Received: November 27, 2014
Accepted: February 2, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015023, DOI 10.4084/MJHID.2015.023
This article is available on PDF format at:

Hoda A. Abdelsamei1, Ashraf M. El-Sherif2, Ahlam M. Ismail3 and Gehan L. Abdel Hakeem4
1 Diagnostic Radiology Department, South Valley University.
2 Diagnostic Radiology Department and, Minia University.
3 Pediatrics Department South Valley University.
4 Pediatrics Department Minia University Egypt.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Background: Iron
overload in patients with beta-thalassemia major (BTM) lead to
alterations in the arterial structures and the thickness of the carotid
arteries. Doppler ultrasound scanning of extra-cranial internal carotid
arteries is non-invasive and relatively quick to perform and may
identify children at increased risk of stroke who would otherwise be
missed. Increased carotid artery intima media thickness (CIMT) is a
structural marker for early atherosclerosis and correlates with the
vascular risk factors and to the severity and extent of coronary artery
disease. Objective: To evaluate the role of carotid Doppler examination and CIMT measurement as a predictor of atherosclerotic changes in BTM children with iron overload. Patients and Methods: Sixty two children with BTM and, thirty age and sex matched normal controls were included. Complete blood count, ferritin, serum cholesterol were done, as well as carotid Doppler ultrasonography to measure the CIMT in both patients and controls. Results: CIMT of thalassemic patients was significantly increased compared to controls (p=0.001). There was a significant positive correlation between CIMT and patient's age, the duration from first blood transfusion, serum cholesterol and, iron overload parameters as serum ferritin, frequency of blood transfusion, iron chelation. The length of the transfusion period was the highest risk factor and splenectomy was a further risk factor. Significant negative correlation was found between CIMT and hematocrit value while no significant correlation was found between CIMT and weight, height, BMI centiles and Hb level. Conclusion: Carotid Doppler is very useful in measurement of CIMT that increased in thalassemic patients that shows a strong relationship with features of iron overload. Routine Doppler measurement of CIMT in these patients is recommended to predict early atherosclerotic changes as well as in follow-up. |
Introduction
Thalassemia syndromes are groups of heterogeneous hereditary
diseases characterized by a decrease or a total absence of synthesis of
α- and/or β-globin chains composing the hemoglobin protein in red blood
cells (RBCs).[1] They are classified according to the type of deficient
globin chain as α- and β-thalassemia.[2] In β-thalassemia, the severity
of the pathophysiology depends on the level of β-globin chain
deficiency, which leads to an excess of α-globin chains.[3]
Consequently, thalassemic RBCs are hypochromic and microcytic and have
a shorter half-life, leading to anemia.[4] Three clinical
phenotypes of decreasing severity have been established: a
transfusion-dependent state, thalassemia major, a moderate phenotype,
thalassemia intermedia, and a benign heterozygous condition,
thalassemia minor. Clinical features, in addition to the RBC anomalies,
are heterogeneous, and patients display several systemic
manifestations.[5] According to the so called “iron hypothesis”, iron
is believed to be detrimental for the cardiovascular system, thus
promoting atherosclerosis development and progression.[6] Iron over-
load in patients with beta-thalassemia major lead to alterations in the
arterial structures and the thickness of the carotid arteries. In
addition, carotid thickness positively correlated with age, Hb,
ferritin and cholesterol levels in these patients. As a result,
coronary artery diseases(CAD) is a quite common cardiovascular
complication in thalassemics. Patients on a regular transfusion regimen
progressively develop clinical manifestations of iron overload
associated with heart dysfunction and left ventricular failure if
inadequately chelated.[7] Doppler ultrasound scanning of extracranial
internal carotid arteries is non-invasive and relatively quick to
perform and may identify children at increased risk of stroke who would
otherwise be missed.[8] High resolution ultrasound is a reliable,
method for detecting early structural and functional atherosclerotic
changes in the arterial wall.[9] Increased carotid artery intima media
thickness (CIMT) is a structural marker for early atherosclerosis, and
it correlates with the vascular risk factors and to the severity and
extent of coronary artery disease.[10,11]
The study objectives:
This study aimed to evaluate the role of carotid Doppler examination
and CIMT measurement as a predictor to atherosclerotic changes
in B thalassemia major (BTM) children with iron overload.
