Insulin-like Growth Factor-1 (IGF-1): Demographic, Clinical and
Laboratory Data in 120 Consecutive Adult Patients with Thalassaemia
Major
Vincenzo De Sanctis1, Ashraf T Soliman2, Giancarlo Candini3, Mohamed Yassin4, Giuseppe Raiola5, Maria Concetta Galati6, Rania Elalaily7, Heba Elsedfy8, Nicos Skordis9, Piernicola Garofalo10, Salvatore Anastasi11 , Saveria Campisi12 , Mehran Karimi13, Christos Kattamis14, Duran Canatan15, Yurdanur Kilinc16, Praveen Sobti17, Bernadette Fiscina18 and Mohamed El Kholy8
1 Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, Ferrara, Italy
2 Department of Pediatrics, Division of Endocrinology, Hamad General Hospital Doha, Qatar
3 Department of Medical Physics, St. Anna Hospital, Ferrara, Italy
4 Department of Hematology, Alamal Hospital, Hamad Medical Center, Doha, Qatar
5 Department of Paediatrics, Pugliese-Ciaccio Hospital, Catanzaro, Italy
6 Department of Haematology, Thalassaemia and Prenatal Diagnosis Regional Center, Pugliese-Ciaccio Hospital, Catanzaro, Italy
7 Department of Primary Health Care (PHC), Doha, Qatar
8 Department of Pediatrics, Ain Shams University, Cairo, Egypt
9 St. George’s University Medical School at the University of Nicosia, Cyprus
10 Endocrine Unit, Villa Sofia –Cervello Hospital, Palermo, Italy
11 Department of Thalassaemia, Garibaldi Hospital, Catania, Italy
12 Unit for the Diagnosis and Treatment of Thalassaemia, Umberto I Hospital, Siracusa, Italy
13 Hematology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
14 First Department of Paediatrics, University of Athens, Athens, Greece
15 Director of Hemoglobinopathy Diagnosis Center and President of Mediterranean Blood Diseases Foundation, Antalya, Turkey
16 Department of Pediatric Hematology, Faculty of Medicine, University of Çukurova, Adana, Turkey
17 Professor of Pediatrics, Christian Medical College and Hospital, Ludhiana, India
18 Department of Pediatrics, NYU School of Medicine, New York, USA
Corresponding author: Vincenzo De Sanctis MD,
Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, 44100
Ferrara, Italy; Tel: 39 0532 770243; E-mail:
vdesanctis@libero.it
Published: November 01, 2014
Received: August 10, 2014
Accepted: October 18, 2014
Meditter J Hematol Infect Dis 2014, 6(1): e2014074, DOI
10.4084/MJHID.2014.074
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Introduction: IGF-1
deficiency in TM patients in children and adolescents has been attributed to
chronic anemia and hypoxia, chronic liver disease, iron overload and other
associated endocrinopathies, e.g. growth hormone deficiency (GHD). Few data are
available in the literature regarding adult TM patients and growth disorders.
The aim of this study was to measure IGF-1 values and other clinical data in a
large number of adult patients with TM to evaluate the possible relationships
between them.
Patients and Methods: A cohort
of 120 adult patients with TM was studied for plasma levels of
IGF-1. Plasma total IGF-1 was determined by chemiluminescent immunometric assay
(CLIA) method. In eleven patients (3 females) the GH response
during glucagon stimulation test (GST) was also evaluated.
Results: Fifty
percent of patients (33 males and 27 females) had IGF-1 levels <- 2 SDs
below normative values for healthy subjects matched for age and sex. In these
patients endocrine complications and elevations of
aminotransferases (ALT) were more common compared to TM patients
with IGF1 > -2SDs. In multivariate regression analyses, height, weight, BMI,
serum ferritin, ALT, HCV serology and left ventricular ejection fraction (LVEF)
were not significantly related to IGF-1, but a significant correlation was
found in females between HCV-RNA positivity and IGF-1, ALT and serum ferritin.
AGHD was
diagnosed in 6 (4 males) out of 11 patients (54.5%) who had glucagon
stimulation tests and in 5 out of 8 (62.5%) with IGF-1 <-2SD. The mean age
of patients with GHD was 39.3 years (range: 25-49 years, median: 39 years)
versus 35.8 years (range: 27-45 years, median: 37.5 years) in non-GHD patients.
A positive correlation between GH peak after GST and IGF-1 level was found (r: 0.6409; p: < 0.05).
:Conclusions: In 50%
of TM patients the IGF-1 levels were 2SDs below average values for healthy
individuals. IGF-1 deficiency was more common in TM patients with associated
endocrine complications, and a significant correlation was found in HCV-RNA
positive females among IGF-1, ALT, and serum ferritin. Further data in a larger
group of patients are needed to confirm whether IGF-1 level <-2
SDs may be a potential criterion for additional studies in TM patients. This
datum could avoid performing GH stimulation tests in the majority of them.
|
Introduction
IGF-1 is a small peptide (molecular weight 7649 Da), that circulates
in serum bound to high affinity binding proteins (IGFBPs), mostly in a
ternary complex with IGF-binding protein 3 (IGFBP-3) and acid-labile
subunit (ALS). This ternary complex is a storage form of IGF-1 in serum
and has a half-life of several hours. ALS is synthesized under direct
control of GH, primarily in hepatocytes. In contrast to pulsatile GH
secretion, circulating IGF-1 and IGFBP-3 are stable and reflect the
long-term status of GH secretion.[1,2]
Although the liver mainly produces IGF-1, every tissue can secrete IGF-1 for autocrine and paracrine purposes.[3]
IGF-1 possesses a large number of activities (anabolic,
antioxidant, anti-inflammatory and cytoprotective actions), however, it
is partly responsible for systemic GH actions.[4]
IGF-1 deficiency in TM patients in children and adolescents has been
attributed to chronic anemia and hypoxia, chronic liver disease, iron
overload and other associated endocrinopathies, e.g. growth hormone
deficiency (GHD).[5-11]
Few data are available in
the literature regarding adult TM patients. Therefore, the
International Network of Clinicians for Endocrinopathies in Thalassemia
and Adolescence Medicine (ICET-A), previously called the International
Network on Endocrine Complications in Thalassemia (I-CET), for a better
interpretation of IGF-1 values in thalassaemia made the following
proposals:
(1) estimate the IGF-1 values in a large number of
adult TM patients; (2) conduct the study in a single center, to
minimize the considerable variation in the assay methods used; (3)
compare the results with those for a reference population of healthy
adults; (4) correlate the IGF-1 values of patients with TM with other
clinical and laboratory parameters; (5) perform a provocative GH
stimulation test with glucagon (GST) in a small group of TM subjects
with normal or low IGF -1 levels (below the mean standard reference
levels); (6) to review the current literature on AGHD in thalassaemia
with the final goal of assisting clinicians in the management of TM
patients with GH-IGF-1 axis related disorders.
