Nahla A. Hamed1, Nabil A. Elhalawani1, Heba S. Kassem2, Mona W. Ayad3 and Enas A. Dammag4.
1 Professor of Hematology, Internal Medicine, Faculty of Medicine, Alexandria University, Egypt.
2 Professor of Pathology, Medical Genetics Center, Faculty of Medicine, Alexandria University, Egypt.
3 Professor of Clinical Pathology, Faculty of Medicine, Alexandria University, Egypt.
4 Hematology, Internal Medicine, Hematology Department, Faculty of Medicine, Taiz University, Yemen.
Corresponding
author: Dr. Enas A. Dammag. Hematology, Internal Medicine, Hematology
Department, Faculty of Medicine, Taiz University, Yemen. E-mail:
enas.alid@yahoo.com
Published: January 1, 2020
Received: June 26, 2019
Accepted: November 13, 2019
Mediterr J Hematol Infect Dis 2020, 12(1): e2020004 DOI
10.4084/MJHID.2020.004
This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by-nc/4.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Background:
Chronic myeloid leukemia (CML) is a myeloproliferative neoplasm where
pathogenesis is based on the oncoprotein termed BCR‐ABL1.[1] TET2
initiates DNA demethylation and is frequently mutated in hematological
malignancies, including CML. The relation between TET2 acquisition and
CML transformation and/or imatinib resistance is needed to be
investigated.[2]
Aim: To
evaluate Ten Eleven Translocation 2 gene (TET2) single nucleotide
polymorphism (SNP) (rs2454206, rs34402524, rs61744960) in chronic
myeloid leukemia (CML) in relation to the disease prognostic criteria.
Materials & Method:
The study included 84 subjects; 54 CML in chronic phase and 30 healthy
subjects as control group matched for age and sex. Routine
investigations, including CBC, bone marrow aspiration, biochemical
investigations, and molecular study, were performed in CML patients to
identify the disease stage. DNA extraction and SNP assay for TET2 gene
polymorphism were done using (Thermo-Fisher predesigned SNP, USA) PCR
prism 7500.
Results: The
mean age was 45.98±15.7 yrs in CML patients and 39.3±6.587 yrs in the
control group (p>0.05). TET2 SNP rs 34402524 was either heterozygous
or homozygous in CML (48%, 46.2% respectively) but was mainly
homozygous among control (80%) group (p=0.012). TET2 SNP rs 2454206
wild type within CML was detected in 65.4% of patients and in controls
was 63.3% (p=0.046). TET2 SNP rs 61744960 showed a homozygous pattern
among all groups (CML and control) (p=0.528). TET2 SNP in CML cases did
not alter the prognostic criteria as no statistical significance was
noted (p>0.05) yet, it was significantly related to spleen size in
rs 34402524 where the homozygous group had larger spleen size and
higher BCR-ABL1 levels six months after starting TKIs (p<0.05).
Conclusions/Recommendation:
TET2 SNP is common among Egyptian chronic myeloid leukemia. TET2 SNP rs
3442524 was associated with larger spleen size and higher BCR-ABL1
levels after six months of starting TKIs suggesting disease progression.
|
Introduction
Chronic
myeloid leukemia (CML) is a myeloproliferative neoplasm. Its
pathogenesis is based on the oncoprotein BCR‐ABL1 that is the fusion of
the Abelson murine leukemia (ABL1) gene on chromosome 9 and the
breakpoint cluster region (BCR) gene on chromosome 22. This oncoprotein
is an active tyrosine kinase that promotes growth and replication.
