.
Guiping Liao1#, Changqing Wei1#, Qiuying Huang1, Manlv Wei1, Jing Li2, Yaopeng Chen2 and Xiaolin Yin1*
1
Department of Hematology, The 923rd Hospital of the Joint Logistics
Support Force of the People's Liberation Army, Nanning, China.
2
Department of Blood Transfusion, The 923rd Hospital of the Joint
Logistics Support Force of the People's Liberation Army, Nanning, China
#Those authors equally contributed to this work.
Correspondence to:
Xiaolin
Yin, Department of Hematology, The 923rd Hospital of the Joint
Logistics Support Force of the People's Liberation Army, Nanning,
Guangxi, China; E-mail:
yin-xl@163.com
Published: July 01, 2024
Received: June 05, 2024
Accepted: June 26, 2024
Mediterr J Hematol Infect Dis 2024, 16(1): e2024050 DOI
10.4084/MJHID.2024.050
This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by-nc/4.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
To the editor
A
prerequisite for a successful allogeneic hematopoietic stem cell
transplantation (HSCT) is the availability of a human leukocyte antigen
(HLA) identical stem cell donor. Due to the fact that the HLA system is
inherited independently of the blood group system, approximately 40–50%
of all HSCTs are performed across the ABO blood group barrier.[1,2]
The expected immune-hematological consequences after transplantation of
an ABO-mismatched stem cell graft are immediate and delayed hemolytic
complications due to presence of isohemagglutinins or passenger
lymphocyte syndrome (PLS).[3] The risks of these
complications can partially be prevented by graft manipulation and
appropriate transfusion support. Here, we report a rare case of
haploidentical HSCT in which a donor’s residual high-titer anti-A
antibody induced intravascular hemolysis and hyperbilirubinemia during
group O RBC transfusion during the blood group transition phase.
An
11-year-old boy was undergoing treatment with dasatinib for chronic
myeloid leukemia, onset May 2022. He subsequently underwent acute
transformation, and allogeneic peripheral stem cell transplantation
from a HLA 5/10-matched donor with ABO incompatibility was performed at
our medical center in September 2023. The patient and donor blood
groups were A positive and O positive, respectively. The boy was
treated with a myeloablative conditioning regimen consisting of
fludarabine, busulfan, and melphalan, and a graft-versus-host disease
(GVHD) prevention and treatment scheme including post-transplant
cyclophosphamide, methotrexate, cyclosporine, and anti-lymphocyte
immunoglobulin. The nucleated cell dose infused was 11.8 × 108/kg and the CD34+ cell dose was 8.5 × 106/kg.
On
day 6 post-transplantation, the patient’s hemoglobin was 63 g/L (normal
range, 120–150 g/dL) and he therefore received a transfusion of 2 units
of red blood cells (RBCs) with type O-filtered leukocytes, after which
he developed fever and hemolysis. Routine blood tests and serum
biochemical tests revealed hemoglobin, 54 g/L; total bilirubin (TBIL),
71.8 μmol/L (normal range, 0–23 μmol/L); direct bilirubin (DBIL), 24.4
μmol/L (normal range, 5–18 μmol/L); indirect bilirubin (IBIL), 47.4
μmol/L (normal range, 5–18 μmol/L); alanine aminotransferase (ALT), 656
U/L (normal range, 7–40 U/L); aspartate aminotransferase (AST), 802 U/L
(normal range, 13–35 U/L); and lactate dehydrogenase (LDH), 1255 U/L
(normal range, 114–240 U/L). Blood analysis at day 8
post-transplantation showed a further drop in hemoglobin to 37 g/L.
Coombs test was positive. The anti-A isohemoagglutitin titer of the
blood donor was >1:1080. Intravascular hemolytic anemia was
considered with elevated bilirubin and aminotransferases caused by
hemolysis, and hydration, alkalinization, diuretic therapy, and type O
washed RBC transfusion were administered, after which the patient’s
hemoglobin gradually increased to 94 g/L. Serum biochemical tests at
day 10 post-transplantation showed TBIL, 259.7 μmol/L; DBIL, 190.4
μmol/L; IBIL, 69.3 μmol/L; ALT, 1092 U/L; AST, 1068 U/L; and LDH, 2494
U/L (Figure 1).