Subjects and methods
From 2009 to 2013, we studied 120
consecutive adult patients with TM followed at our institution Patients
with thalassaemia intermedia, cirrhosis, cardiac and renal failure and
HIV positivity were excluded from the study.
An extensive medical
history, including data on associated complications and current
medications, was obtained, and a physical examination (pubertal status,
weight, and height) for each patient was performed. Body mass index
(BMI) was calculated as the body weight divided by the height squared
(Kg/m2). A subject was considered overweight when the BMI was between 25 and 29.9 and obese when the BMI was 30 or higher.
All
patients were on regular transfusions (mean haemoglobin level 11.5
g/dl) and iron chelation therapy with deferoxamine (64 patients: 30-45
mg/kg body weight, 4-6 days a week by slow subcutaneous infusion by
pump, starting in 1977-1978), or oral deferiprone (22 patients: 75
mg/kg body weight daily), or deferiprone plus deferoxamine (25
patients; 75 mg/kg body weight daily and 40 mg/kg body weight, 3 days a
week, by slow subcutaneous pump infusion) or oral deferasirox (9
patients: 20-30 mg/kg body weight daily).
The following clinical
and laboratory data were also recorded: age at first transfusion, age
at start of regular chelation therapy, duration of iron chelation
therapy, compliance with treatment and the presence of associated
growth and endocrine complications, as previously described.[12]
The
compliance was arbitrarily considered as good when the chelation
therapy was given 5-6 days a week, moderate four days a week and poor
less than three days a week.
Blood samples were drawn in the
morning after an overnight fast and at least 2-3 weeks after the last
blood transfusion to measure the serum concentrations of IGF-1, free
thyroxine (FT4) and thyrotropin (TSH), urea, creatinine, electrolytes,
glucose, calcium, phosphate and serum ferritin. As routine or to
exclude severe liver pathology or decreased synthetic functions,
alanine aminotransferase (ALT), gamma glutamyl transferase (γGT),
alkaline phosphatase (ALP), total and direct bilirubin, albumin,
prothrombin time (PT) and international normalization ratio (INR), and
serologic screening assays for hepatitis C virus seropositivity (HCVab
and HCV-RNA ) were also evaluated.
Iron overload was assessed at
the beginning of the study, by serum ferritin level. It was arbitrarily
categorized as mild, moderate or severe if the levels were <1000
ng/ml, from 1000 to 2000 ng/ml and >2000 ng/ml, respectively.[13]
In
eleven patients (3 females) the GH response, after glucagon stimulation
test (GST), was evaluated. Blood samples were collected for 3 hours (at
baseline, 30, 60, 90, 120, 150 and 180 minutes), because, according to
the literature, the majority of GH peaks occur between 120 and
180 minutes (85%). Serum glucose, insulin and GH were measured; a GH
peak below three μg/L was defined as severe GHD, according to Gomez et
al.[14]
For ethical reasons we used as a
reference for normal the IGF-1 values determined in a large population
of healthy subjects, reported in the literature[12]
using the same automated chemiluminescence immunoassay system (CLIA). A
serum IGF-1 level below -2 SD was considered as deficiency.
Insulin
resistance was also calculated in these patients using HOMA-IR
(homeostasis model assessment method). Considering HOMA-IR values, the
studied population was defined as a. (insulin sensitive) HOMA-IR <
2.24; b. (intermediate) 2.24 - ≤ 3.59; c. (insulin resistant) HOMA-IR
> 3.59.[16]
Biochemical, Hormonal and Cardiac Assessment:
Fasting blood samples for circulating IGF-1 were collected and stored
at −60°C until centrally assayed. Plasma total IGF-1 was determined on
EDTA by chemiluminescent immunometric assay (CLIA) method (Nichols
Institute Diagnostics, San Juan, CA). The assay was performed after
separation of IGF-1 from binding proteins by Liaison® autoanalyser
(DiaSorin SpA, Saluggia, Italy). The sensitivity of the test was six
ng/ml, whereas the intra- and inter-assay coefficients of variation
(CVs) of our in-house pooled serum control sample were 4.8% and 7.1%,
respectively.
Serum GH concentrations were measured in duplicate
at each time point with commercial solid-phase two-site
chemiluminescent immunoassay. The inter- and intra-assay CVs were below
7%.
TSH and FT4 were assessed with an electro-chemoluminescence
(ECLIA) assay with a normal range of 0.8-1.8 ng/dL for FT4 and 0.5-4.6
mIU/l for TSH. The minimal detectable levels of FT4 and TSH were 0.2
ng/dL, and 0.1 mIU/L, respectively. The inter-assay and intra-assay
coefficients of variation of FT4 varied from 5.8% to 6.26%, and from
2.6% to 2.9%, respectively, and those of TSH were from 5.1% to 5.7%,
and from 2.2% to 2.9%, respectively.
All biochemical and serologic
tests were carried out in accordance with the routine procedures of the
central laboratory. Serum ferritin was measured by
electrochemiluminescence immunoassay. Reference range values were
30-350 μg/l in males and 15-150 μg/l in females.
Left ventricular
ejection fraction (LVEF, %) was measured according to the
recommendation of the American Society of Echocardiography, using
freeze-frames from two-dimensional directed M-mode echocardiogram.[17]
Associated endocrine complications were defined according to the I-CET position statement published in 2013.[12]
Ethical Aspects:
The study was made in accordance with the provisions of the Declaration
of Helsinki. The prospective study was started at the beginning of 2009
by the Coordinator of I-CET (VDS) at the Thalassaemia Centre of
Ferrara, and was completed at the end of 2013 at the Quisisana
Pediatric and Adolescent Outpatient Clinic of Ferrara. All of the
subjects gave their consent to participate in the study.
