Received: June 6, 2015
Accepted: August 8, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015050, DOI 10.4084/MJHID.2015.050
This article is available on PDF format at:

Omar Al-Rawi1, Fawzi Abdel-Rahman1, Rula Al-Najjar1, Husam Abu-Jazar1, Mourad Salam1 and Mustafa Saad2
1 Stem cell & bone marrow transplantation program, King Hussein Cancer Center, Amman, Jordan
2 Division of Infectious Diseases, Prince Sultan Cardiac Center, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Introduction: Cytomegalovirus
(CMV) reactivation and infection are well-recognized complications after
allogeneic stem cell transplantation (SCT). Only a few studies have addressed
CMV reactivation after autologous SCT (ASCT). Methods: We retrospectively
reviewed medical records of 210 adult patients who underwent ASCT for lymphoma
or multiple myeloma (MM) at a single
center from January 1st, 2007 until December 31st, 2012.
All patients were monitored weekly with CMV antigenemia test till day 42 after
transplantation, and for 2 months after last positive test in those who had any
positive CMV antigenemia test before day 42. Results: Thirty-seven (17.6%)
patients had CMV reactivation; 23 patients had lymphoma while 14 had MM as the
underlying disease. There was no difference in the rate of CMV reactivation
between lymphoma and MM patients (20% versus 14.7%, P = 0.32). The majority
of the patients were treated with
ganciclovir/valganciclovir, all patients had their reactivation resolved with
therapy, and none developed symptomatic CMV infection. None of the patients who
died within 100 days of transplantation had CMV reactivation. Log-rank test
showed that CMV reactivation had no effect on the overall survival of patients
(P values, 0.29). Conclusion: In our cohort, CMV
reactivation rate after ASCT was 17.6%. There was no difference in reactivation
rates between lymphoma and MM patients. With the use of preemptive therapy,
symptomatic CMV infection was not documented in any patient in our cohort. CMV
reactivation had no impact on patients’ survival post ASCT. |
Introduction
Cytomegalovirus (CMV) reactivation and infection are known
complications of allogeneic stem cell transplantation (SCT). Its
incidence is more frequent after allogeneic SCT than after autologous
SCT.[1]
Previous studies on CMV reactivation
after autologous SCT (ASCT) showed an incidence of 30-40% in patients
who were monitored by weekly CMV polymerase chain reaction (PCR) or
antigenemia tests, and 1-13% in those monitored by clinical signs of
CMV infection.[2-10]
The incidence of CMV
reactivation following ASCT has not been carefully evaluated in subsets
of patients with different underlying hematological malignancies such
as multiple myeloma (MM) and lymphoma. Studies in this regard are
sparse.
The prevalence of CMV immunoglobulin G (IgG)
positivity in the population of the Eastern Mediterranean region is
reported to be higher than that of the population of the western
countries; Bazarbachi et al. reported a prevalence of 90% in the
Eastern Mediterranean region compared to 60% in Europe.[11]
We
performed this single-center study to evaluate the incidence of CMV
reactivation in recipients of ASCT, to compare the incidence of CMV
reactivation in patients with lymphoma versus multiple myeloma (MM),
and to assess the outcome of these reactivations and their impact on
transplant recipients’ survival.
Patients and Methods
Patients: We included all patients who had ASCT at King Hussein Cancer Center, Amman, Jordan, in the period between January 1st, 2007 and December 31st,
2012. Data were retrospectively collected from the patients’ medical
records and the bone marrow transplantation program’s database. We
collected information on patients’ demographics, underlying diseases,
CMV status, conditioning regimens, CMV reactivation, presence of signs
and symptoms of CMV infection, treatment modalities, CMV reactivation
outcomes, and patients’ survival. Composed data entered into a
computerized database and then were analyzed. The protocol was approved
by the local Institutional Review Board; written informed consent was
waived.
Locally developed guidelines were followed for the diagnosis and management of patients with CMV reactivation.
Definitions:
CMV reactivation was defined as a positive CMV antigenemia test in ≥ 5
cells/250,000 leukocytes examined, or if the test was positive in less
than 5 cells on two or more consecutive occasions with unexplained
cytopenias and/or liver enzyme elevation.
Cytopenias were defined as an absolute neutrophil count (ANC) <1000 x109/L, platelet count <70 x109/L,
and/or hemoglobin level less than 10 gm/dl. Patients were considered to
have liver enzyme elevation if they developed values more than 1.5
times the upper limit of normal. These patients underwent careful
evaluation for other potential causes of cytopenias and/or liver enzyme
elevations such as drugs, and other viral infections.
