We reported eight children admitted with MIS-C. Seven patients were boys. The median age was eight years (interquartile range IQR:4-10 years). All children were previously fit and well. No one had obesity. The first patient with confirmed MIS-C in our cohort was admitted on November 3, 2020. Known exposure to COVID-19 was reported in 4 cases. Demographic, clinical data, laboratory test findings, and echocardiographic findings were shown in table 1.
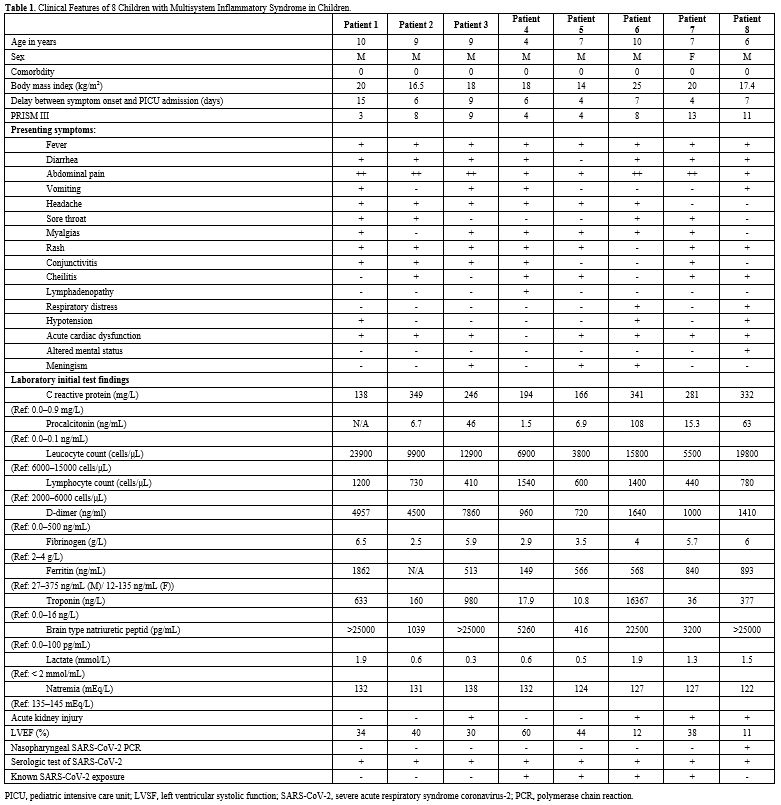 |
Table
1. Clinical Features of 8 Children with Multisystem Inflammatory Syndrome in Children. |
Fever and gastrointestinal symptoms associated with pain were reported in all cases. The median delay between fever and PICU admission was 6.5 days (IQR: 4-15 days). Five patients had marked abdominal pain and were examined by the surgeon for possible appendicitis. Abdominal echography was performed in 3 cases, and an abdominal computed tomography scan in one case and showed mesenteric lymphadenitis in 2 cases and a peritoneal effusion pelvic fluid in 1 case. Seven patients had diarrhea. On examination, we found rash (n=7), conjunctivitis (n=7), cheilitis (n=5), and meningism (n=3). A lumbar puncture was performed in one case before admission in PICU for possible meningitis. We reported cardiac dysfunction in 7 cases and shock with hypotension in 3 cases. The LVEF was less than 30% in 2 subjects who presented the most severe MIS-C form with higher inflammation markers (C-reactive protein, procalcitonin).
Laboratory test findings showed an increased level of C-reactive protein and procalcitonin in all cases without microbial cause. We reported lymphopenia, increased fibrinogen level, and D-dimer levels in all patients. Troponin and pro-brain natriuretic peptide (pro-BNP) levels were elevated in all cases presenting with cardiac dysfunction; however, the lactate level was normal. Four patients had an acute kidney injury. Two patients had an increase in lipase levels up to 3 times average.
All patients had positive SARS-COV-2 serology. Only one patient had a positive nasopharyngeal RT-PCR SARS-COV-2 testing, as shown in table 1.
Treatment and outcomes for our cohort were shown in table 2. All patients required respiratory support; three were mechanically ventilated and had severe cardiac dysfunction with hypotension. Echocardiographic measures improved under inotropic agents (dobutamine and milrinone). One patient required levosimendan. Complete recovery of left ventricular function was observed at a median delay of 4 days (IQR: 1-7 days) after admission. All patients received intravenous immunoglobulin (IVIG:1 dose of 2 grams per kilogram), methylprednisolone (10 milligrams per kilogram per day for three days), and a low dose of aspirin. Low-molecular-weight-heparin was administered in five patients. Antibiotics were used in two cases, but the treatment has been stopped on day 3. The median duration of fever was one day (IQR: 1-4 days). No abnormality in the coronary artery was found. No deaths occurred in our small cohort. All patients were discharged from PICU after a median length of stay of 5.5 days (IQR: 2-10 days). All children will be monitored into the future for the follow-up.
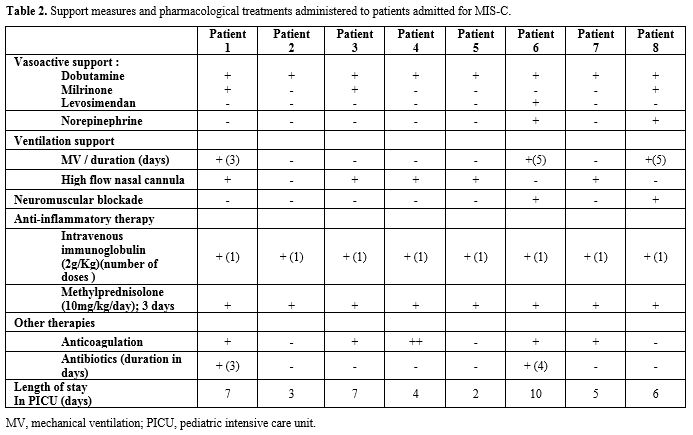 |
Table
2. Support measures and pharmacological treatments administered to patients admitted for MIS-C. |