Received: August 29, 2014
Accepted: September 25, 2014
Meditter J Hematol Infect Dis 2014, 6(1): e2014070, DOI 10.4084/MJHID.2014.070
This article is available on PDF format at:

Giorgia Sulis1, Alberto Roggi1, Alberto Matteelli2 and Mario C. Raviglione2
1 University
Division of Infectious and Tropical Diseases, WHO Collaborating Centre
for TB/HIV collaborative activities and for TB elimination, University
of Brescia, Brescia, Italy.
2 Global Tuberculosis Programme, World Health Organization, Geneva, Switzerland.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Tuberculosis (TB) is a major public
health concern worldwide: despite a regular, although slow, decline in
incidence over the last decade, as many as 8.6 million new cases and
1.3 million deaths were estimated to have occurred in 2012. TB is by
all means a poverty-related disease, mainly affecting the most
vulnerable populations in the poorest countries. The presence of
multidrug-resistant strains of M. tuberculosis in most countries, with
somewhere prevalence is high, is among the major challenges for TB
control, which may hinder recent achievements especially in some
settings. Early TB case detection especially in resource-constrained
settings and in marginalized groups remains a challenge, and about 3
million people are estimated to remain undiagnosed or not notified and
untreated. The World Health Organization (WHO) has recently launched a
new global TB strategy for the “post-2015 era” aimed at “ending the
global TB epidemic” by 2035. This strategy is based on the three
pillars that emphasize patient-centred TB care and prevention, bold
policies and supportive systems, and intensified research and
innovation. This paper aims to provide an overview of the global TB epidemiology as well as of the main challenges that must be faced to eliminate the disease as a public health problem everywhere. |
Introduction
Tuberculosis (TB) is a major public health concern worldwide:
despite a regular, although slow, decline in incidence over the last
decade, as many as 8.6 million new cases and 1.3 million deaths were
estimated to have occurred in 2012. TB is by all means a
poverty-related disease, mainly affecting the most vulnerable
populations in the poorest countries. The presence of
multidrug-resistant strains of M. tuberculosis in most countries, with
somewhere prevalence is high, is among the major challenges for TB
control, which may hinder recent achievements especially in some
settings. Early TB case detection especially in resource-constrained
settings and in marginalized groups remains a challenge, and about 3
million people are estimated to remain undiagnosed or not notified and
untreated. The World Health Organization (WHO) has recently launched a
new global TB strategy for the “post-2015 era” aimed at “ending the
global TB epidemic” by 2035. This strategy is based on the three
pillars that emphasize patient-centred TB care and prevention, bold
policies and supportive systems, and intensified research and
innovation.
This paper aims to provide an overview of the global
TB epidemiology as well as of the main challenges that must be faced to
eliminate the disease as a public health problem everywhere.
Global Epidemiology
According to the World Health Organization (WHO), about 8.6 million
cases (8.3-9.0 million) were estimated to have occurred in 2012,
approximately 2.9 of whom were in women. Most cases are estimated to be
in Asia and Africa (58% and 27% respectively), with the highest
incidence in India (range 2.0-2.4 million) and China (0.9 -1.1
million), together accounting for 38% of the total number of cases.[1]
The
global TB incidence rate slowly declined from 1997 to 2001, with an
increase in 2001 (due to the rising number of cases among HIV-infected
patients in Africa) (Figure 1).
Subsequently, a 1.3% per year average reduction rate has been observed
since 2002, reaching 2.2% between 2010 and 2011. The absolute number of
cases is also currently decreasing, though this declining trend only
began in 2006. Based on these findings, the Millennium Development Goal
6 Target for tuberculosis (i.e. “to halt and begin to reverse the
incidence”) has already been achieved.
Twelve million (11-13
million) prevalent cases of TB were estimated in 2012, corresponding to
about 169 cases per 100 000 population.[1] TB prevalence is declining
globally since the early 1990s (before incidence started to decline).
This decline is largely attributed to the progressive introduction of
the DOTS strategy which, by emphasizing bacteriological diagnosis and
standard short-course chemotherapy with direct observation of
treatment, may have significantly contributed to the reduction of
chronic and untreated cases, as well as to the duration of illness (Figure 1).
Nevertheless, the Stop TB Partnership target of halving the 1990
prevalence rate by 2015 will probably be missed (a reduction of 37% was
registered in 2012, 169 / 100 000 compared to 263 / 100 000 in 1990),
because of the delays in the African and the European WHO
regions.