Several signaling pathways downstream are involved, such as RAS, RAF,
JUN kinase, MYC, and STAT. The end product is leukemogenesis
created via a cytokine‐independent cell cycle and aberrant apoptotic
signals.[3]
The progression of CML into accelerated phase or
blastic phase is associated with the acquisition of genetic or
epigenetic abnormalities in particular somatic mutations in genes of
chromatin modification of DNA methylation in addition to BCR-ABL
rearrangement.[4]
TET-2 has pleiotropic roles during
hematopoiesis, including stem cells self-renewal, lineage commitment,
and terminal differentiation of monocytes.[5] The chromosome 4q24
region containing theTET-2 gene[6] TheTET-2 gene has 11 exons,[7] and
the resulting messenger RNA (mRNA) may form three different isoforms
due to alternative splicing.[8] TET 2 is part of the non-driver genetic
alterations that may influence myeloproliferative neoplasms development
and outcome in general.[9]
The Ten – Eleven Translocation TET
proteins TET-1,TET-2, TET-3 are α - ketoglutarate and Fe2+ dependent
enzymes capable of modifying DNA methylation status.[10] TET family
enzymes and 5- hmC are critical in epigenetic regulation during
development.[11] Homozygous and heterozygous mutations in TET-2 gene are
recurrent events in human hematopoietic malignancies. Most of these
mutations decreaseTET-2 enzymatic activity by truncating the protein or
affecting its catalytic activity.TET-2 deletion is sufficient to
initiate myeloid and lymphoid transformation, including CML.[12] The
role of TET2 polymorphism is not fully established according to the
prognostic and responsiveness to treatment in the context of myeloid
malignancies, mainly CML.
Aim of Work
The
aim of this study is to evaluate the incidence of the TET2 single
nucleotide polymorphism (SNP) (rs2454206, rs34402524, rs61744960) in
chronic myeloid leukemia and healthy controls in relation to the
disease’ prognostic-criteria.
Materials and Method
The
study included 84 subjects; 54 cases were diagnosed as CML, and 30
subjects as a control group matched for age and sex. Cases were
selected from Alexandria Main University Hospital Internal Medicine
Department (Hematology Unit) Egypt to determine the selected SNPs
genotype frequency. Written Informed consent was taken from every
patient and approval of the Ethical committee (IRB No. 00008699, FWA
No.00015712) was provided. Routine investigations, including CBC, bone
marrow aspiration, biochemical investigations, and molecular study,
were performed according to CML to identify the disease stage. A 3ml
blood collected via EDTA tubes from either peripheral blood or bone
marrow aspirate was done. DNA extraction was performed using Invitrogen
purelink genomic DNA minikit (Cat No. k1820-01, Lot No 1510617). The
SNP assay for TET2 gene polymorphism, performed with (Thermo-Fisher
predesigned SNP, USA) PCR prism 7500 device, included tree
polymorphisms that are c-25996719-10, rs 34402524, lot p161221-001 H06,
PN*40 (intron missense) c-11566753-20, rs 2454206, lot p161221-001 H08
PN *40 (intron missense) c-25746528, rs 61744960, lot p161221-001 H05
PN*40 (intron missense).
Patients were started on Imatinib 400mg
per oral daily after confirming the diagnosis and were followed up
monthly by CBC, liver and renal function tests as a routine for filling
up their prescriptions. At 3 and 6 months, BCR ABL1 IS% was done by
real time PCR to monitor response during which no dose adjustments were
required, and mild side effects were reported in the form of mild
musculoskeletal pain treated by paracetamol.
Statistical analysis.
The software of IBM SPSS 20 was used. Data were tested for normality
using the Kolmogorov-Smirnov test, Shapiro-Wilk test. Measurement data
were displayed in the form of minimum, maximum, mean ± SD. T-test was
used for comparing means in parametric data. Qualitative data were
displayed in percentages and tested by Pearson's Chi Square and Fisher
Exact Test according to the categories and cells estimation %. If the
distribution was nonparametric in distribution, measurement data were
displayed in the form of median value and range, and the nonparametric
test (Mann-Whitney U) was used for comparing median value. Spearman
bivariate correlation analysis was used for analyzing correlation.
P<0.05 indicated statistical significance.