CMV
pneumonia was defined as the presence of interstitial infiltrates on
chest radiographs accompanied by a histopathological demonstration of
CMV in lung biopsy material. CMV gastrointestinal infection was defined
as the presence of gastrointestinal symptoms accompanied by a
histopathological diagnosis of CMV infection.
CMV monitoring:
All patients were routinely monitored for CMV reactivation on weekly
basis after engraftment until day 42 post stem cell infusion, and those
with positive CMV antigenemia test before day 42 were further
monitored for 2 months after last positive test. Monitoring was done by
testing for the presence of CMV pp65 antigenemia. CMV antigenemia assay
is based on the detection of the CMV lower matrix protein pp65 in
polymorphonuclear leukocytes by immunostaining with monoclonal
antibodies.
CMV antigenemia testing was performed in duplicates[12] using cytocentrifugation slides prepared of 2.5 X 105 peripheral blood leukocytes per slide. Slides then were fixed with formaldehyde,[12,13]
and then stained with the immunofluorescence staining using monoclonal
antibodies ppUL83 (pp65) blend (Argene, Biomerieux, Marcy l'Etoile,
France).
Antiviral prophylaxis and therapy: All patients were given prophylaxis with acyclovir 250mg/m2 intravenously every 8 hours from day minus 3 until white blood cell engraftment (absolute neutrophil count [ANC] > 500 x109/L
for 2 consecutive days) when they were changed to oral acyclovir 400 mg
every 12 hours. Routine CMV monitoring was started immediately after
engraftment by weekly CMV antigenemia testing till day 42
post-transplant. Patients who developed a positive CMV antigenemia test
but did not meet the criteria for CMV reactivation (i.e. more than 5
positive cells, or more than two readings less than 5 cells with
unexplained cytopenias and/or liver enzyme elevation) had their
prophylaxis changed to valacyclovir 1 gm orally every 8 hours.
Patients with CMV reactivation having adequate blood counts (ANC>1000 x109/L, and platelets >70 x109/L) were treated with ganciclovir 5mg/kg every[12]
hours during the induction phase of therapy followed by 5mg/kg every 24
hours during the maintenance phase. Alternatevely, valganciclovir 900
mg was give orally twice a day during the induction phase followed by
900 mg and daily during the maintenance phase of therapy. On the
other hand, patients who had cytopenias were treated with foscarnet at
a dose of 90 mg/kg every 12 hours for induction followed by 90mg/kg
every 24 hours for maintenance therapy.
The induction therapy was
given initially for 7 days, and if repeat CMV antigenemia test became
negative, patients were then switched to maintenance therapy for 10
more days. On the other hand, if positive results appeared on repeated
testing, induction therapy was continued, repeat CMV antigenemia
testing was done twice weekly, and patients were switched to
maintenance therapy once the test turned negative.
Statistical analysis:
Descriptive statistics was performed on demographic data and clinical
information of patients, showing counts and percentages for categorical
data, and medians and ranges for continuous data. Chi-square test was
used to compare categorical data as appropriate, depending on the
assumptions required for each test. Overall survival was presented
using Kaplan-Meier curves. Log-rank test was used to compare survival
times. A P value of < 0.05 was considered statistically significant.
All analyzes were performed using SAS version 9.1 (SAS Institute Inc,
Cary, NC).
Results
A total of 210 consecutive adult patients with lymphoma (55%) and MM
(45%) who underwent ASCT were included. The majority of patients were
females (58.6%), less than 50 years old (61.9%), had partial remission
of their underlying hematological malignancy before transplantation
(70%), and received acyclovir for prophylaxis (94.3%). Of the 210
patients, 205 (97.6%) were CMV IgG positive before transplantation
while 10 (4.8%) were CMV IgM positive. All of the latter had a negative
baseline CMV antigenemia test.
All patients received appropriate
chemotherapy to treat the underlying hematological malignancy before
being considered for transplantation. Patients with MM were treated
with thalidomide and dexamethasone as first-line therapy; as for
high-risk patients, cyclophosphamide was added to this regimen. Ten
patients received bortezomib as a second-line therapy due to poor
response to first-line chemotherapy. Patients with Hodgkin lymphoma
were treated with ABVD (adriamycin, bleomycin, vinblastine, and
dacarbazine), while those with diffuse large B-cell lymphoma were given
R-CHOP (rituximab, cyclophosphamide, adriamycin, vincristine, and
prednisone) as first-line therapy. Second-line chemotherapy in lymphoma
patients was DHAP (dexamethasone, ara-C, and cisplatin), third-line was
ICE (ifosfamide, carboplatin, and etoposide), and the fourth-line was
mostly navelbine, or gemcitabine.
