Since February 2020, Italy has faced one of the worst medical emergencies spanning centuries, the SARS-CoV-2 virus pandemic. Lombardia region had the highest number of deaths in Italy and one of the highest mortality rates worldwide.[1,2] Fear and anxiety about a new disease and what could happen can cause strong emotions in adults and children.[3-5] Public health actions, such as social distancing, can make people feel isolated and increase stress and anxiety. Patients with pre-existent chronic morbidities can feel more stressed and anxious about their health and healthcare support.[6] In addition, the pandemic caused a drastic reduction of spaces and medical and nurse staff dedicated to outpatients suffering from rare diseases because of the urgent needs in the intensive, sub-intensive, and ward units. Accordingly, outpatient medical services warranted only non-deferrable care.
In our Centre, we regularly follow patients with hereditary anemias and hemochromatosis. All of them require scheduled check-ups, but their therapeutic needs are quite different, which means that the SARS-CoV-2 pandemic impacted patients' management. While the Centre was able to guarantee non-deferrable therapies in thalassemia and sickle cell patients, checks or phlebotomies in hemochromatosis were limited to urgent needs. Our aim was to evaluate these patients' emotional responses during the pandemic through an online survey. Eighty patients with transfusion-dependent thalassemia, patients with sickle cell diseases undergoing regular transfusion or erythro-exchange and other transfusion-dependent anemias (ThSA), plus 100 patients with hemochromatosis (HH) received the questionnaire. The questionnaire includes 35 items regarding anagraphic data, health and emotional status, perception of risk, and social support[7] during the pandemic (details on request). Patients were asked to answer anonymously and voluntarily.
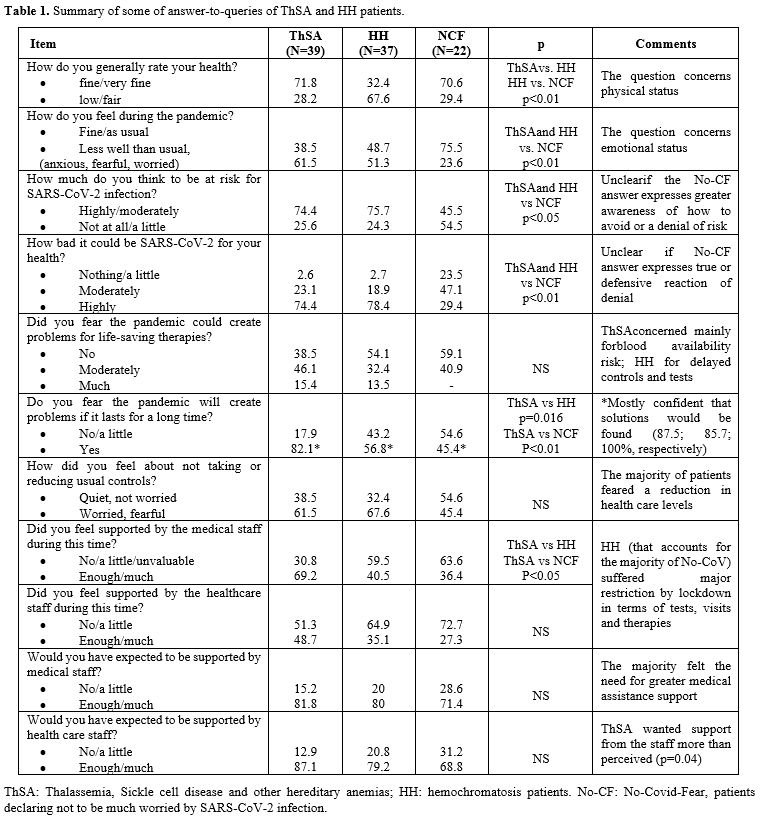
The questionnaire was answered by 44/80 ThSA (55%) and 54/100 HH (54%). ThSA and HH patients differed for age (39.1+14.4 vs 57.2+9.5 years, respectively; p<0.0001) and gender (men 59.1% vs 87%, respectively; p=0.0026). 93% of ThSA were resident in Lombardia during the pandemic and 74% HH in northern regions. About half of the patients were aware of relatives, friends, acquaintances affected, or dead by SARS-CoV-2 infection. There was no difference in patients' answers according to gender apart from a single item: more ThSA females (78%) feared the pandemic could create problems in life-saving therapy management than males (46%) (p=0.035), in agreement with other reports showing the lesser psychological impact of Covid-19 outbreak in males than females.[3,8] The SARS-CoV-2 infection severity perception was high or very high in 88.6% of ThSA and 68.5% in HH (p=0.018). 17 HH (31.5%) and 5 (11.4%) ThSA patients declared not to be worried about SARS-CoV-2 infection (p=0.027). These patients did not differ according to gender, age, and geographical origin. They were considered apart (NCF) and compared to the other groups (ThSA and HH), as summarised in Table 1.
 |
Table
1. Summary of some of answer-to-queries of ThSA and HH patients. |
Both ThSA and HH reported highly and moderately frequent anxiety (64.1% and 67.6%, respectively) as well as worries and concern regarding the SARS-CoV-2 pandemic (82.1% and 91.9%, respectively) higher than reported in China's general population.[9,10] Forty-one percent of ThSA and 59.5% of HH would have expected more information about SARS-CoV-2 infection and therapies, more listening, and greater swab and/or serology testing availability.
Our findings show that SARS-CoV-2 pandemic had a marked impact on patients' emotions. ThSA were more worried than HH patients, possibly because of their different needs but were more confident about the future than HH (74.5% vs. 54%, p<0.02), probably on account of their younger age. A large number of ThSA were concerned about the risk of reduced blood supply, a fear amplified by the media's early alarmistic reports, but not justified in fact. The restrictions caused by the pandemic on the availability of adequate spaces and health personnel increased the patients' fears and concerns about their own health: one-fourth of ThSA and even more HH felt they were not supported as much as desired during pandemics. Also, about 40% of ThSA and more than half HH asked for more attention, information, and SARS-Cov-2 infection protection. NCF patients seemed to minimize the severity and risk of Covid-19, which contrasts with their demand for more information, reassurance, and support similar to that of the other groups. We believe that such an attitude might suggest a defensive denial and yet no real sense of security.
Despite the limited number of participants, this survey has the advantage of focusing on two specific subsets of patients with rare diseases requiring either undeferrable life-saving therapies or just regular checks. Rare diseases include a wide range of pathologies but share common features, including the need for multidisciplinary support related to the complexity of diseases, adequate structures, and complementary services, investments in education, and hospital job placement of medical and staff personnel (www.eurordis.org). Unfortunately, these are not often a priority for the national and local health authorities. Hospital reallocation of spaces, doctors, and nurses induced by the pandemic is likely to have brought back to the patients the perception that their pathology was taken into little account. Indeed, our survey showed a high level of anxiety and concern in the patients resulting from several components: i. general fear for a new and potentially lethal disorder;[5] ii. additional disease-related risk;[11] iii. decreased standard care, including reduced spaces, access to therapies, laboratory tests, and medical visits. All the patients wished for greater support from the medical and health staff. Regional and local authorities ought to take particular notice of these remarks in order to guarantee adequate management of patients with rare diseases according to the European and Italian regional resolutions (www.regione.lombardia.it), even in the case of an emergency as SARS-CoV-2 was and could be in the next future. In addition to and in close connection with this, our results suggest the need for exhaustive information to be provided at adequate times and in suitable places. We believe information is the major requirement since we need to develop "healthy concern" in patients to contain both their anxiety and defensive attitude, thus preventing them from denial with ensuing greater exposure to risk.