Results
The
mean age was 45.98±15.7 yrs in CML patients and 39.3±6.587 yrs in the
control group (p>0.05). TET2 SNP rs 34402524 was either heterozygous
or homozygous in CML (48%, and 46.2% respectively) but was mainly
homozygous among the control (80%) group (p=0.012). TET2 SNP rs 2454206
wild type within CML was 65.4% and in control was 63.3% group (p=0.046)
(Table 1, Figure 1)
TET2 SNP rs 61744960 showed a homozygous pattern among all groups (CML
and control) (p=0.528). CML counts were not influenced by TET2
polymorphism, including Hb level, platelets count, WBC, basophil count,
and bone marrow blasts (P>0.05) (Table 2).TET2
SNP in CML cases did not alter the prognostic criteria as no
statistical significance was noted (p>0.05) except for TET2 SNP
rs3442524 homozygous group that was significantly related to huge
spleen size with homozygous group and higher BCR-ABL1 levels after six
months of starting TKIs (p<0.05) (Table 3).
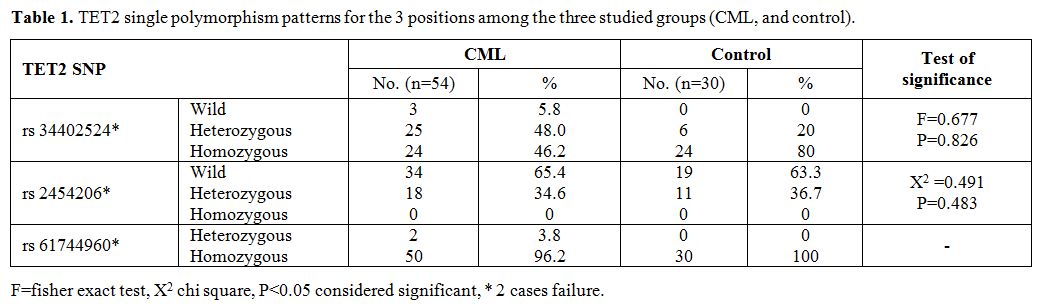 |
Table 1.
TET2 single polymorphism patterns for the 3 positions among the three studied groups (CML, and control). |
