The introduction of effective antiretroviral (ARV) regimens have produced a profound impact on the natural history of HIV infection, leading to a dramatic decrease in its mortality and a considerable increase in the life expectancy of Persons Living with HIV (PLWH). Nevertheless, these patients still appear to be at higher risk of a number of co-morbidities, such as cardiovascular disease (CVD) than the general population.[1,2] Measurement of carotid IMT with color-Doppler ultrasonography is a non-invasive, sensitive and highly reproducible technique aimed at the assessment of vascular anatomy and function, and for identifying and quantifying atherosclerotic lesions, even at a very early stage. It is a well-validated research tool and is widely used in clinical practice.[3]
This technique allows measurement of a variety of parameters including intima-media thickness (IMT), arterial diameter, the presence of plaque, blood flow, and velocity measurements.
Carotid IMT and presence of plaque have been shown to predict cardiovascular events in large studies.[4,5] Also, in low-risk subjects, initial screening by IMT and plaque assessment is likely to provide useful information for the detection of subclinical atherosclerosis.[6] Furthermore, common carotid blood flow (CBF) velocity was independently associated with future cardiovascular disease (CVD) using color duplex ultrasound and Doppler spectral analysis.[7] In clinical practice, evaluation of the carotid artery by ultrasonography is a handy, simple, and safe method to detect and prevent CVD indirectly. In preventive medicine, IMT measurement is especially important for subjects with intermediate CV risk, i.e., for subjects with a 10 year risk of CV disease between 6% and 20%.[8]
PREVALEAT (PREmature VAscular LEsions and Antiretroviral Therapy) is an ongoing multicenter, longitudinal cohort study involving several Italian centers since 1998, aimed to the evaluation of cardiovascular (CV) risk in HIV-infected patients using color-Doppler ultrasonography.[9-12] The cohort produced, in the years, several studies in this field. Considering that this technique is, at present, widely diffused among the Italian HIV outpatient facilities, our present aim is to generate a National Register of color-Doppler ultrasonography (Archi-Prevaleat) to better evaluate the characteristics of vascular lesions in PLWH, on a large number of data. This ongoing project involves, at present, nine Italian Centers in which the ultrasonographic examination is performed by specifically trained physicians during a Continuing Medical Education stage previously organized by the coordinating Center (Bari). Periodical follow-up meetings were held using images and filmed reports aimed at the comparison and standardization of the technique. The Register is based on an on-line platform (http://www.archiprevaleat.com/) aimed at collecting data regarding patients routinely submitted to the examination for the first time and at all the subsequent follow-up examinations.
Intima Media Thickness (IMT) of common and internal carotid for both left and right sides is registered. A minimum of three measurements are requested: on the common carotid artery: 1 cm before the carotid bifurcation and at the carotid bifurcation; on the internal carotid: 1 cm after the carotid bifurcation and 2 cm after the carotid bifurcation. An IMT of >1 mm is considered pathological. Atherosclerotic plaques, if present, are described. All relevant images are photographed and properly archived.
The register will generate retrospective, non-interventional observational studies, planned by the panel of specialists involved in the project during periodical meetings.
The following parameters will be evaluated at the first visit and at the subsequent control visits, every 6 to 12 months:
1) IMT of common and internal carotid for both left and right sides: ultrasonography of the epi-aortic vessels is performed using a power colour-Doppler instrument with 7.5 MHz probes. We evaluate the characteristics of the intima, together with the pulsation index, the resistance index, the minimal speed, the peak speed and mean speed. A minimum of three measurements are requested: on the common carotid artery: 1 cm before the carotid bifurcation and at the carotid bifurcation; on the internal carotid: 1 cm after the carotid bifurcation and 2 cm after the carotid bifurcation. An intima media thickness (IMT) of >1 mm is considered to be pathological. Atherosclerotic plaques, if present, are described. All images are photographed and properly archived.
2) Data regarding independent risk factors for CVD (family history, smoke, active drug addiction, alcohol consumption) are collected at baseline and re-evaluated every 12 months.
