Prasanta Purohit1, Siris Patel1, Pradeep Kumar Mohanty1, Padmalaya Das2 and Jogeswar Panigrahi3
1 Sickle
Cell Clinic and Molecular Biology Laboratory, Veer Surendra Sai
Institute of Medical Sciences and Research (VIMSAR), Burla, Sambalpur,
Odisha, India
2 Department of Infectious Disease, Asian Institute of Public Health, Bhubaneswar, India
3 School of Life Sciences, Sambalpur University, Jyotivihar, Burla, Odisha, India
Corresponding
author: Prasanta Purohit. Senior Research Fellow. Sickle Cell Clinic
and Molecular Biology Laboratory, Veer Surendra Sai Institute of
Medical Sciences and Research (VIMSAR), Burla, Sambalpur, Odisha,
India. Tel: +91-97781-18055; Fax: +91-663- 2432624. E-mail:
prasanta.biochem@gmail.com
Published: November 1, 2016
Received: July 10, 2016
Accepted: October 14, 2016
Mediterr J Hematol Infect Dis 2016, 8(1): e2016055, DOI
10.4084/MJHID.2016.055
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by-nc/4.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
Sickle cell anemia (SCA) and Plasmodium falciparum
malaria are two major public health problems in the state of Odisha,
India. The prevalence of sickle cell gene in the western part of Odisha
is 13.1%,[1] P. falciparum
contributes 23% of cases and 15% of malaria-related deaths in India.
Various African studies have shown that, even though SCA protects from P. falciparum infection, the risk of severe illness and death due to malaria is higher.[2,3] Though several factors are responsible for the disease severity in P. falciparum malaria
in patients with SCA, it was recently found that fetal hemoglobin
(HbF), a physiological hemoglobin usually found higher in patients with
SCA had a negative epistatic interaction with HbS during protection
against malaria.[4] The role of HbF against P. falciparum malaria
in cases with normal hemoglobin genotypes has been widely studied and
found to be protective against severe disease manifestation. So it is
necessary to investigate this association in the regions with high
prevalence of sickle cell gene and high endemicity of P. falciparum malaria. This study aims to find out the effect of HbF level on the clinical manifestation of severe P. falciparum malaria in patients with SCA.
This
prospective study was undertaken at the Sickle Cell Clinic and
Molecular Biology Laboratory, Veer Surendra Sai Institute of Medical
Sciences and Research, Burla, Odisha, India. Forty-six adult patients
with SCA along with severe P. falciparum
malaria admitted in the Department of Medicine of this institute were
included in this study. The mean age of patients was 25.4±8.8 years
(range, 17 to 60 years) with 58.7% (27/46) being males. The hemoglobin
variants including HbF was estimated by Cation-Exchange high
performance liquid chromatography (CE-HPLC) using Variant II – β-thalassemia
short program (Bio-Rad laboratories, Hercules). The mean % HbF level
was found to be 18.2 ± 4.9 %; ranging from 6.0 to 29.0 %.
The severity of malaria was defined by WHO guideline in 2010.[5]
The severity due to the malarial infection was defined by the presence
of single or multiple complications. Cerebral malaria, severe malarial
anemia, jaundice, acute renal failure and/or hepatopathy were
considered as the major clinical symptoms of the patients. Among the
various clinical symptoms, the incidence of cerebral malaria was 37.0%
(17/46) followed by severe malarial anemia (21.7%, 10/46). Episodes of
vaso-occlusive crises were observed in 50.0% of cases. Death was
recorded in 9 patients including six females. The demographic and
clinical features of patients have been shown in Table 1.
There were multiple complications responsible for mortality in these
patients. The comparison of % HbF level in patients with a various
number of complications they had revealed that the mean % HbF levels
increased with the number of clinical complications in the patients.