Statistical Analysis:
Characteristics of the studied patients are reported as mean ± standard
deviation (SD), median, number and range. Quantitative variables are
reported as medians (range or percentiles) or mean (SD).
Statistical
significance of the differences between variables was assessed using
the unpaired two-tailed Student’s t test or Wilcoxon test using a
software package program. The frequency distributions for age and sex
were analyzed using the chi-square test while the multiple regression
analysis was conducted using the multiple linear fitting with least
squares method.
The distribution analysis of IGF1 values in males
and females groups was performed including the following parameters:
mean and SD, median, range, kurtosis, skewness, and percentiles.
Fisher's Exact test was used to calculate the probability value for the relationship between two dichotomous variables.
A p value < 0.05 was considered as significant.
A
software program used for the statistical analysis was developed by Dr.
Candini (Department of Medical Physics, St. Anna Hospital, Ferrara,
Italy) and validated according to Alder and Roesser.[18]
Results
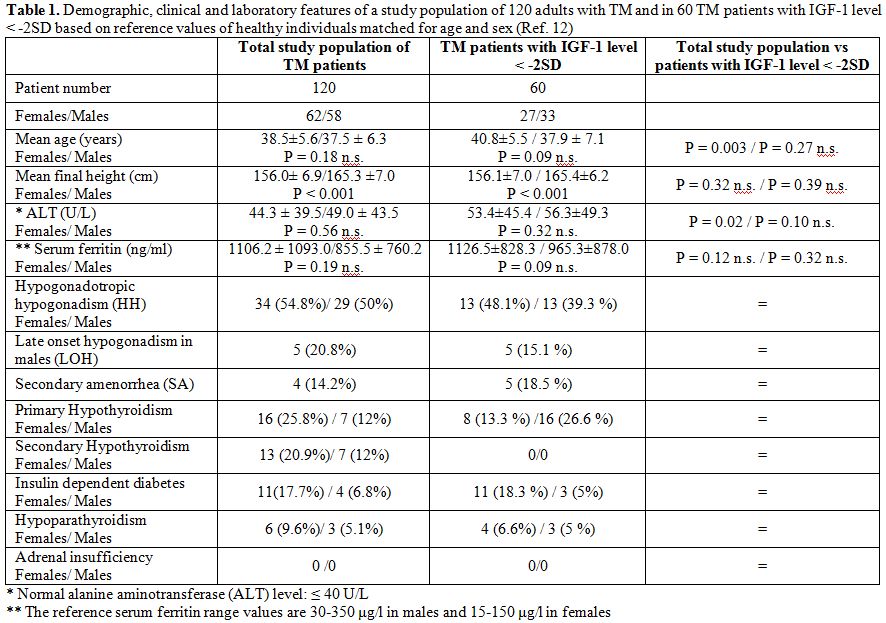
The demographic, clinical, and laboratory data of the TM study population are presented in Table 1. Rates of infection with hepatitis C are displayed in Table 2.
|
|
Table 1. Demographic, clinical and laboratory
features of a study population of 120 adults with TM and in 60 TM
patients with IGF-1 level < -2SD based on reference values of
healthy individuals matched for age and sex (Ref. 12) |
|
|
Table 2. Prevalence of thalassaemia major patients infected with HCV enrolled in the study |
A statistical comparison between HCV positive and negative
TM patients was not done because only 3 TM patients were HCV negative (Table 2).
In addition, using a multivariate discriminant analysis the
classification error observed between HCV positive and negative
patients was 20% and therefore was considered not clinically acceptable.
An
abnormal ALT value (>40 U/L) was observed in 51.8% of female TM
patients with IGF-1 levels < -2SD and 23 % of patients with IGF-1
levels > -2SD. Similar results were observed in males (48.4% with
IGF-1 levels < -2SD and 26.6% IGF-1 levels > -2SD).
Of the
120 patients, 58 (48%) were males and 62 (52%) females, with an age
range of 26.0 - 53.2 (median 38) years for females and 20.8 - 51.2
years for males (median 37.05), 64.4 % of the patients were above 35
years of age. The mean body mass index (BMI) was 22.48 ± 3.34 kg/m2.
The
mean value of BMI in TM female patients with IGF 1 <-2SD was 23.8 ±
4.3 (range: 18.6 - 40) and in patients with IGF 1 > -2SD was 23.2 ±
3.5 (range: 17.2 – 32.2. The mean value of BMI in TM male patients with
IGF 1 <-2SD was 22.3 ± 2.7 (range: 17.4 – 28) and in patients with
IGF 1 > -2SD was 22.1 ± 1.7 (range: 18.5 – 23.2).
Seven TM
female patients were classified as overweight and three as obese; 5 TM
male patients were classified as overweight and none as obese.
Of 63 patients with hypogonadism, 13 (37%) were on stable sex steroid therapy (Table 1).
All patients with primary or central hypothyroidism or
hypoparathyroidism were receiving levothyroxine or calcium and
calcitriol. The type 1 diabetic patients were treated with insulin.