Patients and Methods
This is a cross
sectional case control study. Sixty two children with BTM were selected
from the pediatric hematology outpatient clinics in Qena and Menia
University hospitals as well as 30 healthy normal age and sex matched
controls in the period from May 2013 to September 2014. Diagnostic
criteria, assessment and management of thalassemic children were based
on Guidelines for the Clinical Management of Thalassemia.[12] The study
was approved by the local research ethics committee of the two
hospitals and written informed consent was obtained from the parents of
all children to share in the study. Included patients with B
thalassemia proved by clinical and laboratory investigations, frequent
blood transfusion, chelation therapy. Patients with familiar
hypercholesterolemia (confirmed by history), cardiovascular symptoms
suggesting the presence of heart failure or atherosclerotic changes and
patients with chronic systemic illness were excluded. All patients were
subjected to the following work-up assessment:
I. The history
including the duration of the illness since the first blood
transfusion, the frequency of blood transfusion (frequent ≥ 2
times/month) and the intake of iron chelating agents. Chelation therapy
is initiated when serum ferritin levels reach approximately 1000 ng/mL
(subcutaneous deferroxamine, oral deferopron or combination of both)
and patients were classified as adequately chelated, poorly chelated or
non-chelated according to serum ferritin level, frequency of blood
transfusion and regularity of chelation.
II. Clinical
examination including general, chest, heart and abdominal examination.
Patient's anthropometric measurements were plotted on growth charts
(Official 2000 centers for centers for disease control (CDC) growth
charts, created by the National Center for Health Statistics
(NCHS).[13]
III. Laboratory and radiological investigations
including complete blood count, hemoglobin electrophoresis, serum
levels of ferritin and iron and iron binding capacity all were done at
the time of the study. Abdominal ultrasound was performed for detection
of the hepatomegaly and /or splenomegaly.
Carotid duplex study:
All patients and controls were subjected to B-mode and color-coded
duplex sonography of their extra-cranial carotid and vertebral
arteries. All studies were performed using a LOGIC P6 ultrasound system
(GE medical systems, Milwaukee, WI) with a 12.0-MHz linear array
transducer. All ultrasound examinations were performed by a single
experienced vascular radiologist who was unaware of the clinical and
laboratory details of the examined children. Examination started by
locating the common carotid artery (CCA) in the lower neck in the
transverse plane. The CCA is followed proximally until the transducer
is blocked by the clavicle, and caudal angulations is tried to evaluate
the common carotid origin if possible. The CCA continues upwards till
it widens to form the carotid bulb; then it bifurcates into internal
and external branches. The transducer is then rotated 90 degrees to be
parallel to the CCA to have longitudinal scanning of the CCA, the
bifurcation, the internal carotid artery (ICA) and external carotid
artery (ECA). The ICA was then followed distally as far as possible and
optimally until it is lost behind the mandible. The vessels were
evaluated meticulously for the presence of subintimal lucency, and
atherosclerotic plaques that bulge into the lumen, followed by
measuring the intimal plus medial thickness (IMT). IMT was measured in
1-cm segment proximal to the dilation of the carotid bulb, referred to
as CCA, and always in plaque-free segments. For each subject, three
measurements on both sides were obtained on the anterior, lateral, and
posterior projection of the far wall. Values for the different
projections and right and left arteries were then averaged. Two
end-diastolic frames were selected and analyzed for mean CIMT, and the
average reading from these two frames was calculated for both right and
left carotid arteries. The average of the two sides was considered the
patient’s overall mean CIMT. Statistical analysis: The data were
statistically analyzed using the SPSS software package, version 16
(SPSS Inc., Chicago, IL, USA) on a personal computer. Numerical data
were expressed as range, mean± SD, median, and percentiles. Non
numerical data were expressed as frequencies. Comparative studies were
done using Student t test and chi square test. (p value < 0.05 was
considered significant). Pearson correlation test was used to detect
correlation between different parameters. In addition, multiple
regression analysis was done to identify the most significant
risk factors.