3) HIV viral load, CD4+ cell counts, total serum cholesterol, LDLc, HDLc, glycemia, triglycerides, body mass index (BMI) are recorded at every control.
Moreover, during the study, periodical meetings will be held using filmed reports and/or images in order to obtain comparison and standardization of the techniques.
We have enrolled until now 159 patients who performed color-Doppler ultrasonography in the participating Centers. Demographic data of the enrolled patients, metabolic data, and result of the color-Doppler ultrasonographic investigation are summarized in Table 1.
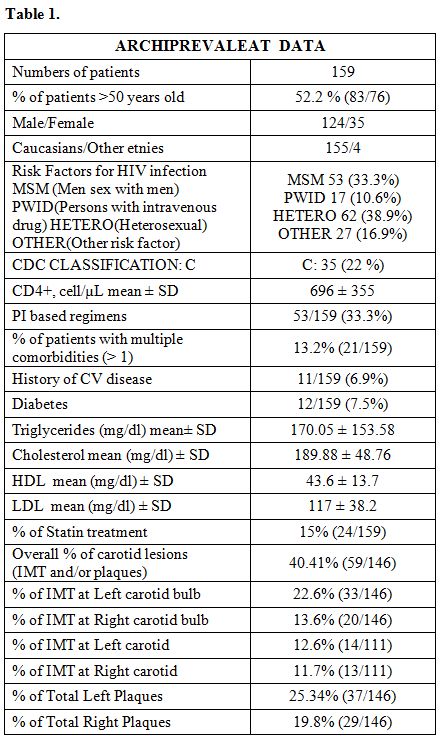 |
Table 1 |
In our cohort, 52% of patients were over 50 years old; females were 28.2%; 13% showed multiple comorbidities, and 6,9% had a history of CV disease. 22% of the patients were in group C of the Center for Diseases Control (CDC) – Atlanta 1993; 33.3% of the patients received an antiretroviral treatment based on protease inhibitors (PIs).
The overall percentage of patients with carotid lesions (IMT and/or plaques) was 40.41% (Figure 1). In detail, the prevalence of IMT has been 22.6% at the left carotid bulb,13.6% at the right carotid bulb, 12.6 % at left internal carotid, and 11.7% at the right internal carotid. We have observed a total of 25.34 % of plaques at the left carotid and a total of 19.86% of plaques at the right carotid. A higher prevalence of plaques has been identified in the bulb section on both sides. (Table 1 and Figure 1).
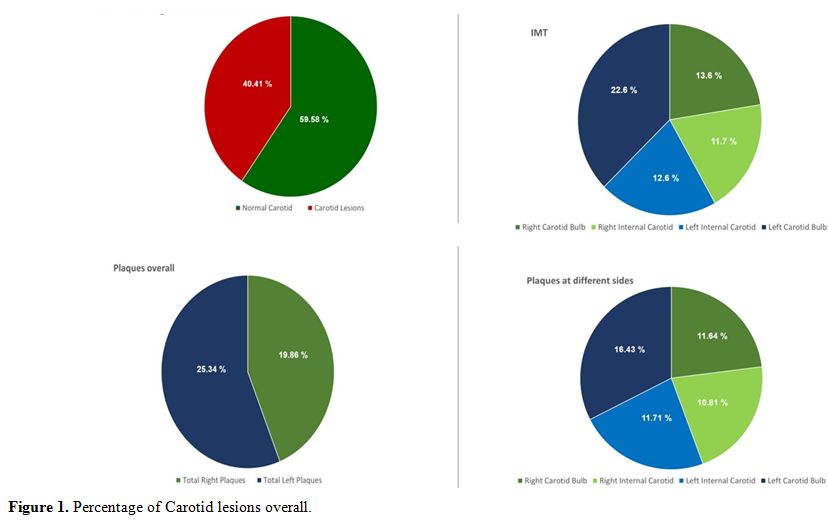 |
Figure 1. Percentage of Carotid lesions overall. |
Analyzing different factors related to IMT, it appeared a high incidence of carotid lesions in patients with high levels of Triglicerides (36%), high levels of Cholesterol (34%). About the low CD4 count, only 5.6% of enrolled patients had < 200 CD4 with IMT in 33% of them. In every case, patients historically classified as CDC C showed a high incidence of IMT (48.5%). About treatment, patients with a PI-based regimen, generally associated with high lipids and higher cardiovascular risk, showed IMT in 28% of cases, higher than patients treated with other antiretroviral regimens (16%). However, in this case, we have a trend of association between PI-based regimens and IMT but without statistical significance (p 0.12) (Figure 2).