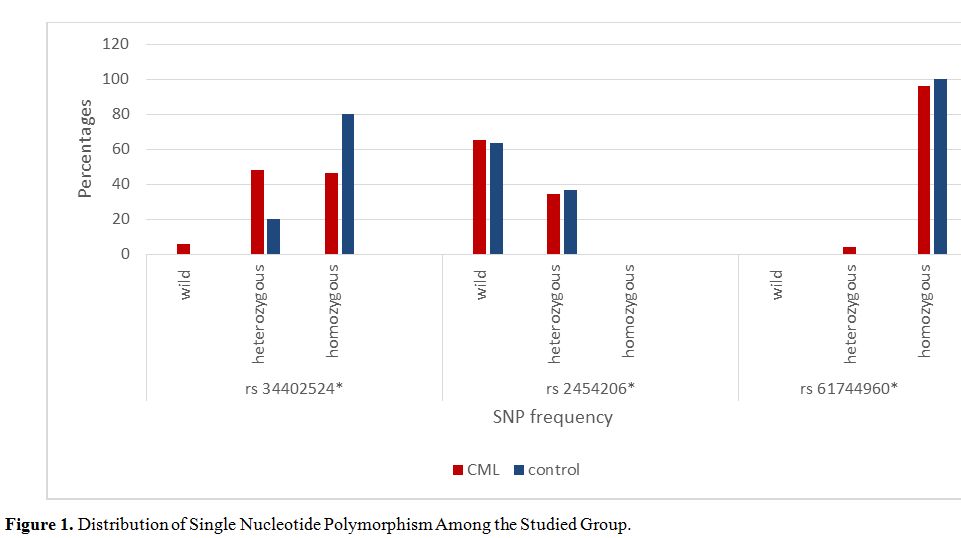 |
Figure 1. Distribution of Single Nucleotide Polymorphism Among the Studied Group. |
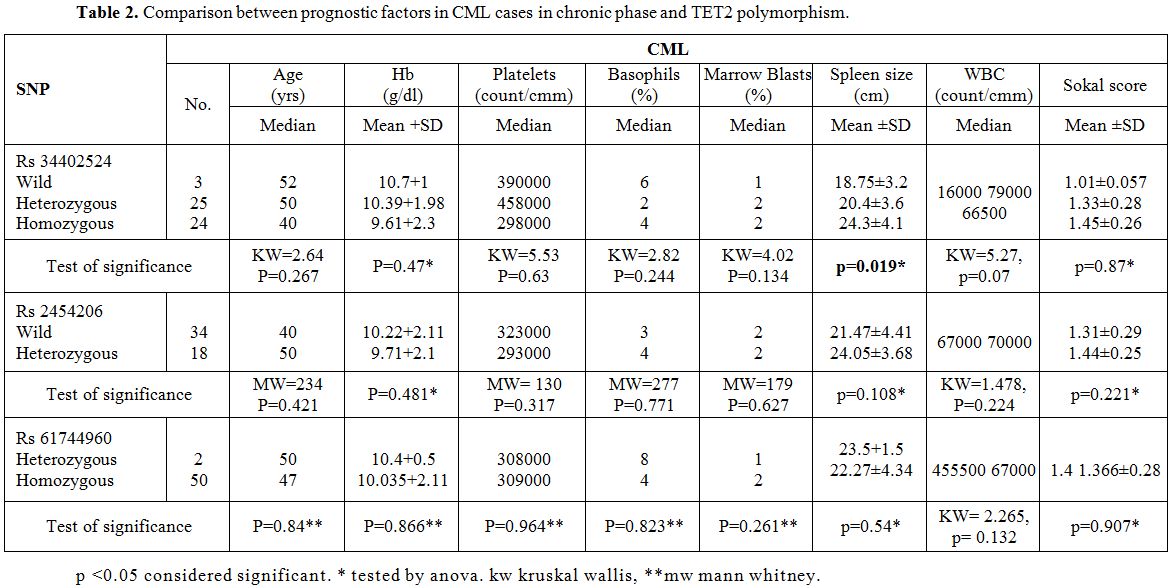 |
Table 2. Comparison between prognostic factors in CML cases in chronic phase and TET2 polymorphism. |
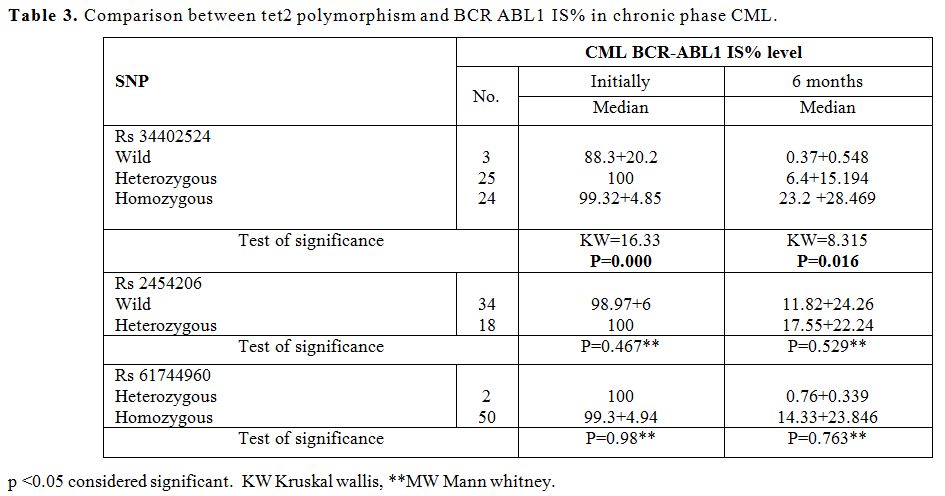 |
Table 3. Comparison between tet2 polymorphism and BCR ABL1 IS% in chronic phase CML. |
Discussion
TET2
regulates epigenetics modification of DNA via regulation of cytosine
methylation, and that is crucial for stem cells and progenitor cells'
self -renewal and leukemia prevention. TET2 mutations are common in
hematological diseases, including CML. TET2 polymorphism is influenced
by racial variation. Little was reported on the influence of TET2
polymorphism among myeloid neoplasms. Studies linked acute leukemia to
various TET2 polymorphism influencing the outcome, and this might
suggest a role of TET2 polymorphism and its mutations in transforming
CML from chronic phase to accelerated phase or blast crisis.
