Ming Tong1,2,3, Ying Xiong4, Chen Zhu5, Hong Xu4, Qing Zheng6, Changping Hu7, Yu Jiang3, Lianhong Zou3, Xiaolin Xiao4, Fang Chen3 and Yimin Zhu2,3*.
1 Department
of Infectious Diseases, The First-affiliated Hospital of Hunan Normal
University (Hunan Provincial People's Hospital), Changsha, 410005,
Hunan, China.
2 School of Life Sciences, Hunan Normal University, Changsha, Hunan, China.
3
Institute of Emergency Medicine, Hunan Provincial Key Laboratory of
Emergency and Critical Care Metabonomics, The First-affiliated Hospital
of Hunan Normal University (Hunan Provincial People's Hospital),
Changsha, 410005, Hunan, China.
4 The Fourth People's Hospital of Yiyang, Yiyang, 413000, Hunan, China.
5 Department of Pediatrics, Yiyang Central Hospital, Yiyang, Hunan 413099, P.R. China.
6
Department of Geriatrics, The First-affiliated Hospital of Hunan Normal
University (Hunan Provincial People's Hospital), Changsha, 410005,
Hunan, China.
7 Department of Pharmacology, Xiangya School of Pharmaceutical Sciences, Central South University, Changsha 410078, Hunan, China.
Correspondence to: Yimin
Zhu. Institute of Emergency Medicine, Hunan Provincial Key Laboratory
of Emergency and Critical Care Metabonomics, The First-affiliated
Hospital of Hunan Normal University (Hunan Provincial People's
Hospital), Changsha, 410005, Hunan, China. E-mail:
zhuyimincs@outlook.com
Published: January 1, 2021
Received: September 23, 2020
Accepted: December 23, 2020
Mediterr J Hematol Infect Dis 2021, 13(1): e2021015 DOI
10.4084/MJHID.2021.015
This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by-nc/4.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Background:
Coronavirus disease 2019 (COVID-19) is highly contagious and deadly and
is associated with coagulopathy. Pentraxin-3(PTX3) participates in
innate resistance to infections and plays a role in thrombogenesis.
Purpose: The present study aimed to investigate the role of PTX3 in coagulopathy in patients with COVID-19.
Methods:
A retrospective study, including thirty-nine COVID-19 patients,
enrolled in Hunan, China, were performed. The patients were classified
into the D-dimer_L (D-dimer<1mg/L) and D-dimer_H (D-dimer≥1mg/L) groups
basing on the plasma D-dimer levels on admission. Serum PTX3 levels
were detected by enzyme-linked immunosorbent assays and compared
between those two groups, then receiver operating characteristic (ROC)
curve analysis, correlation analysis, and linear regression models were
performed to analyze the association between PTX3 and D-dimer.
Results: Our results showed that serum PTX3 levels (median values, 10.21 vs. 3.36, P<0.001), computerized chest tomography (C.T.) scores (median values, 10.0 vs. 9.0, P<0.05), and length of stay (LOS) (mean values, 16.0 vs. 10.7, P=0.001)
in the D-dimer_H group were significantly higher than that in D-dimer_L
group. ROC curve analysis revealed that the AUC of white blood
corpuscle counts, C-reaction protein, erythrocyte sedimentation rate,
and PTX3 for COVID-19 were 0.685, 0.863, 0.846, and 0.985,
respectively. Correlation analysis showed that there was a positive
relationship between PTX3 and D-dimer (r=0.721, P<0.001), chest CT imaging score (r=0.418, P=0.008), and LOS (r=0.486, P=0.002). Multiple linear regression analysis showed that the coefficient of determination was 0.657 (P < 0.001).
Conclusion:
Serum level of PTX3 was positively correlated with disease severity and
coagulopathy. Detection of serum PTX3 level could help identify severer
patients on admission
|
Introduction
In
December 2019, a cluster of severe pneumonia cases of unknown cause,
lately named Coronavirus disease 2019 (COVID-19), was reported in
Wuhan, China. A novel strain of coronavirus, severe acute respiratory
syndrome coronavirus 2 (SARS-CoV-2), was identified as the pathogen.[1]
COVID-19 can be asymptomatic or mild to severe symptomatic. As of
September 1, 2020, more than 25 million cases of COVID-19 have been
reported worldwide, with over 854 000 deaths, and the number is
overgrowing.[2]
Pentraxin-3 (PTX3) is a pentraxin superfamily member and is involved in acute and chronic inflammation and innate immunity.[3] The level of PTX3 fluctuates with the intensity of the immune-inflammatory response.[4]
PTX3 is also involved in endothelial dysfunction through various
mechanisms and is correlated with acute pulmonary embolism-related
deaths,[5] while endothelial dysfunction has been reported in severe COVID-19 and plays a vital role in coagulopathy.[6]
As an indirect marker of coagulation activation, the D-dimer level
greater than 1μg/mL (i.e. 1mg/L) on admission has been correlated with
an increased likelihood of in-hospital death in COVID-19 patients.[7]
The present study aimed to detect the serum level of PTX3 in different
groups according to the serum level of D-dimer and to analyze the
correlation of serum PTX3 levels with disease severity and coagulopathy.