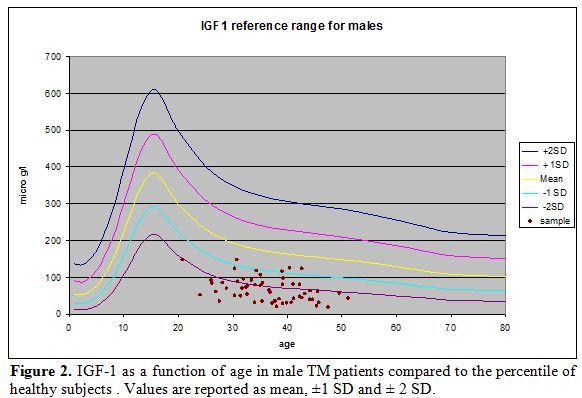
In
males with TM, the serum concentrations of IGF-1 ranged between 18.3
and 147.7 ng/ml (mean 68.29 ± 33.5 ng/ml; median 62.5 ng/ml; kurtosis
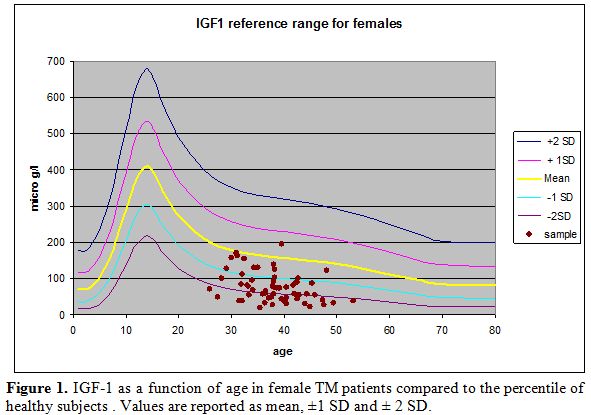
-0.5, skewness 0.57); whereas, in females with TM, IGF-1 ranged between
19.5 and 195.5 ng/ml (mean 76.46 ± 41.84 ng/ml; median 69.05 ng/ml;
kurtosis 0.02; skewness 0.87).
The distribution of IGF-1 values in the two groups of TM patients compared to the percentiles of Brabant et. al[15] are reported in Figures 1 and 2.
|
|
Figure 1. IGF-1 as a function of age in female TM
patients compared to the percentile of healthy subjects . Values are
reported as mean, ±1 SD and ± 2 SD. |
|
|
Figure 2. IGF-1 as a function of age in male TM
patients compared to the percentile of healthy subjects . Values are
reported as mean, ±1 SD and ± 2 SD.
|
No significant differences were observed between IGF-1
values in men and women with TM (t-test: 1.18; p: 0.249). In
multivariate regression analyses, height, weight, BMI, serum ferritin,
ALT, HCV serology and left ventricular ejection fraction (LVEF) had no
significant relationship with IGF-1 levels, but a significant multiple
correlation was found in females, with HCV-RNA positivity, between
IGF-1, ALT and serum ferritin (r= 0.504 , p= 0.043). The simple
correlation matrix was as follows: IGF1 vs ALT: r = 0.505 p < 0.05;
IGF1 vs serum ferritin: r = - 0.466 p < 0.05; ALT vs serum ferritin:
r = - 0.402 p < 0.05.
A statistical comparison of IGF 1 values
between HCV positive and negative TM patients was not done because only
three patients were HCV negative (Table 2).
In addition, using a multivariate discriminant analysis the
classification error between patients HCV positive and negative
patients was 20% and therefore considered not statistically acceptable.
Analysis
of individual IGF-1 levels in TM patients showed that IGF-1 levels were
below -2SDs of normal values for healthy individuals[15] in 60 (50 %) patients (33 males and 27 females).
The demographic, clinical and laboratory features of the TM patients with IGF-1 levels < -2SD below normal are reported in Table 1.
A
comparison of clinical and laboratory features of male and female TM
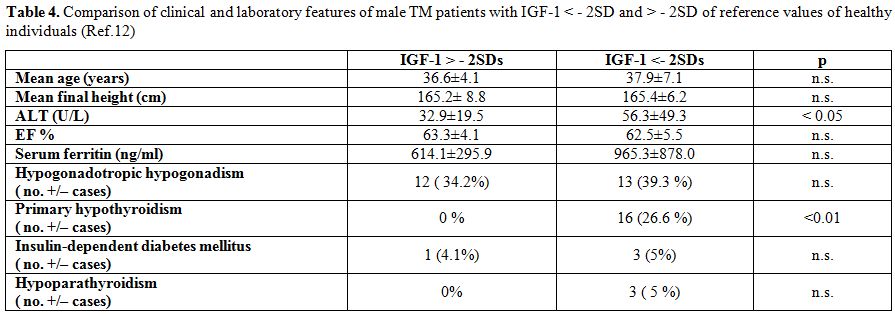
patients with IGF-1 < - 2SD and > - 2SD are reported in Tables 3 and 4.
|
|
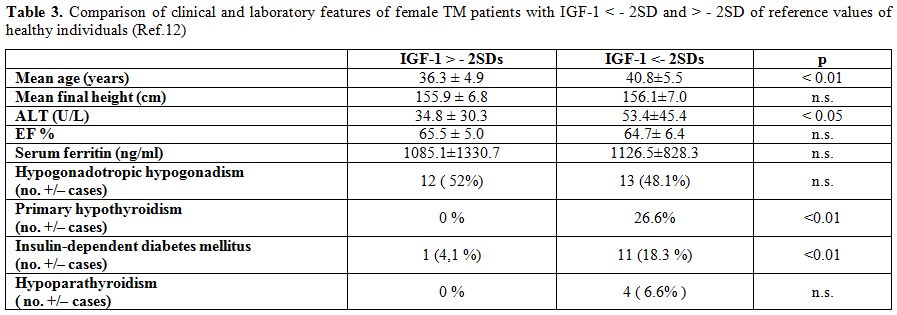
Table 3. Comparison of clinical and laboratory features
of female TM patients with IGF-1 < - 2SD and > - 2SD of reference
values of healthy individuals (Ref.12) |
|
|
Table 4. Comparison of clinical and laboratory features
of male TM patients with IGF-1 < - 2SD and > - 2SD of reference
values of healthy individuals (Ref.12) |
There were significant differences in age, ALT levels, and
rates of primary hypothyroidism and insulin-dependent diabetes between
female patients with IGF-1 levels <2 SD and those with higher IGF-1
levels; significant differences only for ALT levels and rates of
primary hypothyroidism were found in males with IGF-1 <2 SD.
The left ventricular ejection fraction (LVEF) was reduced (< 50%) in 2 patients (1.6%).
AGHD
was diagnosed in 6 (4 males) out of 11 patients who had glucagon
stimulation tests (54.5 %). The mean age of patients with GHD was 39.3
years (range: 25-49 years) versus 35.8 years (range: 27-45 years) of
non-GHD patients.
