Received: September 30, 2015
Accepted: November 18, 2015
Mediterr J Hematol Infect Dis 2016, 8(1): e2016002, DOI 10.4084/MJHID.2016.002
This article is available on PDF format at:

| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract We introduce a 78-year-old woman
presented with thrombocytosis and high blast count who had a history of
splenectomy. Her cytogenetic analysis revealed aberrant chromosomal
rearrangements in different clonal populations harboring 46XX karyotype
with t(9;22) (q34;q11). RT-PCR assay detected the e1a2 BCR-ABL translocation resulting from rearrangement of the minor breakpoint cluster region (m-bcr) in BCR gene. Subsequent evaluation of the disease showed calreticulin (CALR) 52-bp deletion as well as the absence of JAK2V617F
heterozygous mutation in granulocyte population of peripheral blood
using allele-specific PCR and bi-directional DNA sequencing. To our
knowledge, this is the first case of a patient initially diagnosed as
p190 BCR-ABL transcript positive CML in blast crisis characterized by a 52-bp deletion in CALR gene. |
Introduction
Chronic myeloid leukemia (CML) is the most important
myeloproliferative neoplasm (MPN) developed due to the known
t(9;22)(q34;q11) chromosomal translocation in pluripotential
hematopoietic progenitor cells. This genetic alteration results in the
formation of Philadelphia chromosome (Ph́), comprising portions of
Abelson (abl) and breakpoint cluster region (bcr) genes.[1,2]
This fusion transcript is present in 90-95% of patients with CML
andserves as adiagnostic and prognostic biomarker. It is also a
therapeutic target in cases with a wide spectrum of clinical symptoms,
including hypercellular bone marrow (BM), splenomegaly, anemia or
platelet dysfunction as well as significant increase in the number of
leukocytes, especially neutrophils and immature myeloid cells.[3] Unlike the common form of p210 BCR-ABL oncoprotein, in which the breakpoint occurs between exon 2 of ablgene on chromosome 9 and exons e12–e16 of the bcrgene on chromosome 22, the first exon of bcrgene
is involved in this translocationin 1-2% of CML patients. This rare
fusion transcript, also known as minor breakpoint cluster region
(m-bcr), codes for a smaller (190kDa) oncoprotein with a unique
clinical presentation between CML and chronic myelomonocytic leukemia
(CMML).[4]
Besides the identification of mutations in Janus kinase 2 (JAK2) and thrombopoietin receptor (MPL) genes BCR/ABL negative MPNs, calreticulin (CALR)
gene mutations have also been used in classification and determination
of diagnostic criteria for MPNs and myelodysplastic/myeloproliferative
neoplasms (MDS/MPN), including essential thrombocythemia (ET), primary
myelofibrosis (PMF) and refractory anemia with ring sideroblasts
associated with marked thrombocytosis (RARS-T), respectively.[5] Insertion/deletion mutations in exon 9 of CALR
does not occur in CML, but some authors have recently reported the
existence of these somatic changes in remaining portions of nonmutated JAK2 and MPL MPN cases.[6]
We report the case of a CML patient with p190 type BCR–ABL transcript who also harbored CALR 52-bp deletion. Beyond a few studies of CML patients with p190 kDa fusion protein,[7] to the best of our knowledge, this is the first report to describe the coexistence of P190 BCR/ABL transcript and CALR
52-bp deletion in blast crisis in a CML patient. Herewith, we have
presented a detailed insight into the study of clinical and molecular
cytogenetic findings to assess the prognostic information in guiding
management strategies for our patient.
Case Report
A 78-year-old woman was admitted to our department in May 2015 with
pallor, weakness and a remote history of splenectomy. Her peripheral
blood (PB) revealed anemia with a hemoglobin concentration of 8.6 g/dL,
thrombocytosis (789,000×103/µL),
white blood cell (WBC) count of 68200/μL with 16% neutrophils, 1%
eosinophils, 1% monocytes, 48% lymphocytes, 16% atypical lymphocytes
and 18% blasts. Morphologic review of the PB smear revealed basket
cells and nucleated red blood cells. BM aspirate smears showed
hypercellular marrow with increased blasts (Figure 1A) and platelets (Figure 1B). Blasts showed a fine chromatin pattern, round nuclei, and scanty cytoplasm.
Cytogenetic
analysis indicated the presence of der(11), der(17) and der(18)
chromosome abnormalities in different clonal populations harboring 46XX
karyotype with t(9;22) (q34;q11) (Figure 1C, 1D) in addition to the observed BCR-ABL fusion gene in BM metaphases by fluorescence in situ hybridization (FISH) (Figure 1E).