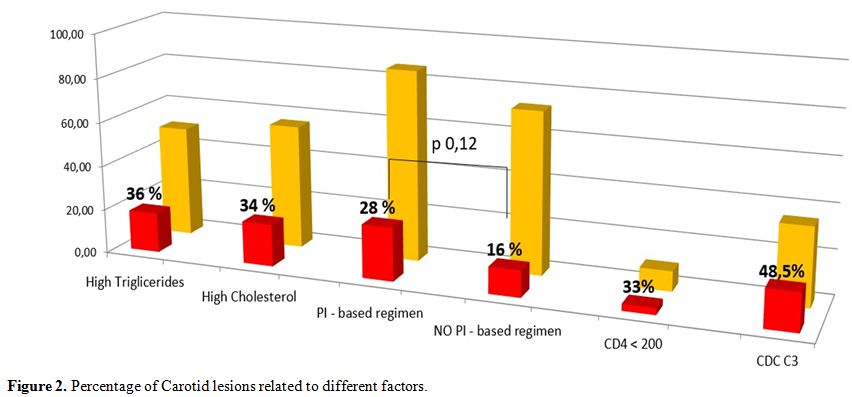 |
Figure 2. Percentage of Carotid lesions related to different factors. |
As seen previously, HIV-infected individuals appear to be at higher risk of CVD than the general population. In HIV patients, chronic inflammatory processes are activated, and atherosclerosis is accelerated. Consequently, cardiovascular disease is one of the most common non-AIDS events with overall increased morbidity and mortality. Although the mechanisms involved remain elusive, endothelial activation due to the chronic inflammation seems to be the keystone of this phenomenon; proinflammatory citokines,[12] pro-angiogenic hematopoietic and endothelial progenitor cells,[13] circulating CD40 ligand, and Dickkopf-1[14] could be involved.
In this setting, measurement of carotid IMT with color-Doppler ultrasonography plays a pivotal role in identifying and quantifying atherosclerotic lesions, even at a very early stage. A Register of echoic images deriving from all the National territory could represent an important source of data able to produce a potentially continuous flux of information.
In our preliminary data IMT appears, as expected, associated above all with higher lipids levels, with CDC’ C stage, and with the adoption of PI-based regimens.
Our Register shows a considerably high percentage of patients with IMT and strong evidence of plaques. However, it is noteworthy that the majority of the patients are over 50 years old; for the most part, they are males, with an advanced stage of HIV disease, treated with PIs-based antiretroviral regimens, and so considered at higher cardiovascular risk.[12,15] These data highlight the fact that the clinicians tend to submit to this investigation their patients at higher risk of CV events; this, at present, hampers a reliable statistical comparison between groups, and represent the major limitation of our study. On the other hand, this behavioral datum is crucial and should be modified with specific educational interventions. As we stated before, in fact, Archi-Prevaleat Register is ongoing and includes periodical follow-up meetings of the involved physicians. For this reason, we feel that it could represent a valuable way to improve the awareness of the Italian specialists regarding this diagnostic tool and to ameliorate its utilization. Considering that this diagnostic tool is particularly useful in patients at intermediate risk, this will prompt to extend the investigation to all patients, to proactively prevent CVD, that, in association to aging, inflammation and dyslipidemia, will have a negative impact on good prognosis conquered by the advent of safer antiretroviral drugs.