In August 2021, a 55-years-old male was admitted to our hospital because of abdominal distension, nausea, and vomiting. He had a history of prostatic cancer treated surgically in 2016 and PTCL-NOS treated in 2017 with six cycles of CHOEP (Cyclophosphamide, Doxorubicin, Vincristine, Etoposide, and Prednisone) followed by autologous stem cell transplant (ASCT) obtaining complete disease remission. On admission, laboratory findings showed anemia (Hb 9.4 g/dL), mild leucocytosis (WBC 12630/mm3 Neu 11540/mm3), hypoalbuminemia (2.8 g/dL), high serum creatinine levels (4,9 mg/dL), hyperuricemia (16,6 mg/dL), and elevated LDH levels (1297 UI/L, normal value <225 UI/L). On clinical examination, he had ascites but no palpable superficial lymph nodes. Computed tomography (CT) without contrast showed peritoneal effusion and thickening at mesenteric and mesogastric fatty tissue levels. Splenomegaly (16 cm) and the portal vein of increased caliber (17 mm) were also detected. A paracentesis was performed, obtaining 4 liters of a cloudy, straw-colored ascitic fluid (AF) with high protein content (3.9 gr/dL), remarkable LDH values (4296 UI/L), and glucose (16 mg/dL). We studied the AF with eight-color multiparametric flow cytometry (MFC) using combinations of monoclonal antibodies. MFC analysis of the AF detected 95% of highly scattered lymphoid B cells, positive for CD45/CD79a/CD19/CD22/CD38/CD18/CD11a/CD27/CD49d/HLA-DR, CD20 partially expressed (20%), kappa light chain restricted and negative for CD5/CD200/FMC7/CD79b/CD10/VS38/CD13/CD33/CD14/CD15/CD11b/CD16/CD56/CD138/MPO/cCD3/NG2/CD123 (Figure 1a). Considering the previous diagnosis of PTCL-NOS, an accurate assessment of T-cells was also performed through immunophenotypic analysis of V Beta Repertoire,[3] which did not detect alterations in any of the 24 families studied.
Cytological examination of ascitic fluid (1000 ml) with May-Grunwald-Giemsa (MGG) stain revealed numerous lymphoid cells of medium to large size, often in apoptosis and sometimes in mitosis. Most cells had round nuclei, prominent nucleoli, and abundant deeply basophilic finely vacuolated cytoplasm (Figure 1b). The remaining concentrated sediment was fixed in 10% formalin, embedded in paraffin, and processed to cell block to perform immunohistochemistry (IHC). Lymphoma cells were immunoreactive for CD79a, CD20 (about 30%), PAX5 (weak and diffuse), MUM1, cMyc (>40%) and BCL2 (>50%) and non-immunoreactive for HHV8, CD3, CD5, CD4, CD8, CD10, CD30, CD138, and BCL6. We performed a molecular biology investigation to evaluate T-cell clonality arising out of a previous diagnosis of PTCL-NOS and to study the B-cell population in the first biopsy at the presentation in 2017. The lymph node and AF were investigated for the presence of immunoglobulins (IG) and T-receptor (TR) clonal rearrangements by qualitative polymerase chain reaction (PCR). All positive targets were sequenced to identify the type of rearrangement and its clonal feature. The screening showed different targets: one was immunoglobulin heavy chain (IGH) gene rearrangements on ascitic fluid, and two resulted in TR gamma chain positive on lymph node biopsy. No common targets were identified between the two samples. Based on these findings, the patient was diagnosed with large B-cell lymphoma of new onset, presenting as peritoneal lymphomatosis. Gastrointestinal localization of disease was excluded by esophagogastroduodenoscopy (EGDS) and recto-colon-sigmoidoscopy (RSCS). Due to the patient poor clinical conditions, a Gemcitabine-based regimen was chosen to obtain a mild clinical improvement. After one week, he received a second infusion of Gemcitabine, but three days later, his clinical conditions worsened again due to fever and pancytopenia. Considering the normalization of serum creatinine (1.1 mg/dL) and the recurrence of abdominal distention, a total body CT scan with contrast confirmed the presence of an abundant amount of ascitic effusion and mesenteric thickening as an omental cake pattern, referring to peritoneal localization of the disease. Small mesenteric lymphadenopathies (15 mm) were observed. Unfortunately, clinical conditions worsened, and the patient died the following day.