In the first step of verification at the molecular level, RT-PCR was
performed for detection of p210-type mRNA as previously described,[8] but sequence analysis of amplification products did not show the p210 BCR-ABL positive rearrangement. This result prompted us to investigate p190BCR-ABL
mRNA fusion transcript by RT-PCR assay according to standard
procedures, which was positive in our patient similar to rare cases of
CML with an inferior outcome of therapy.[9]
The
initial manifestation of the disease was an overwhelming splenomegaly;
however, the patient was referred to our center with a high platelet
count anterior to splenectomy. In consideration of the possibility of a
chronic myeloproliferative disease transformed in the acute phase, it
has been carried out allele-specific PCR to detect the mutation JAK2V617F. Combining the previously published studies with current data, including a high platelet count and the absence of JAK2V617F mutation, we were encouraged to study mutations in exon 9 of CALR by bidirectional sequencing in the following investigations (Figure 1F),[10] which surprisingly revealed a del52CALR mutant with a high allele burden in granulocyte population.
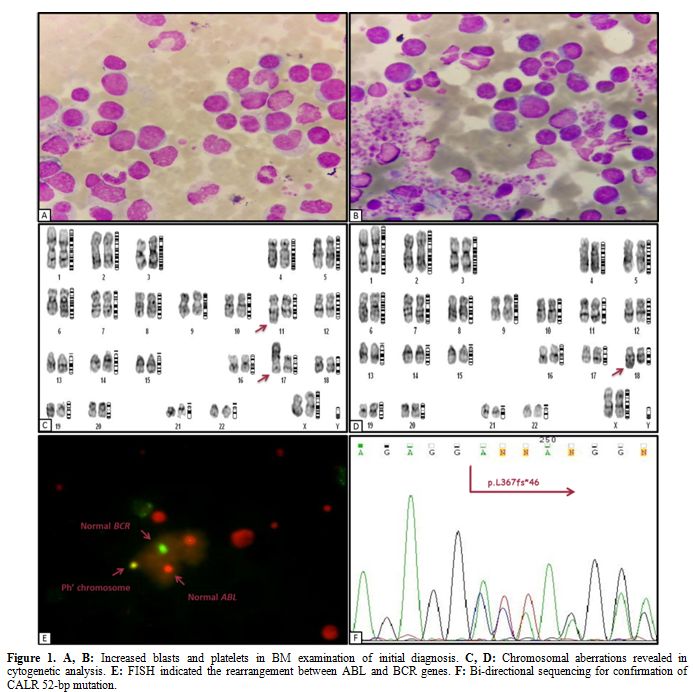 |
Figure 1. A, B: Increased blasts and platelets in BM examination of initial diagnosis. C, D: Chromosomal aberrations revealed in cytogenetic analysis. E: FISH indicated the rearrangement between ABL and BCR genes. F: Bi-directional sequencing for confirmation of CALR 52-bp mutation. |
Discussion
We report the case of an untreated CML patient bearing p190 BCR/ABL transcript and CALR
52-bp deletion with additional chromosomal aberrations. The patient had
a dramatic thrombocytosis as well as high WBC count. Although rarely
reported, exclusive expression of e1a2BCR-ABL translocation is
associated with highly divergent clinical outcomes. Previous studies
suggest no relationship between distinct clinical presentations of CML
and type of BCR-ABL rearrangement[11] while many
others put them in a high-risk category at diagnosis with an early
transformation to blast phase similar to our patient.[12,13]
CMML-like
phenotype with monocytosis seems to be a useful diagnostic picture for
most cases of p190 BCR-ABL CML especially in chronic phase,[11]
but we advocate the consideration of more detailed analysis to prevent
any delay in therapeutic interventions for p190 blast crisis cases due
to lack of distinct clinical and biological features. Xu et al.
reviewed 17 cases of CML patients expressing p190 BCR-ABL oncoprotein
and JAK2V617F mutations who almost achieved a good response during treatment with tyrosine kinase inhibitors (TKIs).[14] This issue raises many questions about the presence of CALR mutation in p190 BCR-ABL CML and its likely impact on the clinical course and prognosis of our patient. So far, CALR mutation status has been associated with thrombocytosis in MPNs, including ET and PMF.[10] We believe that the presence of CALR
52-bp deletion in our CML case imparts the high platelet count and
ultimately mimics its progression toward cases other than CML in MPNs.
Since platelet count acts as a prognostic factor in the evaluation of
response to TKIs, we suggest the detection of CALR
mutation in all p190 BCR-ABL CML patients initially presenting with
thrombocytosis given the prognosis and treatment strategies in such
cases.[15] In summary, this interesting case illustrates that CALR
52-bp deletion may act as a distinctive feature in the diagnosis of
p190 BCR-ABLCML patients. Questions remain regarding the exact
contribution of CALR deletion to MPNs.
References

[TOP]