The average increase in the % HbF level was 15.7±4.0, 18.0±4.0,
18.9±6.1 and 20.8±1.2 respectively in patients with single, two, three
and four complications. Further linear regression analysis between
total hemoglobin level and % HbF level in the patients elucidated an
inverse relationship (r, -0.356; p, 0.015), which indicates that
patients with higher % HbF level had lower total hemoglobin
level.
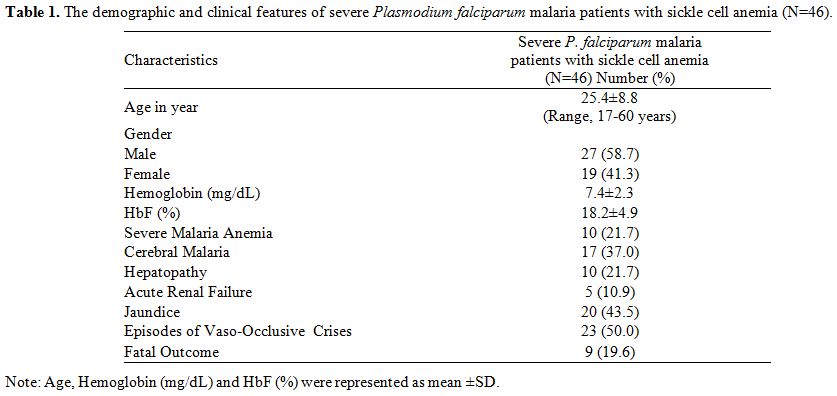 |
Table
1. The demographic and clinical features of severe Plasmodium falciparum malaria patients with sickle cell anemia (N=46). |
In
another comparison, we found that there was a trend in increasing % HbF
level in patients with severe malarial anemia compared to patients
without it. A similar tendency was observed in patients with cerebral
malaria. The average % HbF level also significantly increased averagely
in patients who died compared to patients who survived (p, 0.01).
The % HbF differences in the patients with severe malarial anemia,
cerebral malaria, and fatality, has been illustrated in Figure 1.
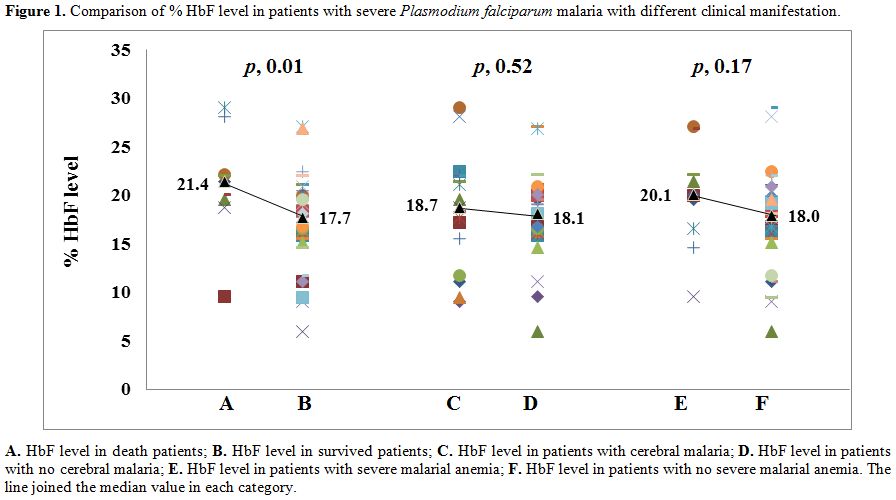 |
Figure 1. Comparison of % HbF level in
patients with severe Plasmodium falciparum malaria with different
clinical manifestation. |
Like HbS, alpha thalassemia has also been found to have a protective role against P. falciparum
malaria. However, this protection afforded by alpha thalassemia becomes
relatively sluggish when co-inherited with HbS. Because of a higher
prevalence of alpha thalassemia in the study area,[1]
we have attempted to compare the hematological and clinical parameters
in patients with heterozygous and homozygous alpha thalassemia
separately against patients with normal alpha globin genotype. There
were no statistically significant differences between the groups in
hematological (Supplementary Table 1)
as well as clinical parameters except for severe malarial anemia which
was higher in patients with homozygous alpha thalassemia (Supplementary Table 2).