Three conditioning regimens were
used according to the underlying disease. In the lymphoma group, 111
(96.5%) patients received BEAM (BCNU, etoposide, cytarabine, melphalan)
chemotherapy regimen for conditioning, and 4 (3.5%) patients received
TEAM (thiotepa, etoposide, cytarabine, melphalan). All patients with MM
received melphalan 200mg/m2 as the
conditioning regimen. All patients had white blood cell engraftment by
day 15 of transplantation (median, 10 days). Overall mortality in our
cohort was 23.8%, while day 100 mortality was 2.9%. Table 1 outlines clinical characteristics of the study cohort.
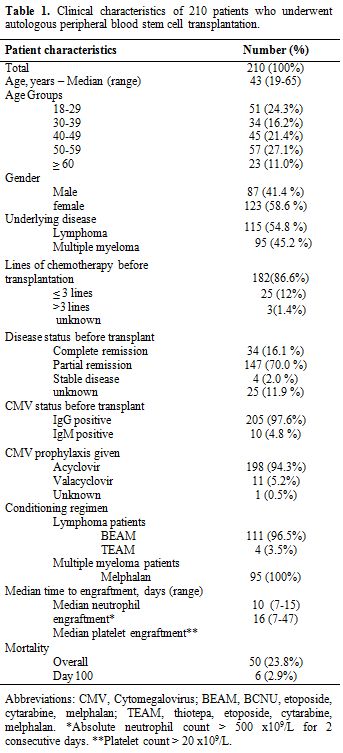 |
Table 1. Clinical characteristics of 210 patients who underwent autologous peripheral blood stem cell transplantation. |
Overall, 37 (17.6%) patients had CMV reactivation. The
median time to CMV reactivation was 31 days (range, 21-54 days). Some
patients were continued on monitoring beyond day 42, because they had
CMV antigenemia positivity during the first 42 days, so they were
monitored for another two months from the last positive test.
At
the time of reactivation, 35 (94.6%) patients were treated with
ganciclovir or valganciclovir. Foscarnet was used to treat CMV
reactivation in 2 (5.4%) patients due to baseline cytopenias
(ANC<1000 x109/L, and/or platelets <70 x109/L).
All patients had their CMV reactivation resolved with therapy, and none
developed symptomatic CMV infection. The anti-CMV induction and
maintenance therapies were given for a median of 8 and 10 days,
respectively. The majority of side effects from therapy were cytopenias
in the ganciclovir/valganciclovir treated patients, and electrolyte
disturbances and renal impairment in the foscarnet treated patients.
The overall mortality was 29.7% among patients with CMV reactivation.
However, none of the patients who died within 100 days of
transplantation had CMV reactivation. Table 2 summarizes the characteristics of patients who developed CMV reactivation.
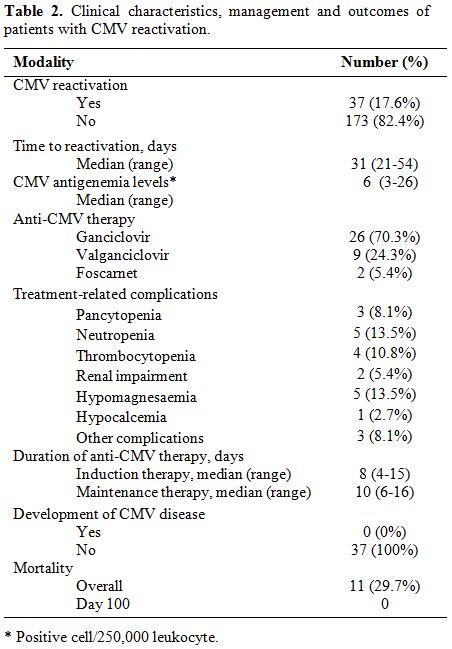 |
Table 2. Clinical characteristics, management and outcomes of patients with CMV reactivation. |
There was no statistically significant difference in
the rate of CMV reactivation
between patients with lymphoma compared to patients with
MM. In addition, older age (≥ 50 years), stage of the underlying
hematological malignancy, disease status at the time of
transplantation, number of lines of chemotherapy before
transplantation, pre-transplant hepatitis B core IgG (HBcIgG)
positivity , and CMV status prior to transplantation, did not correlate
with CMV reactivation as shown in Table 3.
Furthermore, prior therapy with bortezomib in patients with MM was not
associated with increased risk of CMV reactivation (P = 0.09).
Patients
were followed up for a median of 32.3 (range, 3.9-75) months. The
overall survival (OS) in our cohort was 76.2%, and the progression-free
survival (PFS) was 55%. The log-rank test showed no difference in the
OS between patients who had CMV reactivation compared to those who did
not (p-values, 0.29) (Figures 1).