Materials and Methods
A
retrospective study was conducted. From February 1 to March 10, 2020,
thirty-nine adult patients (age ≥18 years) tested positive with
SARS-CoV2 of throat-swab samples were admitted into the Infectious
Disease Ward in the Fourth People's Hospital of Yiyang in Hunan, China,
and they were all recruited into the study. The clinical
characteristics and laboratory findings of COVID-19 patients were
extracted from the medical records. Upon admission, the patients
underwent blood routine tests, biochemical and immunological routine
tests, quantifications of plasma C-reaction protein(CRP), erythrocyte
sedimentation rate(ESR) and D-dimer, and computerized chest
tomography(C.T.) scanning to assess the severity of COVID-19.
Diagnostic criteria for COVID-19 severity were based on the guidelines
of the National Health Commission of China.[8] The
patients were treated with inhaled interferon α-2b and oral
lopinavir-ritonavir as antiviral therapies and supportive treatments.
In our setting, no patients died during the observation period.
The
patients were discharged at the following conditions: the absence of
fever for at least three days; significant improvement in both lungs on
chest C.T. scanning; clinical remission of respiratory symptoms;
repeated negative in RT-PCR test of throat-swab samples at least
24-hours interval.
The study was approved by the ethics committee
of the indicated hospital by the Code of Ethics of the World Medical
Association Declaration of Helsinki. Written informed consent was
waived due to the nature of our retrospective study.
Blood sample collection.
PTX3 detections were routinely performed for the patients who had been
suspected of systemic infection in our hospital. In the cohort, vein
blood samples for PTX3 detection were collected at admission in a
fasting state, 6 a.m. the next morning after admission, and immediately
centrifuged at 1500×g and stored at −80°C until thawed once and
analyzed.
Chest computerized tomography.
The chest C.T. image analysis and grading were performed by two
radiologists with extensive thoracic radiology experience. The final
scores and grading were determined using a scoring system described in
the previous study;[9] the details are shown in Table 1.
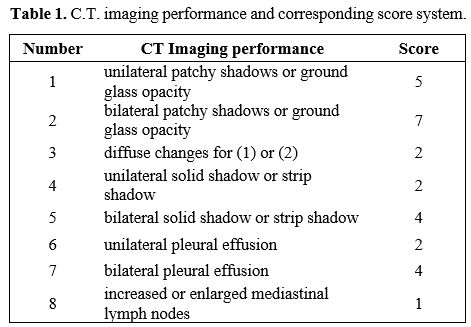 |
Table
1. C.T. imaging performance and corresponding score system.
|
Enzyme-linked immunosorbent assay (ELISA).
Strictly according to the manufacturer's instructions, quantitative
determination of the serum PTX3 level of one batch was performed weekly
using commercially available ELISA kits.
Statistical Analysis.
Categorical variables were reported as the counts and percentages, and
significance was detected by the chi-square test. The continuous
variables were described using mean and standard deviation if they were
normally distributed, or median and interquartile range (IQR) value if
they were not normally distributed. Continuous variables were compared
using independent group t-tests when they were normally distributed;
otherwise, the Mann-Whitney U-test was used. Correlation analysis was
performed by Pearson's correlation coefficient. Statistical analysis
was performed by SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). A
two-sided P-value<0.05 was considered statistically significant.
Results
Patient Characteristics.
According to the plasma D-dimer level on admission, the patients were
divided into the D-dimer_L group (<1mg/L) and the D-dimer_H group
(≥1mg/L). 48.7% (19 cases) were male, and there was no difference in
sex ratio between the D-dimer_L group and the D-dimer_H group. The
patients' average age was 49.0 years old, and the median age was 49.0
and 54.0 years old in D-dimer_L and D-dimer_H groups, respectively (P=0.03).
There were no significant differences in smoking, cardiovascular
disease, diabetes between both groups, while significant differences in
length of stay were observed (mean values, 10.7 vs. 16.0, P=0.001, Table 2).
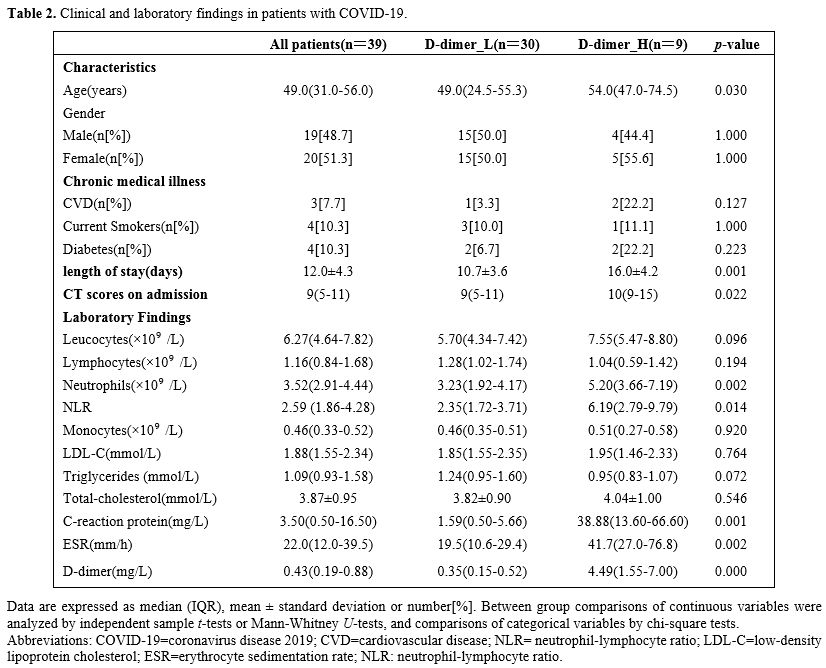 |
Table 2. Clinical and laboratory findings in patients with COVID-19.