Results
Demographic, clinical and laboratory data for patients and controls are shown in table 1. No significant difference between patients and controls regarding age or gender, while significant difference was found regarding weight, height and BMI centiles, Hb level, hematocrite value, serum ferritin and serum cholesterol. The duration since first transfusion ranged from 1.5-13 years with a mean of 7.26± 3.7. Thirty two patients (51.6%) had frequent blood transfusion, 24 patients (38.7%) were adequately chelated, and 24 patients (38.7%) undergone splenectomy operation. Table 2 shows comparison between patients and controls regarding CIMT. There was a significant difference between studied patients and controls regarding CIMT measurements (p =0.001). As shown in table 3 and figures 1 and 2, significant positive correlation was found between CIMT and patient's age, duration since the first blood transfusion, serum ferritin and serum cholesterol. Significant negative correlation was found between CIMT and hematocrit value while no significant correlation was found between CIMT regarding weight, height, BMI centiles and Hb level. CIMT was significantly increased in BTM children in relation to children with frequent blood transfusion, patients who were poorly chelating or had splenectomy (Table 4). Figures 3-5 show the ultrasonographic CIMT measurements and the Doppler spectrum of the carotid vessels in healthy controls and in patients with BTM. Table 5 and figure 6 display the risk factors increasing CIMT in thalassemic patients. Duration of illness carries the highest risk factor followed by the inadequate iron chelation therapy.