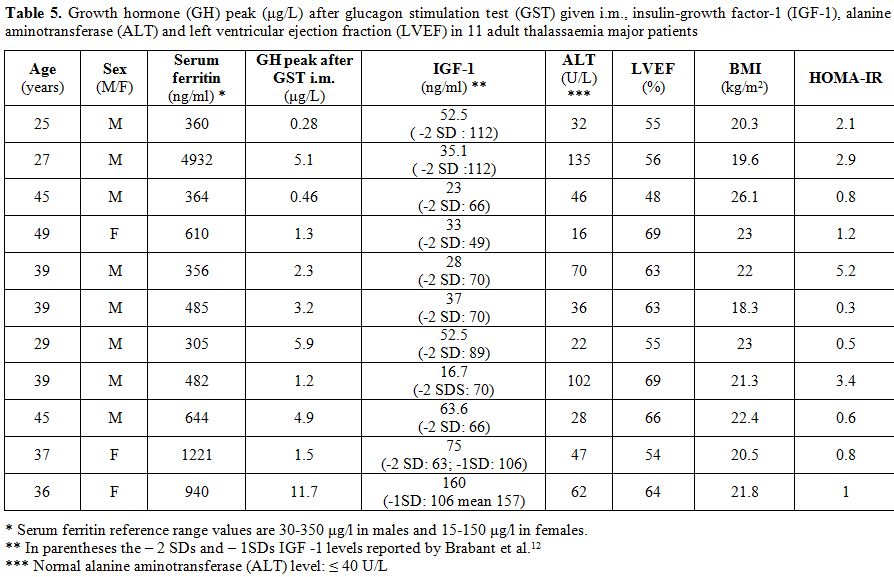
A positive correlation between GH peak after GST
and IGF-1 levels was found (r =0.6409; p: < 0.05). In particular, a
low GH peak after GST (range 0.28-1.3 ng/ ml) was found in 5 out of 8
patients (aged 25-49 years) with an IGF-1 level below -2SDs (range 16.7
– 52.5 ng/ml) and in 1 out of 2 patients with an IGF-1 level below -1SD
(75 ng/ml) (Table 5). No correlation was observed between IGF-1 level, ALT and LVEF.
A HOMA-IR > 3.59 was found in one female TM patient with GHD (Table 5).
In
general, in our patients the compliance to treatment was good or
satisfactory. A serum ferritin level below 1000 ng/ml was observed in
36 (65.5%) female and 37 (74%) male TM patients. A ferritin level >
2000 ng/ml was observed in 11 (20%) female and 5 (10%) male patients.
The remaining patients had a serum ferritin level between 1000 to 2000
ng/ml [11 females (20%) and 8 (16%) males]. However, we did not know
with absolute certainty if the patients in the past had a severe iron
overload.
|
|
Table 5. Growth hormone (GH) peak (μg/L) after glucagon
stimulation test (GST) given i.m., insulin-growth factor-1 (IGF-1),
alanine aminotransferase (ALT) and left ventricular ejection fraction
(LVEF) in 11 adult thalassaemia major patients. |
Discussion
In
healthy individuals, serum levels of IGF-1 peak at puberty (mean level:
391 ng/ml, between the ages of 14-15 years) and decline with age (mean
level: 174 ng/ml at the age of 35 years and 99 ng/ml at the age of 70
years).[15]GH
is the most important factor controlling IGF-1 secretion and
concentration. Other factors are also determinant: age, sex, pubertal
stage, ethnicity, nutritional function, hepatic status and hormones
(sex steroids, thyroxin, and prolactin).[19-22]Very low levels of IGF-1 were found in our adult patients with TM with or without GH deficiency (GHD).[22-24] Of 120 TM patients, 50 % (33 males and 27 females) had IGF-1 levels 2SDs below average values for healthy individuals.[15]A
marked IGF-1 deficiency (IGF1 < -2SD) was more common in TM patients
with associated endocrine complications, and multiple significant
direct correlations were found in females, with HCV-RNA positivity,
among IGF-1, ALT and serum ferritin. There is increasing evidence that between 8% to 44% of adult patients with TM develop some degree of GHD.[36-40]
On GST, GHD was found in 6 out of 11 TM patients studied (54.5%), aged
25-49 years. Of those with GHD, five had IGF < -2SD However, the
number of patients was too small to perform a statistical correlation.
Similar results were obtained by Soliman et al.[29]
The authors diagnosed IGF-1 deficiency (IGF-1 <-2 SDs) in 20
patients out of 30 (66.6 %). Twelve out of 30 TM patients (40%) had
GHD.[41] Peak GH levels correlated significantly with
IGF-1 levels and the height of TM patients expressed in SDS. Neither GH
peak nor IGF-1 concentrations were correlated to serum ferritin and
liver enzymes.[29] TM patients with GHD and IGF-1
deficiency also had a significantly lower bone mineral density (BMD)
T-score at the lumbar spine compared to patients with normal GH and
IGF-1 levels.[29] These data confirm the role of
IGF-1 in the pathophysiology of osteoporosis in addition to prenatal
and postnatal body growth.[30-37]An
abnormal ALT value (>40 U/L) was observed in 51.8% of our female TM
patients with IGF-1 levels < -2SD and 23% of patients with IGF-1
levels > -2SD. Similar results were observed in males (48.4% of TM
patients with IGF-1 levels < -2SD and 26.6% of patients with IGF-1
levels > -2SD. Both differences in rates were statistically
significant.In
addition to GHD and chronic liver disease, IGF-1 deficiency in patients
with TM may be partly due to anemia, iron overload, hypogonadotropic
hypogonadism (HH) or its treatment, vitamin D or zinc deficiency.Soliman
et al. have demonstrated the beneficial effect of correcting anemia on
increasing serum levels of IGF-1 in children with TM.[24,38]
Similarly, correction of other forms of anemia and correction of
hypoxia by surgical repair of congenital cyanotic heart lesions have
been previously shown to improve IGF-1 secretion, as well as subsequent
growth.[39-41] In the study by Soliman et al.,
however, the TM patients were severely anaemic (7.5 ±1.2 g/dl) before
blood transfusion. The increase of mean Hb from 7.5 ± 1.2 g/dl to 9.2 ±
0.8 g/dl was associated with a significant increase in circulating
IGF-1 from 53 ± 35 ng/ml to 82.6 ± 39 ng/ml.[24,38]All
our TM patients were receiving regular blood transfusions and their
mean Hb level was 11.5 g/dl (mean of pre and post-transfusion Hb).