Severe malarial anemia was associated with alpha thalassemia whereas
alpha thalassemia has no impact on mortality, so we have analyzed the
association of severe malarial anemia with mortality and was found
insignificant (OR, 0.2; 95%CI [0.038-0.98]; p, 0.06).
From the three factors above, which are associated with severity and mortality due to P. falciparum
malaria in patients with SCA, derived that HbF has a negative role in
protection against severe disease manifestation. It has been found that
HbF provides protection from P. falciparum malaria by diminishing the growth of the parasites inside the RBCs.[6] Instead of giving protection, the high level of HbF in our patients is associated with a major severity of P. falciparum infection. This might be due to the peripheral selection and not for its increased synthesis of HbF in patients with SCA.
Though,
HbF in SCA is found to be supportive in reducing episodes of
vaso-occlusive crises and requirements of blood transfusion,[7]
the protection afforded by HbS against severe malaria reduced with
increased % HbF level. This study agrees with the hypothesis of a
negative epistatic interaction between HbS and HbF in reducing
protection against severe malaria by Mmbando et al.,[4]
In this situation, use of hydroxyurea (a drug which usually increases
HbF level) in patients with SCA in malaria endemic regions is
debatable. In general, hydroxyurea must be started in severe patients
with SCA because (1) increasing HbF level following hydroxyurea therapy
is the principal but not the sole determinant of clinical responses in
these patients; (2) some patients with minimal or no increased in HbF
level following hydroxyurea therapy also showed significant clinical
responses.[8] In the present study, 26 patients were
on hydroxyurea therapy, from which 15.4% (4/26) of patients died
compared to 25.0% (5/20) of death in patients without hydroxyurea
therapy. A large cohort study in a malaria endemic region is essential
to give conclusive results on the association of HbF and use of
hydroxyurea in patients with SCA.
Acknowledgment
This
study was supported by research funding from Indian Council of Medical
Research (ICMR), New Delhi; Department of Science and Technology (DST),
New Delhi; and National Health Mission, Govt. of Odisha, India.
References
- Purohit P, Dehury S, Patel S, Patel DK. Prevalence
of Deletional Alpha Thalassemia and Sickle Gene in a Tribal Dominated
Malaria Endemic Area of Eastern India. ISRN Hematology. 2014; 2014:
e745245. http://dx.doi.org/10.1155/2014/745245 PMid: 24808962 PMCid: PMC3967634

- Mmbando
BP, Mgaya J, Cox SE, et al., Negative Epistasis between sickle and
foetal haemoglobin suggests a reduction in protection against malaria.
PLoS ONE. 2015; 10(5): e0125929. http://dx.doi.org/10.1371/journal.pone.0125929 PMid:25965586 PMCid:PMC4428884
- McAuley
CF, Webb C, Makani J, et al., High mortality from Plasmodium falciparum
malaria in children living with sickle cell anemia on the coast of
Kenya. Blood. 2010;116:1663-1668. http://dx.doi.org/10.1182/blood-2010-01-265249 PMid:20530796 PMCid:PMC3073423
- Makani
J, Komba AN, Cox SE, et al., Malaria in patients with sickle cell
anemia: burden, risk factors, and outcome at the outpatient clinic and
during hospitalization. Blood. 2010; 115(2): 215-220. http://dx.doi.org/10.1182/blood-2009-07-233528 PMid:19901265 PMCid:PMC2843825
- World Health Organization: Guidelines for the Treatment of Malaria, 2nd ed. Geneva, World Health Organization, 2010 http://www.who.int/malaria/publications/atoz/9789241547925/en/
- Pasvol
G, Weatherall DJ, Wilson RJ. Effect of foetal haemoglobin on
susceptibility of red cells to Plasmodium falciparum. Nature. 1977; 270
(5633):171-3. http://dx.doi.org/10.1038/270171a0 PMid:337159
- Mashon
RS, Dash PM, Khalko J, et al., Higher fetal hemoglobin concentration in
patients with sickle cell disease in eastern India reduces frequency of
painful crisis. European Journal of Hematology. 2009; 83(4):383-384. http://dx.doi.org/10.1111/j.1600-0609.2009.01290.x PMid:19508686
- Steinberg
MH, Lu Z-H, Barton FB, et al., Fetal hemoglobin in sickle cell anemia:
Determinants of response to hydroxyurea. Blood. 1997; 89:1078-1088.