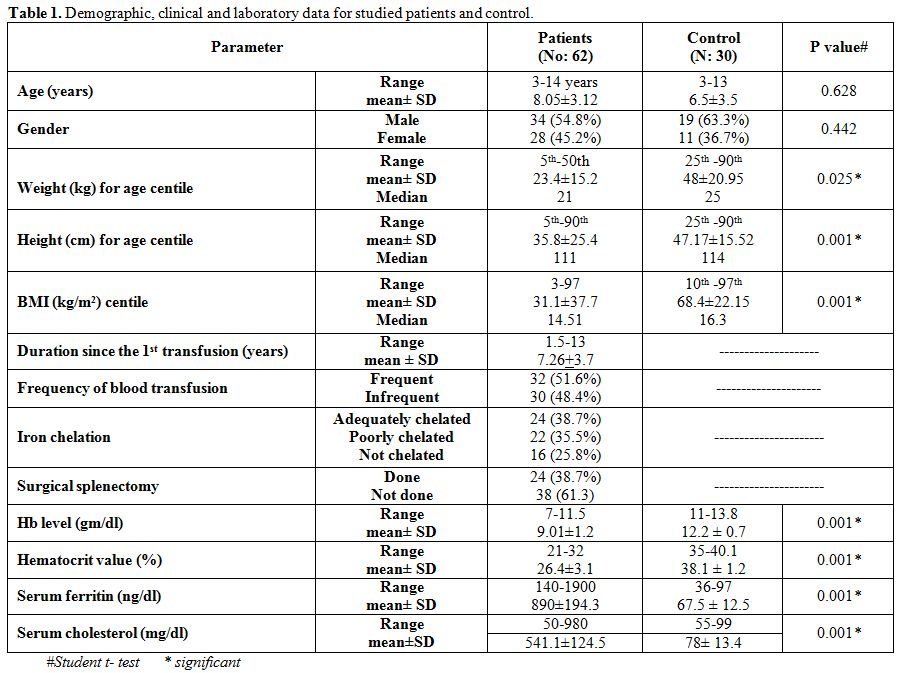 |
Table 1. Demographic, clinical and laboratory data for studied patients and control. |
 |
Table 2. Comparison between patients and controls regarding CIMT(mm). |
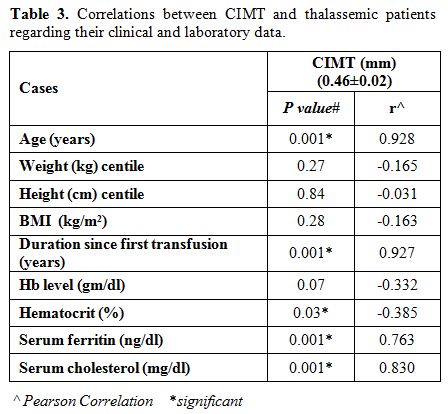 |
Table 3. Correlations between CIMT and thalassemic patients regarding their clinical and laboratory data. |
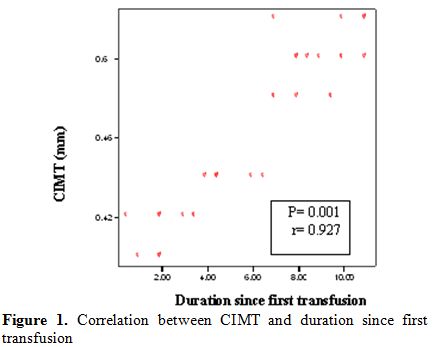 |
Figure 1. Correlation between CIMT and duration since first transfusion. |
 |
Figure 2. Correlation between CIMT and serum ferritin. |
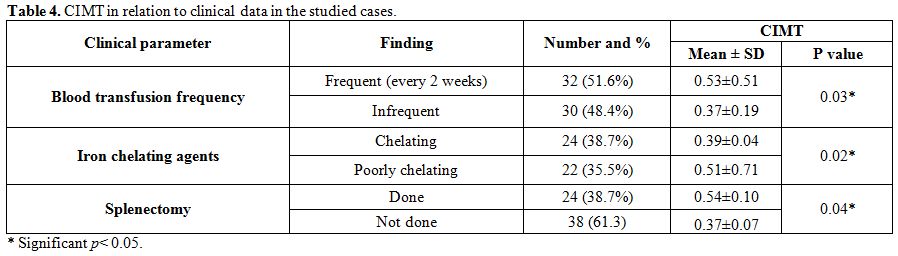 |
Table 4. CIMT in relation to clinical data in the studied cases. |
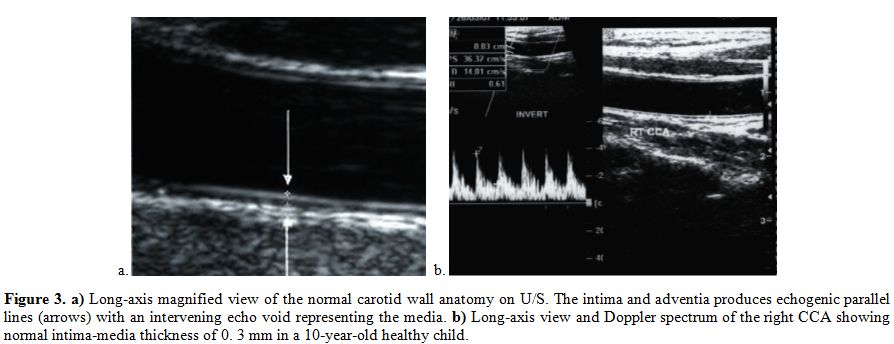 |
Figure 3. a) Long-axis magnified view of the normal carotid wall anatomy on U/S. The intima and adventia produces echogenic parallel lines (arrows) with an intervening echo void representing the media. b) Long-axis view and Doppler spectrum of the right CCA showing normal intima-media thickness of 0. 3 mm in a 10-year-old healthy child. |
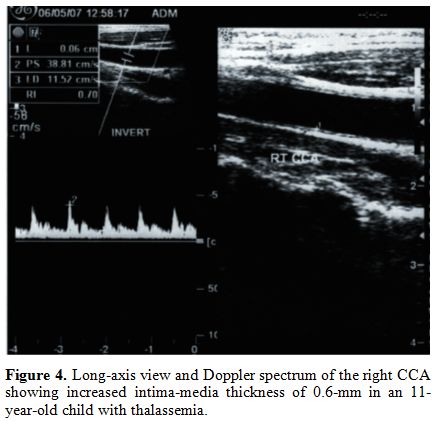 |
Figure 4. Long-axis view and Doppler spectrum of the right CCA showing increased intima-media thickness of 0.6-mm in an 11-year-old child with thalassemia. |
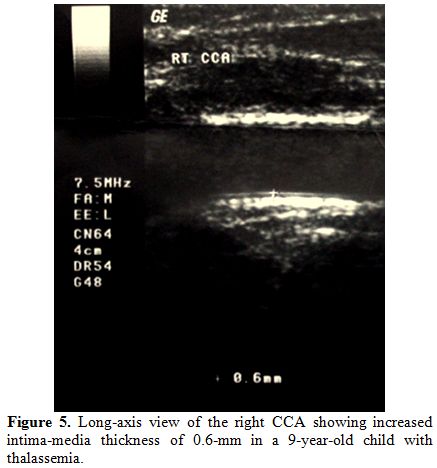 |
Figure 5. Long-axis view of the right CCA showing increased intima-media thickness of 0.6-mm in a 9-year-old child with thalassemia. |
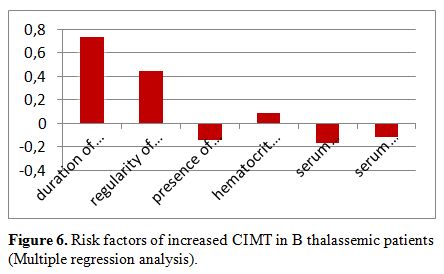 |
Figure 6. Risk factors of increased CIMT in B thalassemic patients (Multiple regression analysis). |