|
For
laboratory findings, there were no significant differences in white
blood corpuscle (WBC) counts, lymphocyte counts, monocyte counts,
plasma levels of low-density lipoprotein-cholesterol (LDL-C),
triglycerides, and total cholesterol between both groups. In contrast,
significant differences in neutrophil counts (P=0.002), neutrophil-lymphocyte ratio(NLR) (P=0.014), plasma levels of CRP, and ESR (P<0.01) were observed. D-dimer's median values in D-dimer_L and D-dimer_H groups were 0.35 vs. 4.49mg/L (P<0.001, Table 2).
On
admission, abnormalities in chest C.T. images were observed for all
patients. The representative chest C.T. findings were bilateral
ground-glass opacity and sub-segmental areas of consolidation. The CT
imaging score was higher in the D-dimer_H group than the D-dimer_L
group (median values, 10.0 vs. 9.0, P=0.022; Table 2).
The
serum level of PTX3 in the D-dimer_H group was significantly higher
than that in the D-dimer_L group (median values, 10.21 vs. 3.36; P<0.001; Figure 1). Correlation analysis showed that there was a positive relationship between PTX3 and D-dimer (r=0.721, P<0.001), chest CT imaging score (r=0.418, P=0.008), and LOS (r=0.486, P=0.002) (Figure 2).
ROC curve analysis revealed that the area under the curve (AUC) of WBC
was 0.685 (95% confidence interval (CI) 0.517 - 0.824, P=0.010), and the optimum cutoff was 8.57x109/L (sensitivity 44.4%, specificity 90.0%). The AUC of CRP was 0.863 (95%CI 0.715 - 0.952, P=0.001),
and the optimum cutoff was 9.05 (sensitivity 88.9%, specificity 86.7%).
The AUC of ESR was 0.846 (95%CI 0.695 - 0.942, P=0.002),
and the optimum cutoff was 20.17 (sensitivity 100%, specificity 53.3%).
The AUC of PTX3 was 0.985 (95%CI 0.883 - 1.000, P<0.001), and the optimum cutoff was 5.54 (sensitivity 100%, specificity 90.0%) (Figure 3).
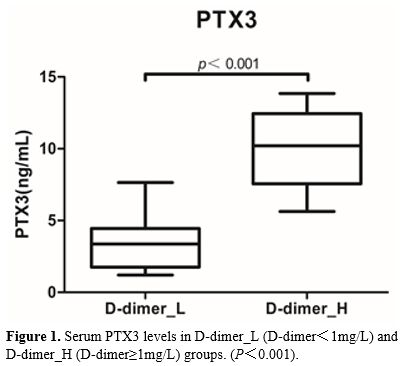 |
Figure 1. Serum PTX3 levels in D-dimer_L (D-dimer<1mg/L) and D-dimer_H (D-dimer≥1mg/L) groups. (P<0.001). |
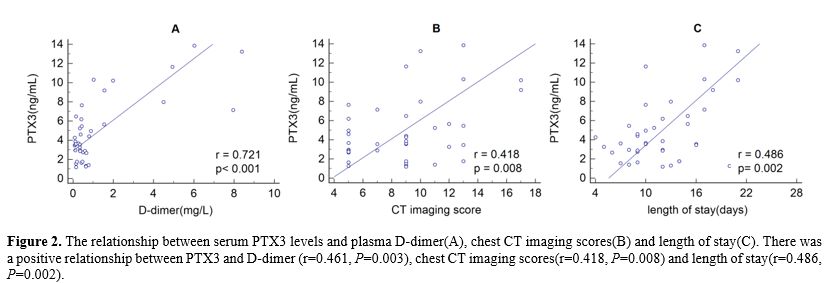 |
Figure 2. The relationship
between serum PTX3 levels and plasma D-dimer(A), chest CT imaging
scores(B) and length of stay(C). There was a positive relationship
between PTX3 and D-dimer (r=0.461, P=0.003), chest CT imaging scores(r=0.418, P=0.008) and length of stay(r=0.486, P=0.002). |
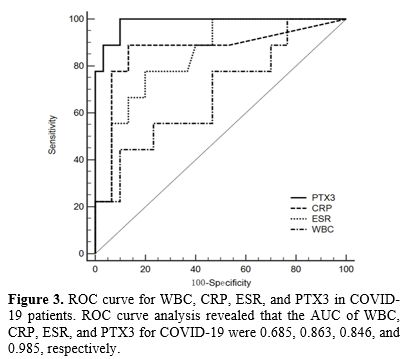 |
Figure 3. ROC curve for
WBC, CRP, ESR, and PTX3 in COVID-19 patients. ROC curve analysis
revealed that the AUC of WBC, CRP, ESR, and PTX3 for COVID-19 were
0.685, 0.863, 0.846, and 0.985, respectively. |
Univariate analysis of categorical variables.
