive protein is a predictor for outcomes after reduced-intensity
allogeneicHematopoietic cell transplantation. Boil Blood Marrow
Transplant. 2008; 14:1209-1216. http://dx.doi.org/10.1016/j.bbmt.2008.08.004 PMid:18940674
- Donnelly
SC, Strieter RM, Kunkel SL, Walz A, Robertson CR, Carter DC.
Interleukin-8 and development of adult respiratory distress syndrome in
at-risk patients groups. Lancet 1993;341:643-647. http://dx.doi.org/10.1016/0140-6736(93)90416-E
- Zahid
MF, Ali N, Shaikh MU, Adil SN. Outcome of allogeneic hematopoietic stem
cell transplantation in patients with hematological malignancies. Int J
Hematol Oncol Stem Cell Res. 2014;8(4):30-8. PMid:25774265
- Massaro
KS, Macedo R, de Castro BS, Dulley F, Oliveira MS, Yasuda MA, Levin AS,
Costa SF. Risk factor for death in hematopoietic stem cell
transplantation: are biomarkers useful to foresee the prognosis in this
population of patients? Infection. 2014;42(6):1023-32. http://dx.doi.org/10.1007/s15010-014-0685-2 PMid:25263811
- Freifeld
AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, Raad II,
Rolston KV, Young J-A H, Wingard JR. Clinical Practice Guideline for
the use of antimicrobial agents in neutropenic patients with cancer:
2010 update by the Infectious Diseases Society of America. CID. 2011:
52(4):e56-93. http://dx.doi.org/10.1093/cid/cir073 PMid:21258094
[TOP]