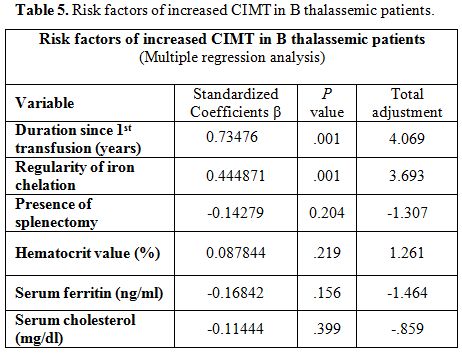 |
Table 5. Risk factors of increased CIMT in B thalassemic patients. |
Discussion
Beta-thalassemia is a group of hereditary blood disorders first described by Cooley and Lee.[14]
With the increased life span of BTM patients, coronary artery disease
may emerge as one of the important cardiovascular complications.[15]
Studies have suggested a link between iron load and risk of
atherosclerosis. The present study was undertaken to evaluate the
role of carotid Doppler examination and CIMT measurement as a
predictive to atherosclerotic changes in BTM children with iron
overload. Our data show that the CIMT of thalassemic patients was
significantly increased compared to controls. This finding is supported
by the results of some previous studies;[16-18] Cheung et al.,[19] found an increase in the CIMT in patients with BTM compared to controls, Tantawy et al, 2009[17] and Gullu et al,[18] found the same results in their study, and Adly et al. [19]
reported that Carotid IMT measurements were significantly but slightly
higher in the BTM group than that in the controls (0.57 ± 0.07 vs. 0.54
± 0.04, P = 0.04) and that CIMT is increased in patients with BTM. On
the other hand, a previous study, carried out by Cusmà et al.,[20]
comparing the CIMT between the thalassemic patients and healthy
subjects (0.67 ± 0.20 mm vs 0.66 ± 0.15 mm), shown no significant
difference. The conclusion of this research was that 2-dimensional
strain and echo-tracking might be more accurate than standard
echocardiography and vascular parameters in the early identification of
cardiovascular involvement.