Univariate analysis of different categorical variables showed no
significant group differences in plasma D-dimer levels based on
stratification of gender, smokers, diabetes, and cardiovascular
diseases (Table 3).
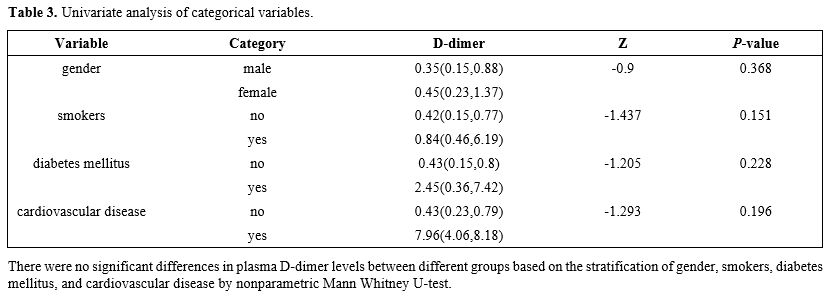 |
Table 3. Univariate analysis of categorical variables.
|
Correlation analysis between continuous variables and plasma D-dimer levels. Pearson’s correlation coefficient analysis showed that there were significant correlations between WBC (r=0.339, P=0.035), NEU (r=0.565, P<0.001) , NLR (r=0.567, P<0.001), CRP (r=0.625, P<0.001), ESR (r=0.623, P<0.001), PTX3 (r=0.721, P<0.001)
and D-dimer,while no significant correlations between age, lymphocyte
counts, monocyte counts, LDL-C, total cholesterol, triglycerides and
D-dimer were observed (Table 4).
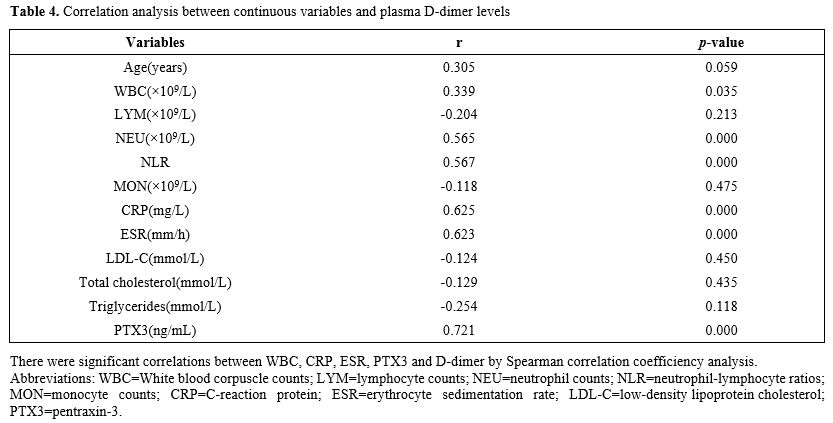 |
Table 4. Correlation analysis between continuous variables and plasma D-dimer levels
|
Linear regression analysis of PTX3 and D-dimer.
D-dimer's influencing factors were analyzed with multiple linear
regression models, and the results showed that PTX3 levels were found
to be independently positively associated with D-dimer levels (ß =
0.451, P=0.006) (Table 5).
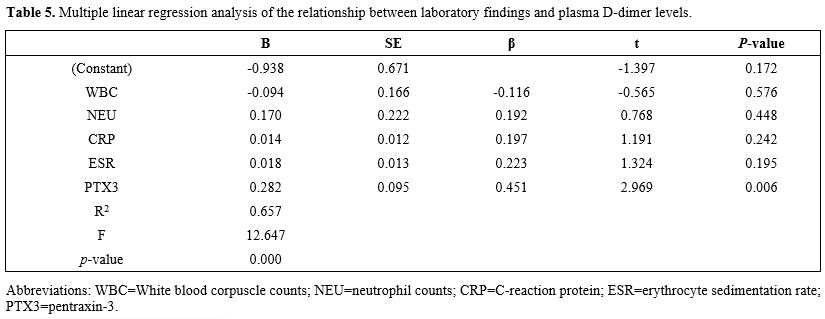 |
Table 5. Multiple linear regression analysis of the relationship between laboratory findings and plasma D-dimer levels.
|
Discussion
To
our knowledge, this is the first study on the role of PTX3 in
coagulopathy in patients with COVID-19. In this study, we divided 39
COVID-19 patients into two groups based on the plasma D-dimer levels on
admission, and ELISA was performed to detect the serum levels of PTX3
in both groups. Our results proved that higher plasma concentrations of
D-dimer were positively associated with higher serum levels of PTX3,
which were also positively associated with higher plasma levels of CRP
and ESR, higher C.T. imaging scores, and longer durations of
in-hospital stay, indicating that the serum levels of PTX3 may
contribute to disease severity and coagulopathy in patients with
COVID-19.
