We present a case of vaccine-induced prothrombotic immune thrombocytopenic (VIPIT) disorder following ChAdOx1 nCoV-19 vaccine in a 29 years old, previously healthy, Caucasian female, which manifested with superior ophthalmic vein (SOV) thrombosis and thrombocytopenia.[3,4] The patient was referred to our Clinic on March 30, 2021, complaining of severe headache, left orbital swelling, and blurred left eye vision. Initial findings showed thrombocytopenia of 18 × 109 per L in association with high D-dimers levels of 35712 μg/L. At physical examination, the patient showed left eyeball swelling with proptosis, limited ocular motility, and diplopia at the vertical gaze (Figure 1a).
The symptoms dated one day before admission, starting with flu-like symptoms and fever. She has received the first dose of vaccine against SARS-CoV-2, ChAdOx1 nCoV-19, ten days before admission. Her medical and pharmacological history were unremarkable negative. She also reported one day of fever after the vaccination. The CT scan of the head was normal. Diagnostic blood examinations showed a normal blood smear, apart from the thrombocytopenia, elevated CRP (142 mg/L), and normal prothrombin, activated partial thromboplastin, and thrombin time and fibrinogen level (2.5 g/L). The nasopharyngeal swab for SARS-CoV2 nucleic acid testing was negative, and serology revealed the presence of SARS-CoV-RBD IgG 59.46 and IgM 1.5 AU/ml, although the patient had no history of infection since the pandemic started.
Contrast-enhanced MRI demonstrated central filling defects (Figure 1b) and hyper T2 signal (Figure 1c) in the left superior ophthalmic vein (SOV), revealing thrombosis.[5]
Screening for antibodies for Heparin/Platelet Factor 4 (PF4) complex using a particle gel immune assay (ID-PaGIA Heparin/PF4 Antibody test) revealed a very high level of antibodies agents the PF4 complex.[6]
Testing for hereditary thrombophilia (Factor V Leiden R506Q mutation, Prothrombin G20210A gene mutation) and other triggers for thrombosis and thrombocytopenia, including lupus anticoagulant, protein C and S activity, cardiolipin IgG and IgM antibodies, hepatitis B and C virus, HIV, cytomegalovirus, and Helicobacter pylori infection, were all negative.
The presence of elevated D-dimers in association with immune thrombocytopenia and MRI-confirmed thrombosis make the diagnosis of vaccine-induced prothrombotic immune thrombocytopenia (VIPIT) probable.[3] Treatment for this condition was initiated following the recommendation of the Drugs & Biologics Clinical Practice Guidelines Working Group and the Ontario COVID-19 Science Advisory Table.[4] Intravenous immunoglobulin (IVIG) 1 g/kg of body weight daily for two days, broad-spectrum antibiotics and direct oral anti-Xa inhibitor, Rivaroxaban, 15 mg twice daily for 21 days were administrated. Afterward, immunosuppression was continued with oral prednisolone 1 mg/kg bw for seven days, with tapering afterward. The patient recovered remarkably rapidly, all the symptoms resolved within 4 to 5 days (Figure 1d), platelets raised to normal level after a week of treatment, and the D-dimer levels went to normal after two weeks of treatment. The patient was discharged home after six days. She is still on prednisolone and Rivaroxaban 20 mg daily and will continue for another two months.
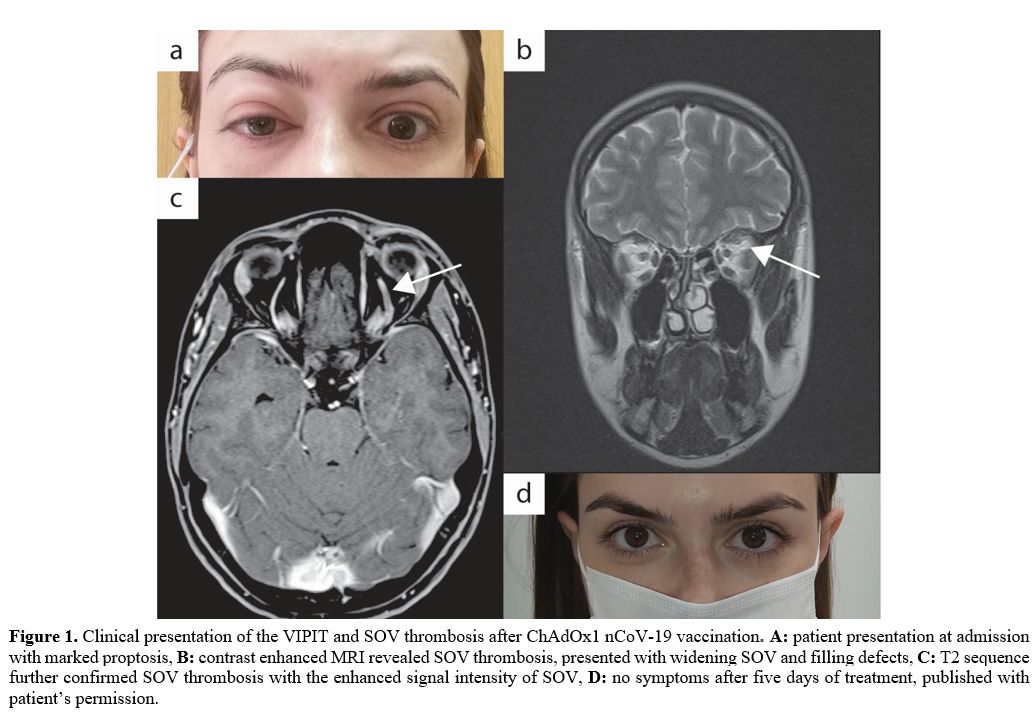 |
Figure
1. Clinical presentation of the VIPIT and SOV thrombosis after ChAdOx1
nCoV-19 vaccination. A: patient presentation at admission with marked
proptosis, B: contrast enhanced MRI revealed SOV thrombosis, presented with widening SOV and filling defects, C: T2 sequence further confirmed SOV thrombosis with the enhanced signal intensity of SOV, D: no symptoms after five days of treatment, published with patient’s permission. |
Since April 9, 2021, the EMA has been listed the condition of unusual blood clots with low blood platelets occurring in the first two weeks after the ChAdOx1 nCoV-19 vaccine as a very rare side effect of this vaccine. A few weeks later, the FDA associated the same side effect with the Janssen ad26.cov2.s (COVID-19) vaccine. Thus, both regulatory agencies underline that the benefits of both vaccines are far greater than their risk.[7,8]
Most of the reported VIPT patients presented with cerebral venous sinus and splanchnic vein thrombosis, but other rare thrombotic complications are possible, and our case of SOV thrombosis is the second-ever described.[5]