Therefore, it is possible that Hb was not a causative factor for the
reduced IGF-1 levels found in our patients.In
general, the compliance to chelation treatment was considered good or
satisfactory in our patients. A serum ferritin level below 1000 ng/ml
was observed in 36 (65.5%) female TM patients and 37 (74%) male
patients. However, we did not know with absolute certainty if the
patients in the past had severe iron overload.Seventy-two of our patients (60%) had hypogonadotropic hypogonadism (HH), late-onset
hypogonadism (LOH) or secondary amenorrhea (SA); 43 patients had
primary or central hypothyroidism (35.8 %); 9 patients (7.5%) had
hypoparathyroidism and 15 patients (12.5 %) had insulin-dependent
diabetes mellitus. Only one-third (37%) of patients with HH were on sex
steroid replacement therapy, but the duration of treatment was variable
from patient to patient. Therefore, a statistical analysis between
treated, untreated and undertreated TM patients with hypogonadism was
not done.It
is well known that oestradiol inhibits IGF1 synthesis in the liver by
inducing suppressor of cytokine signalling 3 (SOCS3), which inhibits GH
stimulated signal transduction.[42] On the other
hand, testosterone (T) not only enhances hepatic IGF1 synthesis, but
also alters the sensitivity of the pituitary gland to negative-feedback
regulation of GH secretion, leading to an increase of GH and IGF-1
levels.[43]Recently,
it has been shown that vitamin D increases circulating IGF1 in adults
and serum IGF-1 levels are significantly correlated with serum zinc.[44,45]
Unfortunately, zinc and vitamin D levels were not assessed because, in
the original protocol, prepared in 1998, these variables were not
included.Another well recognised effect of low IGF-1 is the increased risk for developing insulin resistance in humans.[46] IGF-1 improves insulin resistance both in type 2 diabetes and subjects with more severe insulin resistance. HOMA–IR
was assessed in only eleven patients (all of them had an IGF 1 level
< - 1 or -2 SDs) studied for GH response to glucagon stimulation
test. None of them had insulin resistance.Further studies, however, are needed in patients with TM because the prevalence of diabetes varies from 6.4% to 14.1%[47] and both insulin resistance and decreased insulin secretion contribute to the development of DM.[47,48]In
conclusion, although many efforts have been made to explore and define
the management of TM patients from the endocrinological standpoint,
some important questions still remain. An
IGF-1 level <-2 SDs may be a potential criterion for screening of TM
patients for GHD, to avoid performing GH stimulation tests in the
majority of them. Nevertheless, further data in a larger group of
patients are needed to confirm this finding.The
dysfunction of the GH-IGF-1 axis has significant clinical implications,
considering that GHD might contribute to the decline of several tissue
functions. IGF-1 is a key peptide involved in cell growth and protein
turnover, acting as the primary mediator of many of the responses
regulated by GH in tissues.We
believe that the role of liver iron overload in IGF-1 deficiency should
be further evaluated by MRI assessment of liver iron concentration
(LIC) and not with serum ferritin levels. In addition, the role of
chronic active hepatitis C and liver function impairment necessitates
more extensive studies.Finally,
given the high prevalence of hormonal deficiencies and the
non-specificity of clinical signs and symptoms, a systematic annual
endocrine referral is recommended in TM patients. It is advisable to
define multidisciplinary cost-effective protocols in which first-line
specialists order baseline pituitary function tests and
endocrinologists do the clinical evaluation, interpret the hormonal
results and evaluate the possible related complications. References
- Laron Z. Insulin-like growth factor 1 (IGF-1): a growth hormone.Mol Pathol. Oct 2001;54: 311–6. http://dx.doi.org/10.1136/mp.54.5.311 PMid:11577173 PMCid:PMC1187088

- Jones
JI, Clemmons DR. Insulin-like growth factors and their binding
proteins: biological actions. Endocrine Rev 1995;16:3-34. PMid:7758431
- D'Ercole
AJ, Applewhite GT, Underwood LE. Evidence that somatomedin is
synthesized by multiple tissues in the fetus. Dev Biol 1980; 75:315–28.
http://dx.doi.org/10.1016/0012-1606(80)90166-9
- Bach
LA. The nsulin-like growth factor system: towards clinical
applications. Clin Biochem Rev 2004:25: 155-64 PMid:18458708
PMCid:PMC1880833
- Soliman
AT, El Zalabany MM, Amer M, Ansari BM. Growth and pubertal development
in transfusion-dependent children and adolescents with thalassaemia
major and sickle cell disease: a comparative study. J Trop Pediatr
1999;45:23-30 http://dx.doi.org/10.1093/tropej/45.1.23 PMid:10191589
- N,
Kyriakou A. The multifactorial origin of growth failure in
thalassaemia. Pediatr Endocrinol Rev. 2011;8 (Suppl 2) :271-7.
PMid:21705977
- Low LC.Growth, puberty and endocrine function in beta-thalassaemia major. J Pediatr Endocrinol Metab. 1997;10:175-84 http://dx.doi.org/10.1515/JPEM.1997.10.2.175 PMid:9364350
- De
Sanctis V, Eleftheriou A, Malaventura C. Prevalence of endocrine
complications and short stature in patients with thalassemia major: a
multicenter study by the Thalassemia International Federation. Pediatr
Endocrinol Rev 2004;2(Suppl 2):249-55. PMid:16462705
- Shehadeh
N, Hazani A, Rudolf MC, Peleg I, Benderly A, Hochberg Z. Neurosecretory
dysfunction of growth hormone secretion in thalassemia major. Acta
Paediatr Scand 1990;79:790-95 http://dx.doi.org/10.1111/j.1651-2227.1990.tb11556.x PMid:2239274
- Soliman
AT, El Zalabany MM, Mazloum Y,Bedair SM, Ragab MS, Rogol AD, Ansari BM.