The spectrum of COVID-19 ranges from asymptomatic, fever
and dry cough, gastrointestinal symptoms, coagulation dysfunction, to
multiple organ dysfunction, and it has been described as a process of
systemic inflammation and immune dysfunction, with a large amount of
interleukin (I.L.)-1β, interferon(IFN)-γ, tumor necrosis factor(TNF)-α,
and other cytokines present in the system.[10] PTX3
is upregulated and released by hematopoietic and stromal cells in
response to pro-inflammatory stimuli, such as IL-1β and TNF-α.[11]
It is an essential component of innate immunity's humoral arm,
participating in innate resistance to infections of fungal, bacterial,
and viral pathogens.[12] Besides, PTX3 is an opsonin
for pathogens, facilitating recognition and phagocytosis by neutrophils
in a Complement- and FcγR-dependent manner and by neutralizing virus
infectivity.[13] Moreover, PTX3 exerts its regulatory
function on the inflammatory response by modulating complement
activity, recruiting inflammatory cells through interacting with the
adhesion molecule P-selectin, or affecting apoptotic cells' engulfment.[12] Thus, PTX3 plays a vital role in innate immunity and inflammation.
Acute-phase proteins, such as CRP, serum amyloid A, and ferritin have been well investigated in patients with COVID-19,[14] while the role of PTX3, which is frequently used to diagnose, predict, and evaluate many inflammatory diseases,[3,15]
has not been reported in COVID-19. Elevated PTX3 has been reported to
be associated with disease severity and outcome in infectious diseases.
Studies proved that PTX3 elevated significantly in hospitalized adult
patients with community-acquired pneumonia,[16] and
the admission levels of PTX3 were useful for predicting the severity of
community-acquired pneumonia, independent of possible pathogens,[17]
suggesting it could be used as a biomarker to assess disease severity
and the detection of PTX3 on admission might be useful for clinical
judgment. Although whether PTX3 plays a compensatory protective role or
a detrimental role in COVID-19 patients is unclear, in a mouse model
with a severe acute respiratory syndrome (SARS), PTX3 has been
demonstrated to play a protective role in coronavirus-induced acute
lung injury.[18] Due to the close similarity of viral genome and pathogenicity for SARS-CoV and SARS-CoV2,[19]
it is reasonable to envisage that PTX3 may play a similar protective
role in the process of immune responses, although further research is
needed.
Since the outbreak of COVID-19, it was characterized as
highly contagious and deadly. Coagulopathy has been reported repeatedly
in recent studies, and the high incidence of massive pulmonary embolism
and deep venous thrombosis suggests a pivotal role of coagulopathy in
the deaths of COVID-19.[20] As the smallest
fibrinolysis-specific degradation product found in the circulation,
D-dimer is a very sensitive biomarker for intravascular thrombus and is
markedly elevated in disseminated intravascular coagulation and
pulmonary embolus. It has been reported that higher concentrations of
D-dimer are independently associated with in-hospital mortality in
COVID-19 patients,[21] and the value greater than 1 mg/L helps to identify patients with poor prognosis at an early stage.[7]
In our study cohort, serum PTX3 levels were associated with higher
plasma D-dimer levels, independent of diabetes mellitus, current
smoking, cardiovascular diseases, aging, and dyslipidemia, which
implies that PTX3 may contribute to coagulopathy in patients with
COVID-19.
Endothelial cells express angiotensin-converting enzyme
2 (ACE2), the receptor for SARS-CoV-2, and the interaction of
SARS-CoV-2 and ACE2 possibly mediates endothelial activation, which has
also been confirmed pathologically in patients with COVID-19.[22]
At present, it is believed that PTX3 is dramatically related to
endothelial dysfunction, and several pathogenic pathways, such as
inhibition of nitric oxide (NO) and P-selectin, have been identified.
NO signaling pathway plays a central role in maintaining endothelial
cell functions, regulating platelet aggregation, adhesion, and clot
formation.[23] The inhibition of PTX3 on NO synthesis
leads to endothelial dysfunction, resulting in an imbalance in vascular
homeostasis and a prothrombotic state.[24] P-selectin is a pivotal factor in the initiation of leukocyte and endothelial cell adhesion,[25] while the dysregulated expression of P-selectin contributes to pathological inflammation and deep vein thrombosis.[26] Through interacting with P-selectin, PTX3 promotes vascular inflammatory response and endothelial dysfunction.[27]
Besides, PTX3 may influence coagulation through activating tissue
factors (T.F.). T.F. is the high-affinity receptor and cofactor for
FVII/VIIa. The TF-FVIIa complex is the primary initiator of blood
coagulation and plays a crucial role in hemostasis. By increasing T.F.