In
our study, TET2 SNP rs 34402524 among chronic phase CML was either
heterozygous 48% or homozygous 46% but was mainly homozygous among the
control group (80%) (p=0.012). As for TET2 SNP rs 2454206, wild type in
CML and control group were (62.5%, 63.3% respectively) (p=0.046). TET2
SNP rs 61744960 showed a homozygous pattern among all groups (CML 95.8%
and control 100%) (p=0.528).
The studied TET2 SNP might be
present as part of a germline phenotype influenced by racial
background, as noted within the control group. Variations of TET2 SNP
between the control group and CML may suggest that CML patients may
have lacked or lost these germline phenotypes during leukomogenesis.
The three profiles of TET2 and BCR-ABL emergence are possible: TET2
could proceed BCR-ABL in these cases all Ph positive and Ph negative
are TET2 mutant. A biclonal disease, in this case, all Ph positive
cells are TET2 wild type. BCR-ABL could occur before TET2 mutation
suggesting a late diagnosis of CML.[2]
Kutny et al., in 2015[13]
in a study involving 403 patients enrolled in Children’s Cancer Group
reported that the 10 SNPs with higher prevalence (4%–54%), only the
most prevalent SNP, rs2454206 (A>G, I1762V) was associated with
survival. OS was significantly higher for patients with minor allele
genotypes (TET2 AG/GG) than those with TET2 AA genotype (60±10% vs.
38±11% at 5 years, log-rank P=0.013 TET2, the genotype was influenced
by racial variations. TET2AA genotype
occurred in 79% of black vs. 39% of white patients (p<0.001).
However, both in black and withe people, the survival was higher in
TET2 AG/GG respect to TET AA genotype.
Li et al. from Taiwan in 2011[14]
reported that about 78.6% of patients were diagnosed with TET2 SNP
(single nucleotide polymorphism). All SNPs were heterozygous, and only
4 SNP were homozygous; all were in SNP rs2454206 (I1762V).[14]
In
our study, as for chronic phase CML, TET2 SNP rs 34402524 homozygous
group was significantly related to larger spleen size and BCR-ABL1 IS%
levels at initial diagnosis and after six months on follow up after
starting TKIs. This suggests that it may play a role in disease
progression within Egyptian population (p<0.05). The other TET2
polymorphisms were common too, yet they did not alter the prognostic
criteria for CML patients regarding the Sokal score, WBC count, and
spleen size (p>0.05).
The present paper is the first to
relate TET2 polymorphism to prognostic parameters, and further studies,
within the Egyptian population.
Conclusions and Recommendations
TET2
SNP is a common finding among Egyptian chronic myeloid leukemia
patients. TET2 SNP rs 34402524 was associated with huge spleen size and
higher BCR-ABL1 levels after six months of starting TKIs denoting the
possibility of its relation to disease progression.
Ethical standards
All
procedures in this research was subjected to the ethical regulation of
ethical committee and a Written Informed consent was taken from every
patient and approval of the Ethical committee of the Faculty Of
Medicine – Alexandria University according to ICH GCP guidelines and
applicable local and institutional regulations and guidelines governing
EC operation (IRB No. 00008699, FWA No.00015712) full-filling the 1964
Helsinki declaration.
References
- Keramatinia A, Ahadi A, Akbari ME, Mohseny M,
Jarahi AM, Mehrvar N, et al. Genomic Profiling of Chronic Myelogenous
Leukemia: Basic and Clinical Approach. Journal of Cancer Prevention
2017;22(2):74-81. https://doi.org/10.15430/JCP.2017.22.2.74 PMid:28698860 PMCid:PMC5503218
- Roche-Lestienne
C, Marceau A, Labis E, Nibourel O, Coiteux V, Guilhot J, et al.