TB mortality was estimated at 1.3 million
deaths (1.0-1.6 million) in 2012, including 320 000 (300 000 - 340 000)
HIV-associated cases. A 45% drop in TB mortality rate has been observed
globally since 1990 (Figure 1).[1]
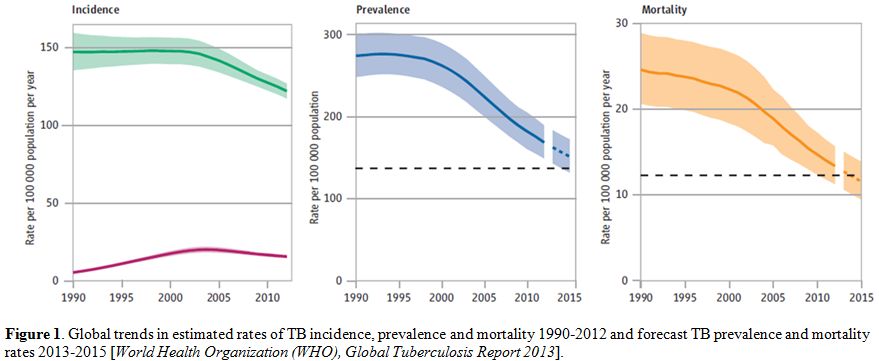 |
Figure 1. Global trends in estimated rates of TB incidence, prevalence and mortality 1990-2012 and forecast TB prevalence and mortality rates 2013-2015 [World Health Organization (WHO), Global Tuberculosis Report 2013]. |
The
traditional case detection rate (CDR), defined as the proportion of
notified cases among the estimated number of new and relapse TB cases,
thought to have occurred in a given year, is a problematic indicator in
TB epidemiology, though it could potentially provide very useful
information on the “diagnostic capacity” of a TB control program.[2]
The denominator consists of an estimate: significant efforts are
currently ongoing to obtain reliable estimates through the performance
of costly prevalence surveys but coverage is still limited.[3] In 2012,
6.1 million TB cases were notified by the National TB Programs
(NTPs). 5.4 million were new cases, and 0.3 million were relapses
(with India and China showing the highest notification rates: 39%
overall); 0.4 million cases of retreatment (excluding relapses) were
also reported. Most newly diagnosed patients had pulmonary TB, and more
than half of them were sputum smear positive.[1] CDR reached 66%
(64-69%) in 2012 with several regional differences. In other words,
one-third of cases, corresponding to an estimated 3 million cases, was
missed that year. This implies that a significant proportion of TB
patients remains either unrecognized and untreated or not notified. The
former actively contribute to further transmission of the disease. The
latter may be detected outside of national programs and managed
inappropriately, also contributing to further transmission and creation
of drug resistance. Further improvements in diagnostic capacity and
surveillance system are needed in some Regions such as South-East Asia,
Africa, and Eastern Mediterranean.
Treatment outcome
represents a useful process indicator to be closely monitored, being a
measure of progress in expanding access to quality-assured care.
Approximately 22 million lives are estimated to have been saved since
1995, when the DOTS strategy was introduced. The proportion of
successfully treated patients, currently reaching 87% at global level,
is significantly lower than the average, in some WHO regions, like the
European one (probably due to the high failure rate associated to
MDR-TB) and in the African one (due to the high rate of deaths or
defaulting linked to HIV co-infection).[1]
The Challenge of Controlling the Disease in the most Vulnerable Populations
Since TB does not homogeneously affect the population, selected
high-risk groups should be identified in all settings as they deserve
special attention and should be addressed specifically with additional
interventions.
TB is mostly a poverty-related disease: this can
explain its uneven distribution in different population groups. Poor
housing and environmental conditions, food insecurity, financial
difficulties, illiteracy, unfavourable psycho-social circumstances are
among the major determinants of TB and concomitantly affect the
capacity of sick persons to access healthcare services.[4-9]
Well-defined
vulnerable groups include people living with HIV infection, prisoners,
homeless people, migrants/refugees, and substance or heavy alcohol
users. Besides the increased risk of exposure to M. tuberculosis,
vulnerable groups are also more likely to progress to active disease
once they are infected due to the immunocompromised status of their
underlying condition. Moreover, in some of these groups TB may remain
for a long time undiagnosed, thus representing a source of infection
for the entire community.[10]
Social marginalization is often
responsible for a limited access to health services leading to
diagnostic delay, clinical worsening and poor adherence to treatment,
and eventually to a less favourable outcome.[11-13] A common
discouraging factor to seek medical care is the fear of stigmatization
that is also an important determinant of poor adherence. The most
fragile populations should be identified in each country in order to
develop and implement tailored interventions aimed at addressing the
needs of hard-to-reach groups. Global disease control will not be
achieved without a cross-cutting approach towards these social
determinants of the disease.