The development of carotid artery
wall hypertrophic remodeling, found in thalassemic patients, is
characterized by an increase in both total wall thickness and
wall-to-lumen ratios; hemolysis likely contributed to the
pathophysiology of both endothelial dysfunction as well as vascular,
structural and mechanical, changes.[22] In our study,
there was significant statistical correlation between CIMT and
patient’s age, ferritin, and total cholesterol levels but there was no
significant difference of CIMT in relation to patient’s hemoglobin
level. This also comes in harmony with the study of Tantawy et al.[17]
who reported that in thalassemic patients, CIMT was positively
correlated with age, ferritin and cholesterol levels, and that
atherogenic lipid profiles in young thalassemic patients with increased
CIMT highlights their importance as prognostic factors for vascular
risk stratification. These findings are further supported by Gursel et
al.,[22] who investigated the relationship between
chronic hemolysis and increased body iron burden and the development of
premature atherosclerosis by using CIMT, ferritin, serum lipid profile.
They concluded that Subclinical atherosclerosis in children with
β-thalassemia major begins early in life, and these children are at
risk for development of premature atherosclerosis. Iron overload is
usually associated with regular blood transfusions which lead to
transfusional haemosiderosis in patients with chronic anemia in
children with BTM.[23] These changes occur initially
in reticulo-endothelial system and secondary in all parenchymal organs,
mainly heart, pancreas, pituitary gland, and gonads, with cytotoxic
effects.[24] So, accumulation of iron has been
implicated as a risk of cardiovascular disease, because of the
catalytic role of iron, causing oxidative stresses on the vessel wall.[25-27]
We also found that CIMT was significantly different in children with
BTM in relation to features suggestive of iron overload including
duration since first blood transfusion which carries the highest risk
factor of increasing CIMT, frequency of blood transfusion, irregular
use of iron chelating agents in patients who were poorly chelating or
had splenectomy. This comes in harmony with the results of a previous
study that was carried out by Cheung et al,[28] who
found that iron overloading in patients with beta-thalassemia major
results in alterations of arterial structures with disruption of
elastic tissue and calcification. This finding is also supported by
Ramakrishna et al.,[29] as well as other epidemiological studies concluding that iron is an important factor in the process of atherosclerosis[27]
and that CIMT is considered an early marker of atherosclerotic process
and is currently used to assess the presence and the progression of
atherosclerosis.[30,31] A significant positive
correlation was found in this study between duration since first blood
transfusion and CIMT, the longer the duration, the more atherogenesis
as reflected by increased CIMT. And also, there was another significant
positive correlation between serum ferritin levels and CIMT. Duration
of illness carries the highest risk factor of increasing CIMT followed
by the iron chelation therapy guided by serum ferritin. The catalytic
role of iron in free radical reactions causes oxidation of LDL and may
be an important factor in the formation of atherosclerotic lesions.
Studies have shown that iron can stimulate lipid peroxidation in vitro
and in vivo.[29] Oxidized LDL is followed by
accumulation of lipids in cells and the formation of foam cells,
characteristic of early atherosclerosis. Thereby, oxidized LDL has
cytotoxic capacity that induces changes in endothelial cells with loss
of endothelial integrity, which could facilitate further accumulation
of both circulating monocytes and LDL and thus promote the progression
of the atherosclerotic lesion.[32-35]
Conclusion
Carotid Doppler is very useful method in measurement of CIMT that
increased in thalassemic patients. CIMT shows a strong relationship
with features of iron overload and atherosclerotic changes. Duration of
illness carries the highest risk factor of increasing CIMT followed by
inadequate iron chelation therapy. Prevention of the progression of
atherosclerosis in early stages is important by decreasing body iron
load in the thalassemic patients. We recommend the routine use of
Doppler measurement of CIMT in BTM patients as a non-invasive
diagnostic method to predict early atherosclerotic changes as well as
in the follow-up to prevent progression of atherosclerosis. Reducing
hyper-lipidemia and body iron load in the thalassemic patients by
dietary restriction or pharmacological therapy and good compliance of
iron chelating agents is also recommended.
References

[TOP]