expression in endothelial cells, activated monocytes, and
monocyte-derived dendritic cells, PTX3 potentially has a thrombophilic
activity and plays a role in thrombogenesis.[28-30]
In our cohort study, although apparent thrombosis formation was
excluded by Doppler ultrasound in deep veins in the lower extremities
and repeated chest C.T. scans, plasma D-dimer levels were elevated in
nine patients with COVID-19, we speculate that the relationship between
pre-thrombosis levels of D-dimer and thrombotic disease is likely
attributable to microvascular thrombosis formation.[31]
Considering
that PTX3 is produced and released rapidly by damaged tissue cells and
inflammatory cells, it could rapidly respond to the systemic
inflammation at an early stage. Meanwhile, PTX3 was found to be
significantly elevated in severe COVID-19 patients and independently
predicted coagulation abnormalities in our study. Therefore, it is of
great urgency to evaluate the potential therapeutic effects of inducers
or inhibitors of PTX3, anti-PTX3 antibodies,[32] simvastatin,[33] and small interfering RNA (siRNA)[34] in patients with COVID-19.
Limitations
should be noted when interpreting the results of this study. First, the
number of patients was too small (only 39 cases), leading to
statistical deviation. Second, since we did not measure the coagulation
system's direct biomarkers and endothelial dysfunction, the specific
disturbed pathways and mechanisms are still unknown, which deserves
further study. Third, the lack of data on longitudinal samples limited
the evaluation of the prognostic value of PTX3. Fourth, the
relationships between PTX3 and other inflammatory markers (such as IL-6
and fibrinogen) are unclear since those markers were untested in the
study.
Conclusions
In
conclusion, although PTX3 is likely to participate in coagulation and
may serve as a therapeutic target in this direction, the role of PTX3
in COVID-19 is still unclear, and further studies are needed to
determine its reliability.
Acknowledgments
On behalf of the authors, we sincerely thank medical staffs in The Fourth People's Hospital of Yiyang, Hunan, China.
References
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao
X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao
GF, Tan W. A Novel Coronavirus from Patients with Pneumonia in China,
2019. N Engl J Med. 2020 Feb 20;382(8):727-733. https://doi.org/10.1056/NEJMoa2001017 PMid:31978945 PMCid:PMC7092803
- Johns Hopkins University. Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html (Accessed September 1 2020).
- Porte
R, Davoudian S, Asgari F, Parente R, Mantovani A, Garlanda C, Bottazzi
B. The Long Pentraxin PTX3 as a Humoral Innate Immunity Functional
Player and Biomarker of Infections and Sepsis. Front Immunol. 2019
April 12;10:794. https://doi.org/10.3389/fimmu.2019.00794 PMid:31031772 PMCid:PMC6473065
- Zlibut A, Bocsan IC, Agoston-Coldea L. Pentraxin-3 and endothelial dysfunction. Adv Clin Chem. 2019;91:163-179. https://doi.org/10.1016/bs.acc.2019.03.005 PMid:31331488
- Yang
H, Zhang J, Huan Y, Xu Y, Guo R. Pentraxin-3 Levels Relate to the Wells
Score and Prognosis in Patients with Acute Pulmonary Embolism. Dis
Markers. 2019 March 12;2019:2324515. https://doi.org/10.1155/2019/2324515 PMid:30992732 PMCid:PMC6434296
- Escher R, Breakey N, Lämmle B. Severe COVID-19 infection associated with endothelial activation. Thromb Res. 2020 Jun;190:62. https://doi.org/10.1016/j.thromres.2020.04.014 PMid:32305740 PMCid:PMC7156948
- Zhou
F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan
L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical
course and risk factors for mortality of adult inpatients with COVID-19
in Wuhan, China: a retrospective cohort study. Lancet. 2020 Mar
28;395(10229):1054-1062. https://doi.org/10.1016/S0140-6736(20)30566-3
- National Health Commission of the People's Republic of China home page. http://www.nhc.gov.cn (published March 3 2020).
- Guo
W, Li M, Dong Y, Zhou H, Zhang Z, Tian C, Qin R, Wang H, Shen Y, Du K,
Zhao L, Fan H, Luo S, Hu D. Diabetes is a risk factor for the
progression and prognosis of COVID-19. Diabetes Metab Res Rev. 2020 Mar
31;e3319. https://doi.org/10.1002/dmrr.3319 PMCid:PMC7228407
- Huang
C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng
Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H,
Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical
features of patients infected with 2019 novel coronavirus in Wuhan,
China. Lancet. 2020 Feb 15;395(10223):497-506. https://doi.org/10.1016/S0140-6736(20)30183-5
- Bottazzi
B, Inforzato A, Messa M, Barbagallo M, Magrini E, Garlanda C, Mantovani
A. The pentraxins PTX3 and SAP in innate immunity, regulation of
inflammation and tissue remodelling. J Hepatol. 2016 Jun;64(6):1416-27.
https://doi.org/10.1016/j.jhep.2016.02.029 PMid:26921689 PMCid:PMC5414834
- Garlanda
C, Bottazzi B, Magrini E, Inforzato A, Mantovani A. PTX3, a Humoral
Pattern Recognition Molecule, in Innate Immunity, Tissue Repair, and
Cancer. Physiol Rev. 2018 April 1;98(2):623-639. https://doi.org/10.1152/physrev.00016.2017 PMid:29412047 PMCid:PMC5985957
- Reading
PC, Bozza S, Gilbertson B, Tate M, Moretti S, Job ER, Crouch EC, Brooks
AG, Brown LE, Bottazzi B, Romani L, Mantovani A. Antiviral activity of
the long chain pentraxin PTX3 against influenza viruses. J Immunol.
