He was diagnosed with IgM-κ MM in October 2020 with complaints of waist pain. The initial workup revealed multiple bone destructions in the thoracolumbar vertebrae and appendages, bilateral ribs, and shoulder blades. Peripheral blood showed hemoglobin of 121 g/L, platelets of 131×109/L, white blood cell count of 5.49×109/L, serum creatinine of 96 μmol/L, and serum calcium of 2.78 mmol/L. Serum protein electrophoresis and immunofixation showed an IgM-kappa monoclonal protein (Figure 1A) with an M protein of 70.6 g/L. Serum kappa-light chain levels were elevated (1261 mg/L), and the kappa/lambda ratio was 157.3267. Urinary kappa light chains were 4225 mg/L, compared with lambda light chains of 5.9 mg/L. A bone marrow aspirate confirmed the presence of 60% plasma cells and a normal karyotype, 46, XY. Fluorescence in situ hybridization (FISH) analysis of the specimen showed immunoglobulin heavy chain (IGH) translocations t(11;14), del(17p), and 1q21 gain/amplification (Figure 1B, C, D). Finally, the patient was diagnosed with multiple myeloma IgM+κ type (D-S stage III, ISS stage II, R-ISS stage III).
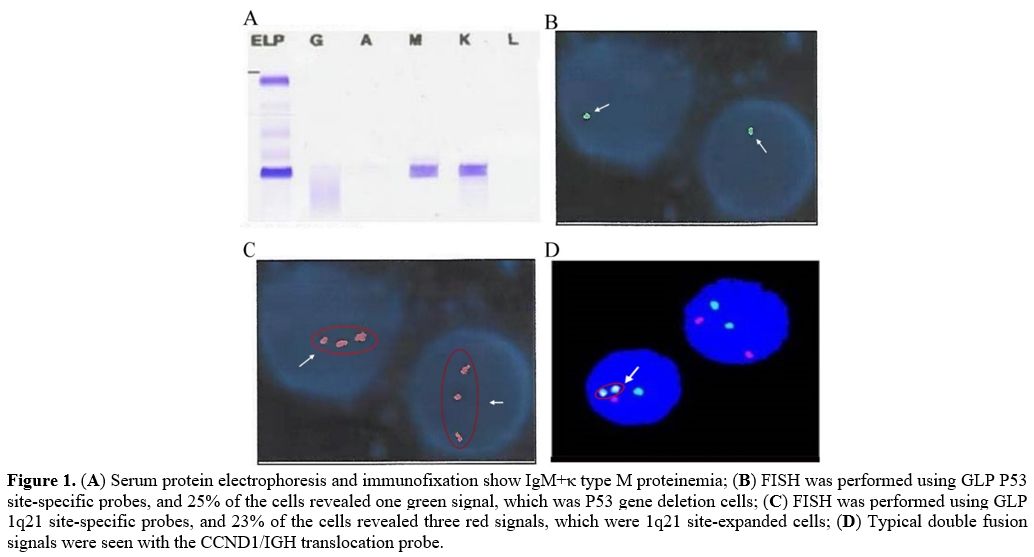 |
Figure
1. (A) Serum protein electrophoresis and immunofixation show IgM+κ type M proteinemia; (B)
FISH was performed using GLP P53 site-specific probes, and 25% of the
cells revealed one green signal, which was P53 gene deletion cells; (C)
FISH was performed using GLP 1q21 site-specific probes, and 23% of the
cells revealed three red signals, which were 1q21 site-expanded cells; (D) Typical double fusion signals were seen with the CCND1/IGH translocation probe. |
Considering the obvious symptoms of bone pain, the most common nonhematologic adverse reaction of bortezomib was peripheral neuropathy, and neuralgia side effects may exacerbate patient suffering. When the creatinine clearance rate was approximately 49 ml/(min*1.73 m2), bortezomib and lenalidomide were abandoned. Then, the patient started therapy with ixazomib 4 mg on Days 1, 8, and 15 plus dexamethasone 20 mg on Days 1, 8, 15, and 22. After some time on this regimen, he developed some rashes but did not pay attention to them. After two cycles of chemotherapy were completed, the creatinine clearance rate returned to normal, which allowed the use of lenalidomide. In pursuit of more effective treatment, an IRd regimen (ixazomib 4 mg on Days 1, 8, and 15 plus dexamethasone 15 mg on Days 1, 2, 8, 9, 15, 16, 22, and 23 with lenalidomide 25 mg/d) was planned to be implemented. Unfortunately, erythema and desquamation symptoms were further aggravated after four days of chemotherapy (Figure 2 A, B, C, D), which forced us to stop the treatment. In addition, a skin biopsy could not be performed due to severe skin lesions and exudation. After specialist symptomatic treatment, the skin peeling and exudation recovered (Figure 2 E, F). Because we were unsure which drug caused the skin peeling, we could no longer allow the patient to take ixazomib or lenalidomide continuously. Therefore, the treatment regimen was changed to pomalidomide and dexamethasone (PomDex) in the next cycle, with anti-platelet aggregation to prevent thromboembolism. During these two cycles, he did not have other skin lesions. In May 2021, bone marrow aspiration confirmed that abnormal proliferation of plasma cells increased to 35%. With a suboptimal response to PomDex, the addition of cyclophosphamide was expected to improve the response and outcomes further. In January 2022, we tried to add bortezomib from 1mg to 2mg, closely monitoring the skin reactions. The patient did not experience rash or skin peeling again. The treatment and review results of the patient are summarized in Figure 3.