Mutation analysis of TET2, IDH1, IDH2 and ASXL1 in chronic myeloid
leukemia. Leukemia 2011;25(10):1661-4. https://doi.org/10.1038/leu.2011.139 PMid:21637286
- Jabbour
E, Kantarjian H. Chronic myeloid leukemia: 2018 update on diagnosis,
therapy and monitoring. American Journal of Hematology
2018;93(3):442-59. https://doi.org/10.1002/ajh.25011 PMid:29411417
- Kim
T, Tyndel MS, Kim HJ, Ahn J-S, Choi SH, Park HJ, et al. Spectrum of
somatic mutation dynamics in chronic myeloid leukemia following
tyrosine kinase inhibitor therapy. Blood 2017;129(1):38. https://doi.org/10.1182/blood-2016-04-708560 PMid:27733357
- E
Solary, O A Bernard, A Tefferi, F Fuks, Vainchenker W. Ten-Eleven
Translocation-2 (TET2) gene in hematopoiesis and hematopoietic
diseases. Leukemia 2013:1-36. https://doi.org/10.1038/leu.2013.337 PMid:24220273
- Ko M, Rao A. TET2: epigenetic safeguard for HSC. Blood 2011;118(17):4501-3. https://doi.org/10.1182/blood-2011-08-373357 PMid:22033942
- Albano
F, Anelli L, Zagaria A, Coccaro N, Minervini A, Rossi AR, et al.
Decreased TET2 gene expression during chronic myeloid leukemia
progression. Leukemia Research 2011;35(11):e220-e2. https://doi.org/10.1016/j.leukres.2011.07.013 PMid:21794915
- Mohr
F, Döhner K, Buske C, Rawat VPS. TET Genes: new players in DNA
demethylation and important determinants for stemness. Experimental
Hematology 2011;39(3):272-81. https://doi.org/10.1016/j.exphem.2010.12.004 PMid:21168469
- Shammo
JM, Stein BL. Mutations in MPNs: prognostic implications, window to
biology, and impact on treatment decisions. Hematology American Society
of Hematology Education Program 2016;2016(1):552-60. https://doi.org/10.1182/asheducation-2016.1.552 PMid:27913528 PMCid:PMC6142495
- Ko
M, Bandukwala HS, An J, Lamperti ED, Thompson EC, Hastie R, et al.
Ten-Eleven-Translocation 2 (TET2) negatively regulates homeostasis and
differentiation of hematopoietic stem cells in mice. Proceedings of the
National Academy of Sciences 2011;108(35):14566-71. https://doi.org/10.1073/pnas.1112317108 PMid:21873190 PMCid:PMC3167529
- Tan L, Shi YG. Tet family proteins and 5-hydroxymethylcytosine in development and disease. Development 2012;139:1895-902. https://doi.org/10.1242/dev.070771 PMid:22569552 PMCid:PMC3347683
- Solary
E, Bernard OA, Tefferi A, Fuks F, Vainchenker W. The Ten-Eleven
Translocation-2 (TET2) gene in hematopoiesis and hematopoietic
diseases. Leukemia 2014;28(3):485-96. https://doi.org/10.1038/leu.2013.337 PMid:24220273
- Kutny
MA, Alonzo TA, Gamazon ER, Gerbing RB, Geraghty D, Lange B, et al.
Ethnic variation of TET2 SNP rs2454206 and association with clinical
outcome in childhood AML: a report from the Children/'s Oncology Group.
Leukemia 2015;29(12):2424-6. https://doi.org/10.1038/leu.2015.171 PMid:26126966 PMCid:PMC4675677
- Li
M-J, Yang Y-L, Jou S-T, Lu M-Y, Chang H-H, Lin K-H, et al. Prevalence
& Prognosis Value of TET2 Gene Polymorphisms in Childhood Acute
Myeloid Leukemia in Taiwan. Blood 2011;118(21):1551. https://doi.org/10.1182/blood.V118.21.1551.1551
[TOP]