2008 March 1;180(5):3391-8. https://doi.org/10.4049/jimmunol.180.5.3391 PMid:18292565
- Terpos
E, Ntanasis-Stathopoulos I, Elalamy I, Kastritis E, Sergentanis TN,
Politou M, Psaltopoulou T, Gerotziafas G, Dimopoulos MA. Hematological
findings and complications of COVID-19. Am J Hematol. 2020
Jul;95(7):834-847. https://doi.org/10.1002/ajh.25829 PMid:32282949 PMCid:PMC7262337
- Perea
L, Coll M, Sanjurjo L, Blaya D, Taghdouini AE, Rodrigo-Torres D,
Altamirano J, Graupera I, Aguilar-Bravo B, Llopis M, Vallverdú J,
Caballeria J, van Grunsven LA, Sarrias MR, Ginès P, Sancho-Bru P.
Pentraxin-3 modulates lipopolysaccharide-induced inflammatory response
and attenuates liver injury. Hepatology. 2017 Sep;66(3):953-968. https://doi.org/10.1002/hep.29215 PMid:28422322 PMCid:PMC5570620
- Kao
SJ, Yang HW, Tsao SM, Cheng CW, Bien MY, Yu MC, Bai KJ, Yang SF, Chien
MH. Plasma long pentraxin 3 (PTX3) concentration is a novel marker of
disease activity in patients with community-acquired pneumonia. Clin
Chem Lab Med. 2013 Apr;51(4):907-13. https://doi.org/10.1515/cclm-2012-0459 PMid:23152412
- Luo
Q, He X, Ning P, Zheng Y, Yang D, Xu Y, Shang Y, Gao Z. Admission
Pentraxin-3 Level Predicts Severity of Community-Acquired Pneumonia
Independently of Etiology. Proteomics Clin Appl. 2019
Jul;13(4):e1800117. https://doi.org/10.1002/prca.201800117 PMid:30557448
- Han
B, Ma X, Zhang J, Zhang Y, Bai X, Hwang DM, Keshavjee S, Levy GA,
McGilvray I, Liu M. Protective effects of long pentraxin PTX3 on lung
injury in a severe acute respiratory syndrome model in mice. Lab
Invest. 2012 Sep;92(9):1285-96. https://doi.org/10.1038/labinvest.2012.92 PMid:22732935 PMCid:PMC3955193
- Naqvi
AAT, Fatima K, Mohammad T, Fatima U, Singh IK, Singh A, Atif S.M.,
Hariprasad G, Hasan GM, Hassan MI. Insights into SARS-CoV-2 genome,
structure, evolution, pathogenesis and therapies: Structural genomics
approach. Biochim Biophys Acta Mol Basis Dis. 2020 October
1;1866(10):165878. https://doi.org/10.1016/j.bbadis.2020.165878 PMid:32544429 PMCid:PMC7293463
- Wichmann
D, Sperhake JP, Lütgehetmann M, Steurer S, Edler C, Heinemann A,
Heinrich F, Mushumba H, Kniep I, Schröder AS, Burdelski C, de Heer G,
Nierhaus A, Frings D, Pfefferle S, Becker H, Bredereke-Wiedling H, de
Weerth A, Paschen HR, Sheikhzadeh-Eggers S, Stang A, Schmiedel S,
Bokemeyer C, Addo MM, Aepfelbacher M, Püschel K, Kluge S. Autopsy
Findings and Venous Thromboembolism in Patients With COVID-19. Ann Intern Med. 2020 Aug 18;173(4):268-277. https://doi.org/10.7326/M20-2003 PMid:32374815 PMCid:PMC7240772
- Cummings
MJ, Baldwin MR, Abrams D, Jacobson SD, Meyer BJ, Balough EM, Aaron JG,
Claassen J, Rabbani LE, Hastie J, Hochman BR, Salazar-Schicchi J, Yip
NH, Brodie D, O'Donnell MR. Epidemiology, clinical course, and outcomes
of critically ill adults with COVID-19 in New York City: a prospective
cohort study. Lancet. 2020 June 6;395(10239):1763-1770. https://doi.org/10.1016/S0140-6736(20)31189-2
- Varga
Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS,
Mehra MR, Schuepbach RA, Ruschitzka F, Moch H. Endothelial cell
infection and endotheliitis in COVID-19. Lancet. 2020 May
2;395(10234):1417-1418. https://doi.org/10.1016/S0140-6736(20)30937-5
- Gresele
P, Momi S, Guglielmini G. Nitric oxide-enhancing or -releasing agents
as antithrombotic drugs. Biochem Pharmacol. 2019 Aug;166:300-312. https://doi.org/10.1016/j.bcp.2019.05.030 PMid:31173724
- Incalza
MA, D'Oria R, Natalicchio A, Perrini S, Laviola L, Giorgino F.