TB/HIV co-infected patients.
People living with HIV/AIDS (PLHIV) are at extremely high risk of TB,
due to the immunological impairment associated to this infection and to
frequent co-existence of deprived social conditions.
In 2012, 1.1
million TB cases (i.e. 13% of the total) were estimated to have
occurred among PLHIV, whom 75% were reported in a few African
countries; where more than 60% of tested TB patients resulted
HIV-positive. Notably, since 2.8 million notified TB patients knew
their HIV status, and 20% of those tested were positive, the number of
notified HIV-infected TB patients was approximately 550 000. This group
represents about half of the number of cases estimated to have occurred
that year.
The number of deaths among HIV-infected TB patients
amounted to 0.3 million in 2012 with no relevant differences between
men and women.
Data from countries that reported treatment
outcomes disaggregated by HIV status showed a lower treatment success
rate for new HIV-positive TB cases (73%) compared to HIV-uninfected
cases (87%).[1] The case fatality rate is specifically high among
HIV-infected TB patients: merging the death and default outcomes (most
defaulting cases will eventually die), this category accounts for 19%
of HIV-positive treated cases globally.
All newly diagnosed TB
patients should be aware of their HIV condition, according to
recommended collaborative TB/HIV interventions.[14] The trend in the
percentage of TB patients knowing their HIV status has continued to
increase since 2004, reaching a peak of 46% in 2012.[1] However, HIV
testing coverage varied widely between countries, with a 74% peak in
the African region. Much lower rates were reported in the Eastern
Mediterranean Region (EMR) and South-East Asia Region (SEAR) (14% and
39% respectively), while the European (EUR) and American Regions (AMR)
slightly exceeded a 60% coverage.[15]
Though WHO recommends that
all TB/HIV co-infected patients must receive timely antiretroviral
therapy (ART) regardless of their CD4+ count,[16] this goal is still
far from being achieved satisfactorily in most countries with an
average coverage of 57% in 2012 at global level (55% in the African
region). Expanding the coverage of ART among HIV-infected TB patients
represents the highest current priority for TB/HIV interventions in
countries with a high burden of both diseases.
Furthermore, data
on the provision of isoniazid preventive therapy (IPT) to PLHIV show an
unsatisfactory level of implementation. Only 42 countries currently
reported on this indicator and just 0.5 million persons initiated it in
2012. In short, indicators to monitor TB/HIV interventions suggest that
progress has been real in the past decade. At the same time, some
interventions with life-saving potential such as timely ARV
administration and IPT are not yet fully implemented.
TB in prisons.
The world prison population is currently estimated at approximately
8-10 million people with a considerably high turnover.[17] TB
represents a major concern for jailed persons, due to overcrowding,
inadequate nutrition and unsuitable medical services.[18-20] However,
the recognition of the magnitude of TB in prison remains a challenge
due to weaknesses of the information system in the penitentiary system.
In a systematic review of the literature, the median incidence rate
ratio for tuberculosis in inmates compared to the general population
was 23.[21] Exposure in prison accounted for a substantial population
attributable fraction of tuberculosis in diverse geographical
settings.[21] It is estimated that up to 25% of a country’s TB burden
may be due to the cases occurring among detainees.[17] Prison inmates
often share narrow spaces with insufficient air circulation which
constitute the ideal conditions for transmission of M. tuberculosis via
airborne droplets. Furthermore, social degradation is often already
present at the time of incarceration, since many prisoners belong to
marginalized groups (e.g. drug addicts, alcohol abusers, homeless
people, migrants) and bear an even higher risk burden in such a
confined environment. Besides the exposure to several risk factors for
infection acquisition and disease progression, the penitentiary system
is often unable to provide adequate TB screening services at first
admission, with delayed application of isolation measures and increased
time-to-treatment. Furthermore, care discontinuation after
release is another relevant issue.[22] In fact, casual and interrupted
treatment significantly contributes to the development and spread of
drug-resistance, creating a TB reservoir which threatens the entire
community through internal personnel, visitors and former inmates.[23]
TB in migrant populations.