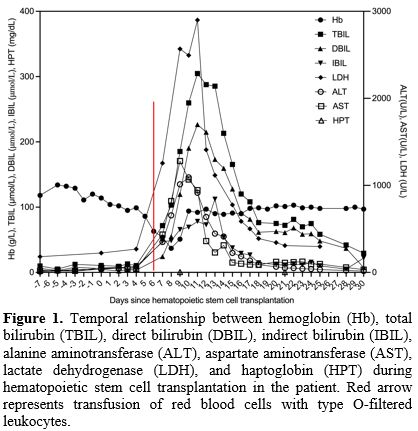 |
- Figure 1. Temporal
relationship between hemoglobin (Hb), total bilirubin (TBIL), direct
bilirubin (DBIL), indirect bilirubin (IBIL), alanine aminotransferase
(ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH),
and haptoglobin (HPT) during hematopoietic stem cell transplantation in
the patient. Red arrow represents transfusion of red blood cells with
type O-filtered leukocytes.
|
Hepatic
veno-occlusive disease, sinusoidal obstruction syndrome, thrombotic
microangiopathy, and viral infections were excluded. His bilirubin and
transaminase levels gradually decreased to normal after treatment with
anti-thymocyte immunoglobulin and basiliximab. The boy had full donor
chimerism of 99.8% at day 28 post-transplantation.
Decreased
hemoglobin levels are a common complication after transplantation with
secondary blood group antigen incompatibility, and may be associated
with PLS. PLS is caused by the transfer of B-lymphocytes present in the
donor graft into the recipient circulation following HSCT.[4]
These cells may produce antibodies against the recipient’s RBCs,
thereby triggering antibody-dependent cytotoxicity and erythroid
clearance, with potential resulting hemolysis and jaundice.[4]
ABO and Rh antibodies are the most common antibodies identified in PLS,
with a type O donor and type A recipient posing the greatest risk of
hemolysis, as in the current patient.[5] Ambulatory monitoring of blood group antibody titers can aid patient monitoring and diagnosis.[6]
The disease is self-limiting and does not require special treatment,
but RBC transfusions may be given in cases of severe anemia. During the
transition phase, transfusion of type O RBCs or recipient RBCs is
recommended for ABO-incompatible transplants.[7] In
the present case, the patient developed intravascular hemolytic anemia
after transfusion of type O RBCs, and it was considered that a small
amount of residual plasma during RBC preparation contained high-titer
anti-A antibodies, which combined with the patient’s own group A RBCs
by an acute hemolytic reaction. The patient’s hemolysis did not worsen
after the transfusion of type O washed RBCs and his hemoglobin level
increased.
Although the patient’s hemolysis resolved and
hemoglobin increased, his bilirubin tended to remain stable; however,
there was a rapid rise in bilirubin, predominantly direct bilirubin, at
day 10 post-transplantation. There was no significant change in the
patient’s weight at this time and platelet transfusions were effective,
which were not consistent with veno-occlusive disease/sinusoidal
obstruction syndrome.[8] Although the patient had
intravascular hemolysis, he had no symptoms such as hypertension,
fragmented RBC, proteinuria, or worsening renal failure, and therefore
did not meet the diagnostic criteria for thrombotic microangiopathy.[9]
Viral tests, including hepatitis B virus, hepatitis C virus,
cytomegalovirus, and Epstein-Barr virus were all negative, and viral
infection was therefore not considered. However, his bilirubin and
aminotransferase levels decreased rapidly after treatment with
anti-thymocyte immunoglobulin and basiliximab, indicating the
possibility of hepatic aGVHD. The blood group-associated antigens are
expressed, not only in RBC membranes, but also in other tissues. Blood
group-associated antigens are widely distributed in intrahepatic and
extrahepatic epithelial cells and hepatocytes, and may be adequate to
induce rejection.[10] It follows the development of severe hyperbilirubinemia during HSCT may be caused by a combination of the factors.
Conclusions
Hemoglobin
and blood group antibody titers need to be measured after HSCT with
minor blood group incompatibility, to allow the early detection of PLS.