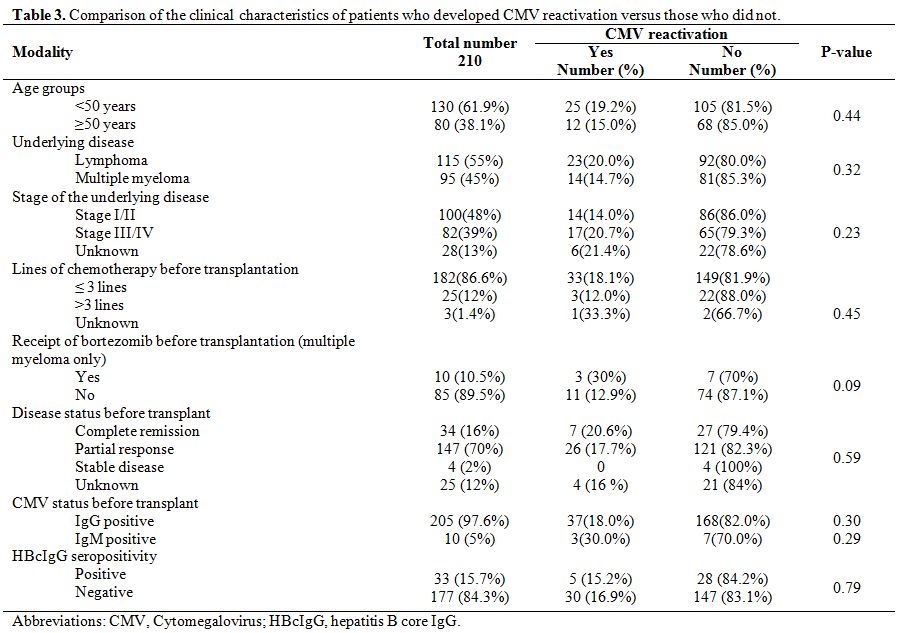 |
Table 3. Comparison of the clinical characteristics of patients who developed CMV reactivation versus those who did not. |
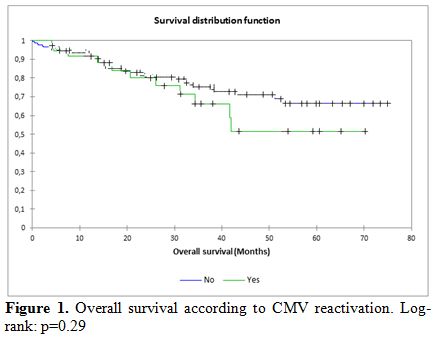 |
Figure 1. Overall survival according to CMV reactivation. Log-rank: p=0.29 |
Discussion
CMV reactivation is a common complication after hematopoietic stem
cell transplantation, and it is more frequently reported after
allogeneic versus autologous SCT. Routine monitoring of CMV
reactivation following ASCT is not a universal practice among all
transplant centers. The recommendations of the European Conference on
Infections in Leukemia (ECIL) considered the routine surveillance for
CMV reactivation after ASCT to be unnecessary because of the low
likelihood of CMV disease. Nonetheless, high risk ASCT recipients,
including those receiving CD34-selected grafts, and those who had prior
treatment with fludarabine, cladribine, or alemtuzumab were considered
to be potential candidates for CMV monitoring and the use of
pre-emptive therapy.[14]
The incidence of CMV IgG positivity in our population is 90% compared to 60% in the European population.[11]
Furthermore, Han et al reported that the CMV antigenemia rate among
seropositive non-transplant cancer patients was 14.3%, compared to only
2.5% among CMV seronegative patients.[8] Our practice
from 2003 to 2007 was to monitor routinely for CMV reactivation till
day 100 post transplant. In 2007, we modified our practice to monitor
for CMV reactivation in ASCT patients until day 42 based on our
observation that patients who did not have reactivation before day 42
did not develop reactivation after that. Although none of them did
receive CD34-selected graft, Alemtuzumab, Cladribine, or Fludarabine
before ASCT, we didn’t stop routine monitoring of our patients
considering the high incidence of CMV IgG seropositivity in our
population.
In this study, despite the higher prevalence of CMV
positivity, the rate of CMV reactivation (17.6%) was lower than what
has been reported (30-40%) in previous studies.[2-10]
Differences in the study design may at least partially account for this
lower-than-anticipated rate. Polymerase chain reaction (PCR) was used
in some studies for CMV monitoring; this is a more sensitive test as
compared to the CMV antigenemia test used in our study. Furthermore, we
did not include patients with a positive CMV antigenemia test that did
not meet the preset definition of CMV reactivation in our cohort.