PMid:9028341
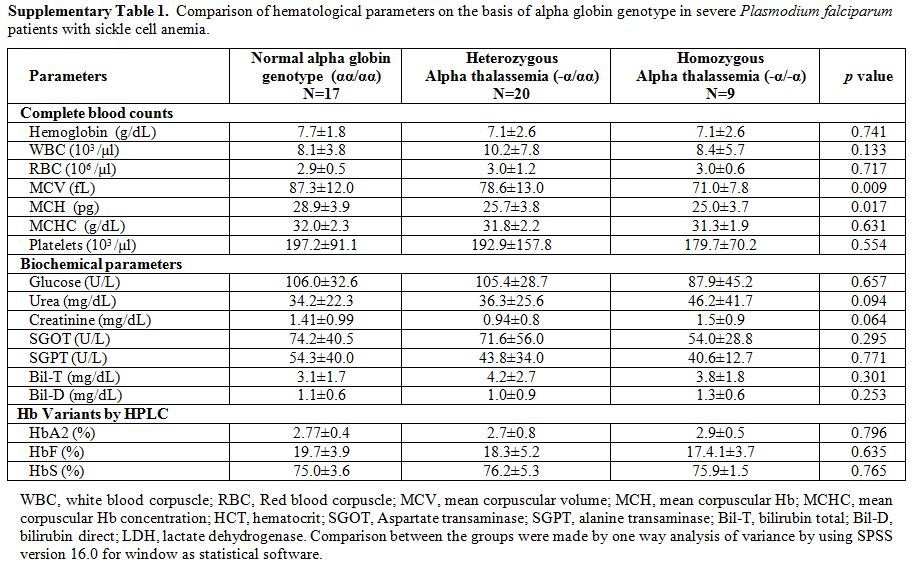 |
Supplementary Table 1. Comparison of
hematological parameters on the basis of alpha globin genotype in
severe Plasmodium falciparum patients with sickle cell anemia. |
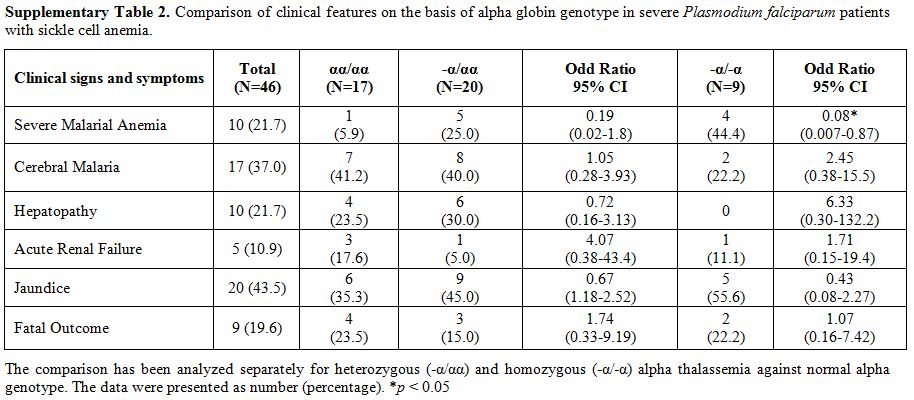 |
Supplementary Table 2. Comparison of
clinical features on the basis of alpha globin genotype in severe
Plasmodium falciparum patients with sickle cell anemia. |
[TOP]