Migration is a common and complex phenomenon which has a profound
influence on population dynamics and the global epidemiology of
diseases. Most of the estimated 232 million international migrants,
that currently cross the borders throughout the world annually (plus an
additional 700-800 million internally displaced persons), originate
from low-income countries, where the largest proportion of the global
TB burden concentrates.[24]
Like many other airborne infections,
TB has no boundaries and easily spreads from one region to another,
just following people movements. Migrants represent the major reservoir
of infection in many low endemic countries, where over 50% of TB cases
occur in this particularly fragile group. Significant transmission to
the native population does not seem to be occurring based on current
evidence.[25-27] In low-burden countries TB incidence rates among
migrants can be 10-20 times that of the autochthonous population.[5]
Though usually healthy at first arrival in the destination country,
such individuals are often latently infected with M. tuberculosis.
Their extremely marginalized conditions and major changes in lifestyle,
leading to immune system weakening, favour the progression of the
disease in an active form. Poverty, overcrowded housing,
hazardous working environment, and the existence of concomitant risk
factors (e.g. illicit drug use, alcohol abuse) are all potential
triggers for TB development and spread.[28] Notably, TB incidence rates
among specific migrant communities may differ from what is observed in
their country of origin, being either lower or higher as a result of
determinants associated to the migration process and the hosting
environment. TB re-activation among latently infected subjects more
frequently occurs within the first two years after resettlement,
probably reflecting their greater psycho-social and economic
instability at the beginning of the migratory process.[29,30]
The Threat of Drug-Resistance
Multi-Drug Resistant TB (MDR-TB) is defined as resistance to, at
least, isoniazid and rifampicin among first-line drugs, while
Extensively Drug Resistant TB (XDR-TB) refers to MDR-TB with additional
resistance to, at least, any fluoroquinolone and any one of three
second-line injectable drugs (i.e. capreomycin, kanamycin and amikacin).
MDR-TB
prevalence is estimated from the reported proportion of MDR-TB cases in
countries that either have a routine drug resistance surveillance
system in place or have undertaken a survey and the global TB
prevalence.[31] About 450 000 cases of MDR-TB (range 300 000 – 600 000)
were thought to have emerged in 2012, accounting for 3.6% (2.1-5.1%) of
all new TB cases and 20.2% (13.3-27.2%) of previously treated cases.
The most affected countries are in the Eastern Europe and Central Asia
Region (ECA), and include the Russian Federation, Belarus, Azerbaijan,
Estonia, Kyrgyzstan, Kazakhstan, Republic of Moldova and Uzbekistan (Figure 2).[1]
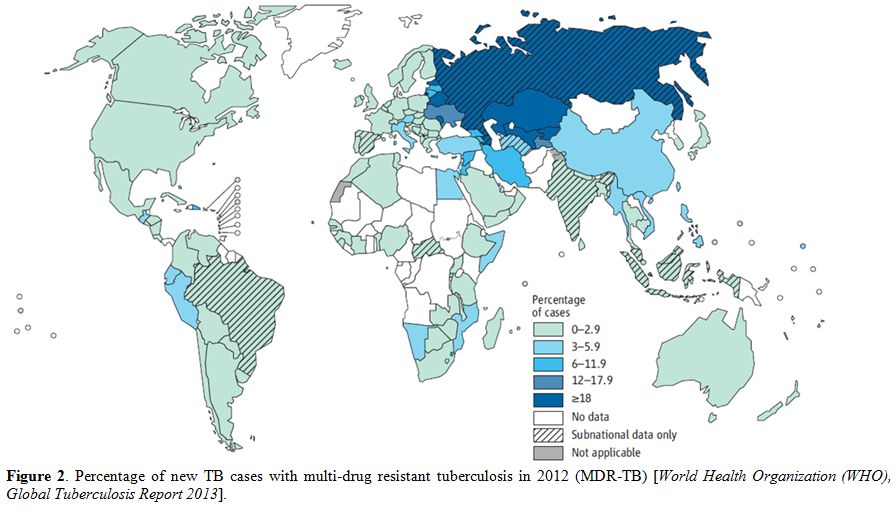 |
Figure 2. Percentage of new TB cases with multi-drug resistant tuberculosis in 2012 (MDR-TB) [World Health Organization (WHO), Global Tuberculosis Report 2013]. |
Furthermore,
XDR-TB, first defined in 2007, has been reported so far by 92 countries
in 2012. Overall, it is estimated that 9.6% of all MDR-TB cases are
XDR-TB.