Spontaneous and provoked growth hormone (GH) secretion and insulin-like
growth factor I (IGF-I) concentration in patients with beta
thalassaemia and delayed growth. J Trop Pediatr 1999;45:327-37. http://dx.doi.org/10.1093/tropej/45.6.327 PMid:10667001
- De
Sanctis V, Skordis N, Galati MC, Raiola G, Giovannini M,Candini G,
Kaffe K, Savvides I, Christou S. Growth hormone and adrenal response to
intramuscular glucagon test and its relationship to IGF-1 production
and left ventricular ejection fraction in adult B-thalassemia major
patients. Pediatr Endocrinol Rev 2011; 8 Suppl 2:S290-4.
- De
Sanctis V, Soliman AT, Elsedfy H, Skordis N, Kattamis C, Angastiniotis
M, Karimi M, Yassin MA, El Awwa A, Stoeva I, Raiola G, Galati MC,
Bedair EM, Fiscina B, El Kholy M. Growth and endocrine disorders in
thalassemia: The international network on endocrine complications in
thalassemia (I-CET) position statement and guidelines. Indian J
Endocrinol Metab. 2013;17:8-18 http://dx.doi.org/10.4103/2230-8210.107808 PMid:23776848 PMCid:PMC3659911
- De
Sanctis V, Soliman A, Candini G, Campisi S, Anastasi S, Yassin M. High
prevalence of central hypothyroidism in adult patients with
ß-thalassemia major. Georgian Med News. 2013;222:88-94. PMid:24099820
- Gomez
JM, Espadero RM, Escobar-Jimenez F, Hawkins F, Pico A, Herrera-Pombo
JC, Vilardell E, Duran A, Mesa J, Faure E, Sanmarti A. Growth hormone
release after glucagon as a reliable test of growth hormone assessment
in adults. Clin Endocrinol 2002;56:329-34 http://dx.doi.org/10.1046/j.1365-2265.2002.01472.x
- Brabant
G, von zur Mühlen A, Wüster C, Ranke MB, Kratzsch J, Kiess W,
Ketelslegers JM, Wilhelmsen L, Hulthén L, Saller B, Mattsson A, Wilde
J, Schemer R, Kann P: German KIMS Board. Serum insulin-like growth
factor I reference values for an automated chemiluminescence
immunoassay system: results from a multicenter study. Horm Res.
2003;60:53-60. http://dx.doi.org/10.1159/000071871 PMid:12876414
- Matthews
DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC:
Homeostasis model assessment: insulin resistance and beta-cell function
from fasting plasma glucose and insulin concentrations in man.
Diabetologia 1985; 28:412–9 http://dx.doi.org/10.1007/BF00280883 PMid:3899825
- Sahn
DJ, De Maria A, Kisslo J, Weyman A. Recommendations regarding
quantification in M-mode echocardiography: results of a survey of
echocardiographic measurements. Circulation 1978;58:1072-83. http://dx.doi.org/10.1161/01.CIR.58.6.1072 PMid:709763
- Alder
R, Roesser EB. Introduction to probability and statistics.WH Freeman
and Company Eds. Sixth Edition.Sab Francisco (USA), 1975
PMCid:PMC1674139
- Le Roith D. Insulin-like growth factors. New Engl J Med 1997;336:633-40. http://dx.doi.org/10.1056/NEJM199702273360907 PMid:9032050
- Leung K C, Johannsson G, Leong G M, Ho K K. Estrogen regulation of growth hormone action. Endocr Rev 2004; 25: 693–721. http://dx.doi.org/10.1210/er.2003-0035 PMid:15466938
- Donahue
SP, Phillips LS: Response of IGF-1 to nutritional support in
malnourished hospital patients: a possible indicator of short-term
changes in nutritional status. Am J Clin Nutr 1989; 50:962–69.
PMid:2816803
- Platz
E A, Pollak M N, Rimm E B, Majeed N, Tao Y, Willett W C,Giovannucci E.
Racial variation in insulin-like growth factor-1 and binding protein-3
concentrations in middle-aged men. Cancer Epidemiol Biomark Prev 1999;
8:1107–10. PMid:10613344
- Soliman
AT, El Zalabany MM, Amer M, Ansari BM. Growth and pubertal development
in transfusion-dependent children and adolescents with thalassaemia
major and sickle cell disease: a comparative study. J Trop Pediatr
1999;45:23-30 http://dx.doi.org/10.1093/tropej/45.1.23 PMid:10191589
- Skordis
N, Kyriakou A. The multifactorial origin of growth failure in
thalassaemia. Pediatr Endocrinol Rev. 2011;8 (Suppl 2) :271-7.
PMid:21705977
- Soliman
AT, Abushahin A, Abohezeima K, Khalafallah H, Adel A, Elawwa A, Elmulla
N. Age related IGF-I changes and IGF-I generation in thalassemia major.
Pediatr Endocrinol Rev. 2011;8 (Suppl 2):278-83. PMid:21705978
- La
Rosa C, De Sanctis V, Mangiagli A, Mancuso M, Guardabasso V,Galati MC,
Caruso-Nicoletti M. Growth hormone secretion in adult patients with
thalassaemia. Clin Endocrinol (Oxf) 2005;62:667-71. http://dx.doi.org/10.1111/j.1365-2265.2005.02276.x PMid:15943827
- Scacchi
M, Danesi L, Cattaneo A, Valassi E, Pecori Giraldi F, Argento C,
D'Angelo E, Mirra N, Carnelli V, Zanaboni L, Cappellini MD, Cavagnini
F. Growth hormone deficiency in adult thalassaemic patients. Clin
Endocrinol (Oxf) 2007;67:790-5. http://dx.doi.org/10.1111/j.1365-2265.2007.02965.x PMid:17608814
- Pincelli
AI, Masera N, Tavecchia L, Perotti M, Perra S, Mariani R, Piperno A,
Mancia G, Grassi G, Masera G. GH deficiency in adult B-thalassemia
major patients and its relationship with IGF-1 production. Pediatr
Endocrinol Rev 2011;8 (Suppl 2):S284-9.