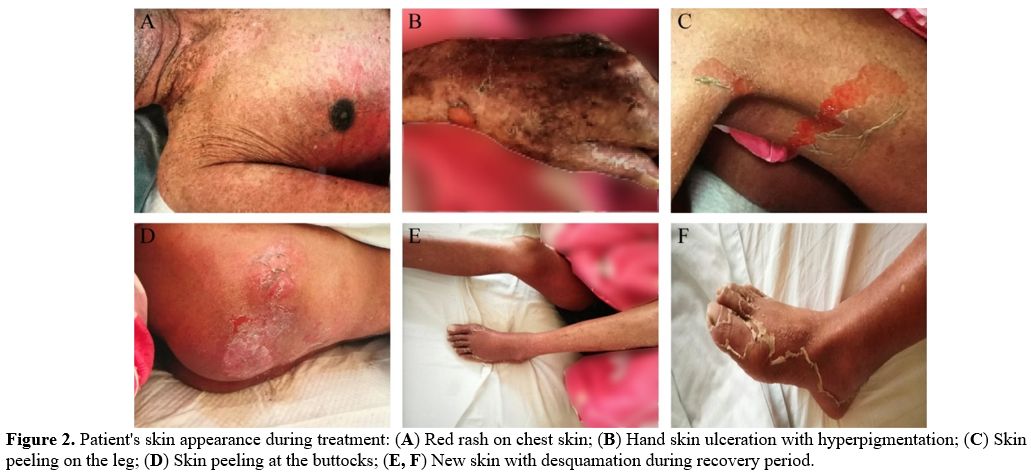 |
Figure 2. Patient's skin appearance during treatment: (A) Red rash on chest skin; (B) Hand skin ulceration with hyperpigmentation; (C) Skin peeling on the leg; (D) Skin peeling at the buttocks; (E, F) New skin with desquamation during recovery period. |
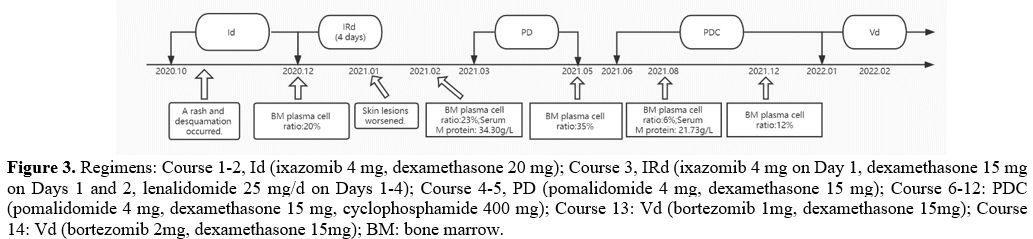 |
Figure 3. Regimens: Course 1-2, Id (ixazomib 4 mg, dexamethasone 20 mg); Course 3, IRd (ixazomib 4 mg on Day 1, dexamethasone 15 mg on Days 1 and 2, lenalidomide 25 mg/d on Days 1-4); Course 4-5, PD (pomalidomide 4 mg, dexamethasone 15 mg); Course 6-12: PDC (pomalidomide 4 mg, dexamethasone 15 mg, cyclophosphamide 400 mg); Course 13: Vd (bortezomib 1mg, dexamethasone 15mg); Course 14: Vd (bortezomib 2mg, dexamethasone 15mg); BM: bone marrow. |
According to the updated cytogenetic risk stratification criteria (including 2016 IMWG and 2018 mSMART 3.0), high-risk cytogenetic abnormalities (HRCAs) are defined as 1q amplification, del (17p), t (4; 14), t (14; 16) and t (14; 20). Recently, several foreign studies have proposed that a combination of various adverse prognostic factors leads to a worse prognosis and survival.[3] An unsatisfactory drug effect cannot exclude the existence of poor prognostic markers.
The cutaneous side effect profile of ixazomib remains to be documented. Kumar et al.[2] discussed the safety of ixazomib in patients with previously untreated myeloma. 17% of patients had skin and subcutaneous tissue disorders, including rash maculopapular, rash, rash pruritic, erythema, skin exfoliation, etc. In this case, the rash was considered due to ixazomib, the only new medication before the patient's skin manifestations. However, exacerbation of the rash caused by lenalidomide cannot be ruled out. The rash was observed with IRd, reflecting the overlapping character of the toxicity that has been seen with ixazomib alone[2] and with lenalidomide.[4,5] The rash observed with IRd typically ranges from limited erythematous, macular, and/or papular lesions that could be pruritic over a few body areas to a more generalized eruption predominantly on the trunk or extremities.[6] Most lenalidomide-related rashes are of mild-to-moderate severity and present as patchy, raised macular skin lesions, sometimes with localized urticaria and/or pruritus.[5] However, serious dermatological reactions, including Stevens-Johnson syndrome (SJS)[7,8] and toxic epidermal necrolysis (TEN),[8,9] have been reported with lenalidomide. For the aggravation of skin lesions that occurred 4 days after starting IRd, the cutaneous adverse reactions of lenalidomide may have a certain boosting effect, with ixazomib playing a leading role.
Both ixazomib and bortezomib are proteasome inhibitors, but cross-allergic reactions may not necessarily occur, which has a clinical significance for drug use. Also, it is important to monitor the skin response after treatment with IRd. Recognizing and identifying cutaneous adverse events allows for early intervention and management while achieving continuous and effective treatment.