If the recipient’s hemoglobin levels decrease, requiring blood
transfusion, washed RBCs should be used where possible to avoid the
introduction of antibodies. In the event of increased bilirubin and
abnormal liver function, it is necessary to be vigilant for aGVHD and
to implement early intervention and control as soon as possible.
Acknowledgements
This
study was financially supported by the Scientific Research Project of
Guangxi Zhuang Autonomous Region Health Committee (Z-A20231086) and the
Scientific Research Fund Project of Guangzhou City Life Oasis Public
Welfare Service Center (GZLZ-HEMA-008).
Informed Consent
Informed consent was obtained from the participant included in the study.
References
- Akkok CA, Seghatchian J. Immunohematologic issues
in ABO-incompatible allogeneic hematopoietic stem cell transplantation.
Transfus Apher Sci. 2018;57:812-5. https://doi.org/10.1016/j.transci.2018.10.020 PMid:30404742
- Worel N, Kalhs P. AB0-incompatible allogeneic hematopoietic stem cell transplantation. Haematologica. 2008;93:1605-7. https://doi.org/10.3324/haematol.2008.001057 PMid:18978296
- Worel N. ABO-Mismatched Allogeneic Hematopoietic Stem Cell Transplantation. Transfus Med Hemother. 2016;43:3-12. https://doi.org/10.1159/000441507 PMid:27022317 PMCid:PMC4797460
- Moosavi
MM, Duncan A, Stowell SR, Roback JD, Sullivan HC. Passenger Lymphocyte
Syndrome; a Review of the Diagnosis, Treatment, and Proposed Detection
Protocol. Transfus Med Rev. 2020;34:178-87. https://doi.org/10.1016/j.tmrv.2020.06.004 PMid:32826130
- Peck
JR, Elkhammas EA, Li F, Stanich PP, Latchana N, Black S, Michaels A.
Passenger lymphocyte syndrome: a forgotten cause of postliver
transplant jaundice and anemia. Exp Clin Transplant. 2015;13:200-2.
- Teshigawara-Tanabe
H, Hagihara M, Matsumura A, Takahashi H, Nakajima Y, Miyazaki T, Kamijo
A, Yamazaki E, Fujimaki K, Matsumoto K, Nakajima H. Passenger
lymphocyte syndrome after ABO-incompatible allogeneic hematopoietic
stem cell transplantation; dynamics of ABO allo-antibody and blood type
conversion. Hematology. 2021;26:835-9. https://doi.org/10.1080/16078454.2021.1986654 PMid:34672906
- Shokrgozar
N, Tamaddon G. ABO Blood Grouping Mismatch in Hematopoietic Stem Cell
Transplantation and Clinical Guides. Int J Hematol Oncol Stem Cell Res.
2018;12:322-8. https://doi.org/10.18502/ijhoscr.v12i4.112 PMid:30774834 PMCid:PMC6375375
- Ruutu
T, Peczynski C, Houhou M, Polge E, Mohty M, Kroger N, Moiseev I, Penack
O, Salooja N, Schoemans H, Duarte RF, Schroeder T, Passweg J, Wulf GG,
Ganser A, Sica S, Arat M, Salmenniemi U, Broers AEC, Bourhis JH,
Rambaldi A, Maertens J, Halaburda K, Zuckerman T, Labussiere-Wallet H,
Basak G, Koenecke C, Peric Z. Current incidence, severity, and
management of veno-occlusive disease/sinusoidal obstruction syndrome in
adult allogeneic HSCT recipients: an EBMT Transplant Complications
Working Party study. Bone Marrow Transplant. 2023;58:1209-14. https://doi.org/10.1038/s41409-023-02077-2 PMid:37573397 PMCid:PMC10622315
- Nusrat
S, Davis H, MacDougall K, George JN, Nakamura R, Borogovac A.
Thrombotic Microangiopathy After Hematopoietic Stem Cell and Solid
Organ Transplantation: A Review for Intensive Care Physicians. J
Intensive Care Med. 2024;39:406-19. https://doi.org/10.1177/08850666231200193 PMid:37990516
- Nakanuma
Y, Sasaki M. Expression of blood group-related antigens in the
intrahepatic biliary tree and hepatocytes in normal livers and various
hepatobiliary diseases. Hepatology. 1989;10:174-8. https://doi.org/10.1002/hep.1840100209 PMid:2744729