- Giovannucci
E. Insulin, insulin-like growth factors and colon cancer: a review of
the evidence. J Nutr 2001;131(11 Suppl S):3109S-20S. Hirschberg R,
Kopple JD: Effects of growth hormone and IGF-I on renal function.
Kidney Int 1989; Suppl 27:S20-S26.
- Poggi
M, Pascucci C, Monti S, Pugliese P, Lauri C, Amodeo G, Girelli G,
Toscano V. Prevalence of growth hormone deficiency in adult
polytransfused thalassemia patients and correlation with transfusional
and chelation parameters. J Endocrinol Invest 2010;33:534-8. http://dx.doi.org/10.1007/BF03346643 PMid:20157288
- Soliman
A, De Sanctis V, Yassin M, Abdelrahman MO. Growth hormone -
insulin-like growth factor-I axis and bone mineral density in adults
with thalassemia major. Indian J Endocrinol Metab. 2014;18:32-8. http://dx.doi.org/10.4103/2230-8210.126525 PMid:24701427 PMCid:PMC3968729
- Daughaday
WH. The possible autocrine/paracrine and endocrine roles of
insulin-like growth factors of human tumors. Endocrinology 1990;
127:1-4. http://dx.doi.org/10.1210/endo-127-1-1 PMid:2163304
- Furstenberger G, Senn HJ. Insulin-like growth factors and cancer. Lancet Oncol. 2002;3:298-302. http://dx.doi.org/10.1016/S1470-2045(02)00731-3
- Yu
H, Rohan T. Role of the insulin-like growth factor family in cancer
development and progression. J Natl Cancer Inst 2000;92:1472-89. http://dx.doi.org/10.1093/jnci/92.18.1472
- Bach LA, Rechler MM. Insulin-like growth factors and diabetes. Diabetes Metab Rev 1992; 8:229-57. http://dx.doi.org/10.1002/dmr.5610080304
- Garnero
P, Sornay-Rendu E, Delmas PD. Low serum IGF-1 and occurrence of
osteoporotic fractures in postmenopausal women. Lancet 2000;355:898-9. http://dx.doi.org/10.1016/S0140-6736(99)05463-X
- Puche
JE, Castilla-Cortázar I. Human conditions of insulin-like growth
factor-I (IGF-I) deficiency. J Transl Med. 2012 Nov 14;10:224. doi:
10.1186/1479-5876-10-224. http://dx.doi.org/10.1186/1479-5876-10-224
- Soliman
AT, Khalafallah H, Ashour R. Growth and fac¬tors affecting it in
thalassemia major. Hemoglobin. 2009;33 (Suppl 1):S116-26. http://dx.doi.org/10.3109/03630260903347781 PMid:20001614
- Isguven
P, Arslanoglu I, Erol M, Yildiz M, Adal E, Erguven M. Serum levels of
ghrelin, leptin, IGF-I, IGFBP-3, insulin, thyroid hormones and cortisol
in prepubertal children with iron deficiency. Endocr J 2007;54:985-90. http://dx.doi.org/10.1507/endocrj.K07-031 PMid:17998761
- Choi
JW, Kim SK. Association of serum insulin-like growth factor-I and
erythropoiesis in relation to body iron status. Ann Clin Lab Sci
2004;34:324-28. PMid:15487708
- El-Sisi
A, Khella A, Numan M, Dilwar M, Bhat A , Soliman AT. Linear growth in
relation to the circulating concentration of insulinlike growth
factor-I and free thyroxine in infants and children with congenital
cyanotic heart disease before vs. after surgical intervention. J Trop
Pediatr 2009;55: 302- http://dx.doi.org/10.1093/tropej/fmp010 PMid:19254914
- Leung
KC, Doyle N, Ballesteros M, Sjogren K, Watts CK, Low TH, Leong GM, Ross
RJ, Ho KK. Estrogen inhibits GH signaling by suppressing GH-induced
JAK2 phosphorylation, an effect mediated by SOCS-2. Proc Natl Acad Sci
U S A. 2003;100:1016-21. http://dx.doi.org/10.1073/pnas.0337600100 PMid:12552091 PMCid:PMC298718
- Ruiz
E, Osorio A, Torres JM, Ortega E. Evidence of different actions of
testosterone, estradiol, FSH, and LH on the growth axis. Endocr Res.
2001;27:25-33. http://dx.doi.org/10.1081/ERC-100107166 PMid:11428716
- Ameri
P, Giusti A, Boschetti M, Bovio M, Teti C, Leoncini G, Ferone D,
Murialdo G, Minuto F. Vitamin D increases circulating IGF1 in adults:
potential implication for the treatment of GH deficiency. Eur J
Endocrinol. 2013;169:767-72. http://dx.doi.org/10.1530/EJE-13-0510 PMid:24005315
- Alves
CX, Vale SH, Dantas MM, Maia AA, Franca MC, Marchini JS, Leite LD,
Brandao-Neto J. Positive effects of zinc supplementation on growth, GH,
IGF1, and IGFBP3 in eutrophic children. J Pediatr Endocrinol Metab.
2012;25:881-7 http://dx.doi.org/10.1515/jpem-2012-0120 PMid:23426817
- Sandhu
MS, Heald AH, Gibson JM, Cruickshank JK, Dunger DB, Wareham NJ.
Circulating concentrations of insulin-like growth factor-I and
development of glucose intolerance: a prospective observational study.
Lancet. 2002;359:1740–45. http://dx.doi.org/10.1016/S0140-6736(02)08655-5
- De
Sanctis V, Soliman A, Yassin M. Iron overload and glucose metabolism in
subjects with ß-thalassaemia major: an overview. Curr Diabetes Rev.
2013;9 :332-41. http://dx.doi.org/10.2174/1573399811309040005 PMid:23687960
- Soliman
AT, Yasin M, El-Awwa A, De Sanctis V. Detection of glycemic
abnormalities in adolescents with beta thalassemia using continuous
glucose monitoring and oral glucose tolerance in adolescents and young
adults with ß-thalassemia major: Pilot study. Indian J Endocrinol
Metab. 2013;17:490-5. http://dx.doi.org/10.4103/2230-8210.111647 PMid:23869308 PMCid:PMC3712382
[TOP]