The response to MDR-TB has been slow in most countries.
Alarmingly, the number of notified MDR-TB cases represents less than
30% of the estimated MDR-TB cases in 2012.[1] This means that the
diagnostic capacity is weak. The implementation of new rapid molecular
diagnostic tests will, hopefully, allow to expand testing capacity in
low-resource settings worldwide and to improve TB case management.
Rapid diagnostic tests such as expert MTB/RIF can be beneficial for
both the individual and the community. A significant reduction of the
time to diagnosis and treatment for infected patients can lead better
outcomes, and so limiting further transmission. In the light of their
potential impact on MDR-TB control, the scale-up of such methods should
be strongly encouraged, in line with the current WHO
recommendations.[32]
With respect to treatment, WHO currently
recommends an 8-month intensive phase and a 20-month minimum overall
treatment duration.[33] Second-line drugs show a less favourable
toxicity profile, higher costs and more limited accessibility than
those included in the standard anti-TB regimen. The report of treatment
outcomes for MDR-TB is challenging, with data available for only 62% of
the MDR-TB cases notified in the 2010 cohort. Of those, only 48%
attained treatment success, which is far from 2015 target of at least
75%.[1] Operational research projects are currently ongoing in many
countries in order to better assess the impact of different second-line
regimens.[34].
TB Control Strategies: Past and Future Steps
After being neglected for two decades, in the early 1990s TB
re-emerged in the global health agenda due to outbreaks in high-income
countries that prompted renewed attention. In 1993, concerned about the
extent of the problem in most of the developing world, WHO declared TB
a global emergency.[35,36] Over the last twenty years global strategies
for TB control have been recommended for adoption and adaptation in all
countries. The first strategy, DOTS, was launched in 1994-1995. It was
based on five key essential components of any sound response to TB:
1) Political commitment with increased and sustained financing;
2) Case detection among people presenting with symptoms in clinics
through quality-assured bacteriology; 3) Standardized and supervised
treatment along with patient support; 4) Effective drug supply and
management system; 5) A standard monitoring and evaluation system
[Framework-WHO, 1994, IUATLD, 1996].[37,38] By adopting this strategy
in as many as 180 countries, approximately 17 million patients were
started on effective treatment by 2003.[39]
The launch of the
first Global Plan to Stop TB 2001-2005 contributed to this achievement
by raising prominently the need to invest both domestically and
internationally. The establishment of the Global Fund in 2002, by
favouring the access to international financing, was an additional
strong factor to strengthen national programmes.[40] As of today, this
mechanism has mobilised about 4.6 billion US$ for TB care and control
in eligible countries.[41]
In view of the need to accelerate
efforts and reach the international targets set in the context of the
MDGs, in 2006 WHO launched an enhanced global strategy referred to as
Stop TB strategy.[42,43] This new approach aimed to ensure universal
access to high-quality health services and patient-centred care for all
individuals with TB, through additional efforts addressing the
challenges emerging in the new century.[44,45] The principles of DOTS
were incorporated as the first component of the 2006 Stop-TB Strategy,
together with five additional components: 1) address TB/HIV, MDR-TB and
the needs of vulnerable populations; 2) contribute to health system
strengthening based on primary health care; 3) engage all care
providers; 4) empower TB patients and encourage community engagement;
5) enable and promote research.[43]
Underpinned by the new Stop TB
Strategy, the second Global Plan to Stop TB covered the period
2006-2015. The scope of this plan was to address the MDG challenge and
pursue the other international targets in order to halve the 1990 TB
prevalence and mortality rate by 2015 and eliminate TB as a public
health problem by 2050 (< 1 case per 1 million population).[46]
Despite all these efforts and the resulting achievements described
above, including the reaching of the TB-relevant target in the MDGs,
global control is progressing slowly, with a decline in incidence of 2%
per year on average. Additional significant challenges remain, such as
multidrug-resistance and the limited advances in the search for new
drugs, diagnostics, and vaccines.
