Received: May 7, 2018
Accepted: June 24, 2018
Mediterr J Hematol Infect Dis 2018, 10(1): e2018046 DOI 10.4084/MJHID.2018.046
This article is available on PDF format at:

May Basood, Howard S. Oster and Moshe Mittelman
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract The
myelodysplastic syndromes (MDS) are a group of clonal bone marrow (BM)
stem cell disorders, characterized by ineffective hematopoiesis,
peripheral cytopenias, and hematologic cellular dysfunction, as well as
potential transformation to acute leukemia. |
Introduction
Thrombopoiesis and Thrombomimetic Agents
Romiplostim
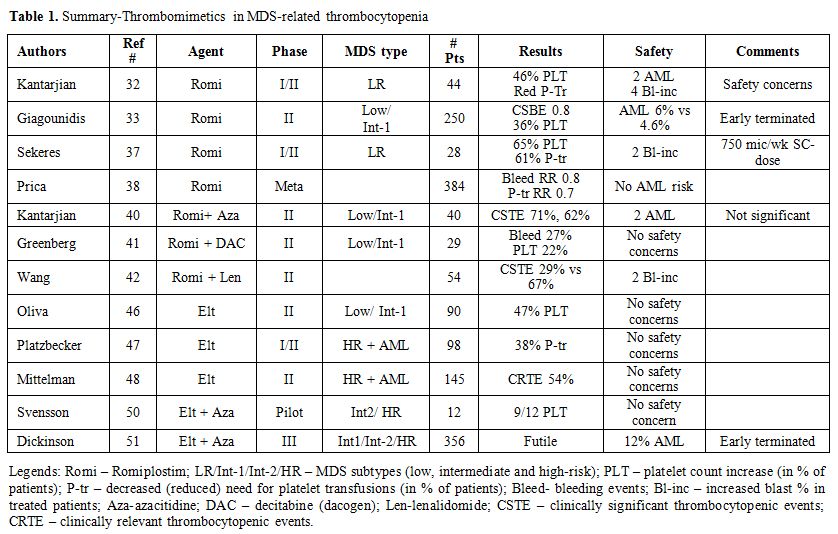 |
Table 1. Summary-Thrombomimetics in MDS-related thrombocytopenia |
Eltrombopag
Summary and Conclusions
References

[TOP]