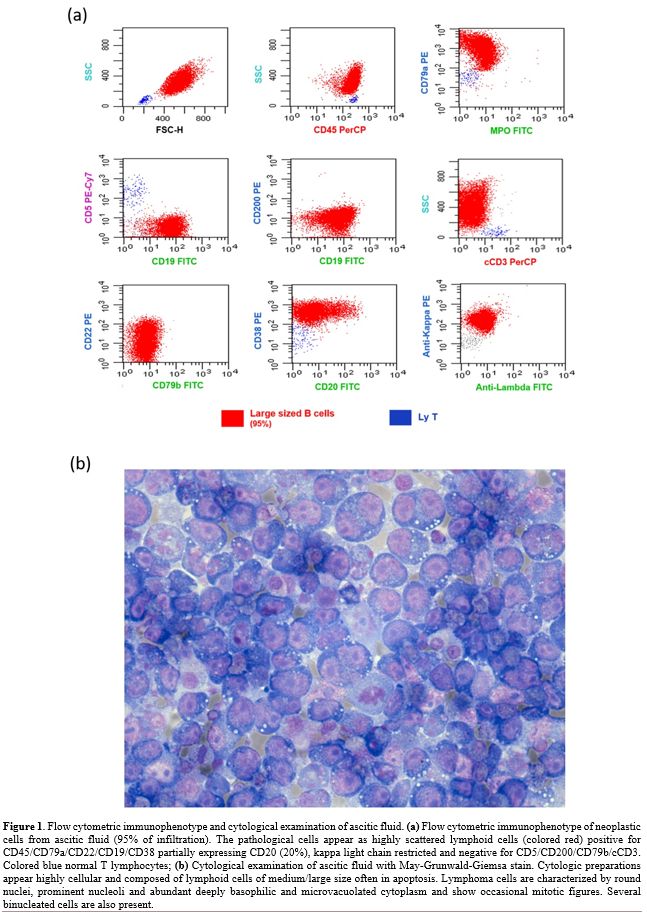 |
Figure 1. Flow cytometric immunophenotype and cytological examination of ascitic fluid. (a) Flow cytometric immunophenotype of neoplastic cells from ascitic fluid (95% of infiltration). The pathological cells appear as highly scattered lymphoid cells (colored red) positive for CD45/CD79a/CD22/CD19/CD38 partially expressing CD20 (20%), kappa light chain restricted and negative for CD5/CD200/CD79b/cCD3. Colored blue normal T lymphocytes; (b) Cytological examination of ascitic fluid with May-Grunwald-Giemsa stain. Cytologic preparations appear highly cellular and composed of lymphoid cells of medium/large size often in apoptosis. Lymphoma cells are characterized by round nuclei, prominent nucleoli and abundant deeply basophilic and microvacuolated cytoplasm and show occasional mitotic figures. Several binucleated cells are also present. |
Peritoneal lymphomatosis is a rare form of extranodal lymphoproliferative disease, frequently associated with diffuse large B-cell lymphoma (DLBCL) and Burkitt's lymphoma.[3] Considering the recent history of PTCL-NOS in our patient, a relapse of the T-cell disease was suspected, although T-cell peritoneal lymphomatosis is extremely rare and usually secondary to intestinal localization.[4] Thanks to a prompt MFC exam with cytology and IHC afterward, we obtained an early diagnosis by avoiding a biopsy exam. Although DLBCL is ideally diagnosed from an excisional biopsy of a suspicious lymph node or tissue, morphologic and cytometry exams should be considered when an invasive diagnostic procedure is not possible. Immunophenotyping by MFC is a rapid and efficient technique adjunct to conventional diagnostic cytopathology in evaluating serous effusions for lymphomatous involvement.[5-6] Studies like MFC and IHC staining help lead to an accurate diagnosis allowing the identification of the molecular characteristics of the lymphoma and its immunophenotype, which dictate treatment decisions.[7-10] This case was interesting as the clinical signs and symptoms could suggest a relapse of PTCL-NOS diagnosed and treated four years before; however, FCM, cytology with IHC, and molecular biology investigations excluded this hypothesis.
In conclusion, MFC could be an extremely useful and rapid method in the integrated diagnostic process with cytology and IHC to obtain a proper diagnosis of NHL to quickly start appropriate therapy, also in the absence of tumor samples for a complete histopathology examination.