In
our cohort, the rate of CMV reactivation was higher in patients with
lymphoma (20%) compared to patients with MM (14.7%). However, the
univariate analysis showed no association between the underlying
disease and CMV reactivation. In comparison, Rossini et al. reported
higher rates of CMV reactivation in patients with MM (42%) compared to
patients with lymphoma (29%).[2] However, the effect of the underlying disease on CMV reactivation was not further analyzed in Rossini’s study.
Only
10 patients with MM of our cohort received bortezomib-based therapy
before transplantation; three of which had CMV reactivation (30%)
compared to 11 out of 85 (12.9%) patients who did not receive
bortezomib, but the difference was not statistically significant. The
lack of statistical difference in our study may in part be due to the
small number of patients who received bortezomib. In a study that
compared 80 patients with MM who received novel therapies prior to
transplantation versus 89 patients who were treated with standard
regimens, Marchesi et al reported a significantly higher rate of CMV
reactivation in the former group.[15]
Kim et al.[16]
reported on the association of tandem transplantation and CMV
reactivation; this was not assessed in our study due to the fact that
tandem transplantation was not utilized routinely in our cohort of
patients.
Marchesi et al. reported that pre-transplant HBcIgG
seropositivity was a predictor of clinically relevant CMV infection in
patients with lymphoma undergoing ASCT, with a 40% rate of CMV
reactivation in HBcIgG-positive patients compared to 9.8% in
HBcIgG-negative patients (P value, 0.008).[17] This
was not the case in our study, as the rate of CMV reactivation in the
HBcIgG-positive group was 15.2%, compared to 16.9% in the negative
group (P value, 0.79). This difference might be due to the low rate of
CMV reactivation in our study (17.6%) compared to 40% in the Marchesi
study which used PCR for monitoring rather than CMV antigenemia testing.
Previous
studies have shown superiority of valacyclovir prophylaxis in
comparison to acyclovir in recipients of allogeneic SCT with less CMV
reactivation.[18,19] This datum inspired
the rationale for our strategy of switching to valacyclovir prophylaxis
in patients who had a positive CMV antigenemia test that did not meet
the definition of CMV reactivation in our study. In our cohort eleven
patients were switched from acyclovir to valacyclovir, but despite this
switch 80% of these patients had rising CMV antigenemia levels on
repeated tests that required preemptive therapy.
The duration of CMV monitoring following ASCT varied in different studies. In the study by Kim et al.,[16]
CMV monitoring was done until patients started on maintenance
chemotherapy after transplantation for MM, while in the study by
Rossini et al., monitoring was done till day 60 post-transplantation.[2]
In our cohort, we monitored CMV reactivation until day 42 if no
positive CMV antigenemia test was documented, and extended it to 2
months after the last positive test in those who had any positive CMV
antigenemia test before day 42. This strategy seems to have been
effective; the median time for reactivation in our study was 31 (range,
21-54) days and all cases of CMV reactivation were detected during the
monitoring period. This finding is similar to that reported by Marchesi
et al.[15] where the median time to CMV reactivation was 33 days.
In
our cohort, treatment of CMV reactivation followed the usual standards
with ganciclovir and valganciclovir being used in the majority of
patients (94.6%) as the initial preemptive therapy. Furthermore, all
patients who had CMV reactivation cleared their CMV antigenemia with
the first line of therapy, and no patient developed symptomatic CMV
infection.
It is interesting to note that CMV reactivation did
not affect the overall survival of patients in our cohort. Moreover,
none of the patients who developed CMV reactivation died in the first
100 days post transplantation.
This study has some limitations
inherent to its design. It is a retrospective study and from a single
cancer center. Therefore, our findings may not apply to other centers
with different patient populations. Also, testing for CMV reactivation
was carried out by the CMV antigenemia test only with no utilization of
PCR. Finally, most of the patients in our cohort received standard
chemotherapeutic regimens prior to transplantation, so the effect of
different modalities of treatments used before transplantation,
especially novel therapies, on the CMV reactivation could not be
carefully assessed.
In conclusion, in our cohort of lymphoma and
MM patients, the rate of CMV reactivation following ASCT was 17.6%.
There was no difference in reactivation rates between lymphoma and MM
patients. With the use of preemptive therapy, symptomatic CMV infection
was not documented in any patient in our cohort. Monitoring of CMV
antigenemia until day 42 post-transplantation seemed to be effective in
patients who did not have any positive CMV antigenemia test. CMV
reactivation had no impact on patients’ survival post ASCT.
References

[TOP]