Oxidative stress and reactive oxygen species in endothelial dysfunction
associated with cardiovascular and metabolic diseases. Vascul
Pharmacol. 2018 Jan;100:1-19. https://doi.org/10.1016/j.vph.2017.05.005 PMid:28579545
- Lam
FW, Da Q, Guillory B, Cruz MA. Recombinant Human Vimentin Binds to
P-Selectin and Blocks Neutrophil Capture and Rolling on Platelets and
Endothelium. J Immunol. 2018 March 1;200(5):1718-1726. https://doi.org/10.4049/jimmunol.1700784 PMid:29335256 PMCid:PMC5821592
- McEver
RP. Selectins: initiators of leucocyte adhesion and signalling at the
vascular wall. Cardiovasc Res. 2015 Aug 1;107(3):331-9. https://doi.org/10.1093/cvr/cvv154 PMid:25994174 PMCid:PMC4592324
- Carrizzo
A, Lenzi P, Procaccini C, Damato A, Biagioni F, Ambrosio M, Amodio G,
Remondelli P, Del Giudice C, Izzo R, Malovini A, Formisano L, Gigantino
V, Madonna M, Puca AA, Trimarco B, Matarese G, Fornai F, Vecchione C.
Pentraxin 3 Induces Vascular Endothelial Dysfunction Through a
P-selectin/Matrix Metalloproteinase-1 Pathway. Circulation. 2015 Apr
28;131(17):1495-505; discussion 1505. https://doi.org/10.1161/CIRCULATIONAHA.114.014822 PMid:25747934
- Napoleone
E, Di Santo A, Bastone A, Peri G, Mantovani A, de Gaetano G, Donati MB,
Lorenzet R. Long pentraxin PTX3 upregulates tissue factor expression in
human endothelial cells: a novel link between vascular inflammation and
clotting activation. Arterioscler Thromb Vasc Biol. 2002 May
1;22(5):782-7. https://doi.org/10.1161/01.ATV.0000012282.39306.64 PMid:12006390
- Napoleone
E, di Santo A, Peri G, Mantovani A, de Gaetano G, Donati MB, Lorenzet
R. The long pentraxin PTX3 upregulates tissue factor in activated
monocytes: another link between inflammation and clotting activation. J
Leukoc Biol. 2004 Jul;76(1):203-9. https://doi.org/10.1189/jlb.1003528 PMid:15226367
- Kasuda
S, Sakurai Y, Tatsumi K, Takeda T, Kudo R, Yuui K, Hatake K.
Enhancement of Tissue Factor Expression in Monocyte-Derived Dendritic
Cells by Pentraxin 3 and Its Modulation by C1 Esterase Inhibitor. Int
Arch Allergy Immunol. 2019;179(2):158-164. https://doi.org/10.1159/000496744 PMid:30893690
- Magro
C, Mulvey JJ, Berlin D, Nuovo G, Salvatore S, Harp J, Baxter-Stoltzfus
A, Laurence J . Complement associated microvascular injury and
thrombosis in the pathogenesis of severe COVID-19 infection: A report
of five cases. Transl Res. 2020 Jun;220:1-13. https://doi.org/10.1016/j.trsl.2020.04.007 PMid:32299776 PMCid:PMC7158248
- Gatto
M, Ghirardello A, Luisetto R, Bassi N, Fedrigo M, Valente M, Valentino
S, Del Prete D, Punzi L, Doria A (2016) Immunization with pentraxin 3
(PTX3) leads to anti-PTX3 antibody production and delayed lupus-like
nephritis in NZB/NZW F1 mice. Journal of autoimmunity 74:208-216. https://doi.org/10.1016/j.jaut.2016.07.002 PMid:27405845
- Yokota
K, Miyoshi F, Sato K, Asanuma Y, Akiyama Y, Mimura T (2011)
Geranylgeranyl-pyrophosphate regulates secretion of pentraxin 3 and
monocyte chemoattractant protein-1 from rheumatoid fibroblast-like
synoviocytes in distinct manners. Clinical and experimental
rheumatology 29 (1):43-49
- Margheri F,
Serratì S, Lapucci A, Chillà A, Bazzichi L, Bombardieri S, Kahaleh B,
Calorini L, Bianchini F, Fibbi G, Del Rosso M (2010) Modulation of the
angiogenic phenotype of normal and systemic sclerosis endothelial cells
by gain-loss of function of pentraxin 3 and matrix metalloproteinase
12. Arthritis and rheumatism 62 (8):2488-2498. https://doi.org/10.1002/art.27522 PMid:20506099
[TOP]