Nevertheless, in view of
recent progress in expansion of proper care and development of new
important tools, more ambitious goals and targets have recently been
approved by the World Health Assembly in its latest session: Tracing
the path towards intensified efforts against TB beyond 2015. The new
post-2015 Global TB Strategy approved by the 67th World Health Assembly
(WHA) in May 2014, aims at “ending the global TB epidemic” by 2035.[47]
This means a 95% mortality reduction and a 90% incidence decline (<
10 TB cases/100 000 population) by 2035 compared to 2015, and the
suppression of any “catastrophic cost” for TB-affected families (Table 1).
The strategy stands on three pillars: (1) promote integrated
patient-centred care and prevention; (2) foster bold policies and
supportive systems; (3) encourage intensified research and innovation (Table 1).
As clearly stated in the ten-component list that constitutes the
backbone of the post-2015 agenda, a special attention is devoted to the
most vulnerable populations (such as migrants, refugees and TB/HIV
co-infected patients) and great emphasis is also placed on the need to
improve diagnostic and therapeutic capacities through a strong
political commitment and intensified investment in research. Crucially,
the new strategy recognises fully the need for bold policies that go
beyond those of national programmes and engage the entire health
system, such as rationalising the use of medicines, ensuring their
quality, establishing infection control measures etc. In addition, the
new strategy calls upon the institution of universal health coverage
and social protection schemes that facilitate access to care by poor
people with TB while preventing catastrophic expenditures due to their
ill health. Finally, the new strategy emphasises that action on social
and economic, “upstream” determinants of TB must be addressed if the
world truly envisages the elimination of this disease in the decades to
come. Four principles underpin the three pillars: government
stewardship and accountability; strong coalition with the civil society
and communities; protecting and promoting human rights, ethics and
equity; and adaptation of the strategy and targets at country level
with global collaboration. In fact, since TB transmission is mainly
airborne, and a large submerged reservoir of infection currently exists
in the community, global elimination will only be achieved through
elimination from every country, which requires international support.
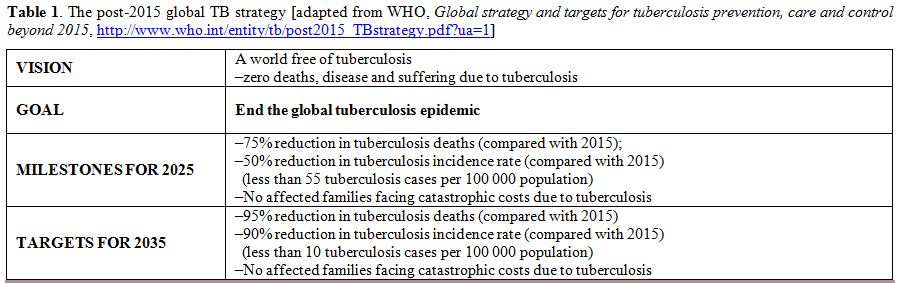 |
Table 1. The post-2015 global TB strategy [adapted from WHO, Global strategy and targets for tuberculosis prevention, care and control beyond 2015, http://www.who.int/entity/tb/post2015_TBstrategy.pdf?ua=1] |
The
strategy is also designed to face the challenges of low-burden
countries (namely, those with an incidence below 10/100 000/year). In
these countries TB tends to concentrate in selected marginalized groups
with limited transmission rates within the general population and with
most TB cases resulting from reactivation of latent TB infection
(LTBI). In an effort to adapt the new strategy to their settings, the
33 countries, that currently can be considered as low-incidence
recently, met in Rome for a Global Consultation, convened by WHO and
the European Respiratory Society. The topic of their discussions was
the common challenges so that they can engage a concerted action to
implement the new strategic directives.
Among priorities in
these countries, but also world-wide, a crucial importance was
attributed to the introduction and the routine application of new
technologies for rapid detection of drug-resistance and particularly
useful for high-risk patients.[48]
After over 40 years from the
development of rifampicin in the 60s, two new anti-tuberculosis drugs
were registered in 2012 and 2013. Bedaquiline was approved by the US
Food and Drug Administration (FDA) at the end of 2012 and is currently
recommended by WHO for the treatment of selected MDR-TB cases.[49] A
year later, Delamanid received the approval from the European Medical
Agency (EMA) and Bedaquiline is currently available for use in MDR-TB
treatment in Europe.[50] Currentely, the pharmaceutical industry has
little interests in investing on research and manufacturing new
anti-tubercular molecules that at present are considered
orphan drugs. A cautious choice of patients and close monitoring during
and after treatment are, therefore, essential to preserving their
efficacy.
References

[TOP]