Vietnam, located in Southeast Asia and sharing borders with Laos, Cambodia to the West, and China to the North, lies within the ‘thalassemia belt’ where the disease is highly endemic. A national survey in 2017 estimated a carrier prevalence of 13.8%.[6] As of 2024, the country’s population was approximately 105.7 million, comprising 54 officially recognized ethnic groups.[7] The majority Kinh group (85.3%) predominantly inhabit lowland regions, while ethnic minorities such as the Thai, Muong, Tay, and Nung (14.7%) are concentrated in upland and mountainous areas, which often face challenges in healthcare accessibility.[7-9] Northern Vietnam, encompassing the Red River Delta, the Northeast, the Northwest, and the North Central, presents pronounced diversity in socioeconomic, cultural, and environmental conditions, making it a relevant setting for epidemiological investigation.
The Thalassemia Center at the National Institute of Hematology and Blood Transfusion, Vietnam (NIHBT) is the largest treatment facility for Thalassemia in Northern Vietnam, providing care to over 4,000 patients and delivering around 20,000 treatment visits annually. Despite advances in clinical management, molecular diagnostics, and prenatal screening, disease control remains limited in remote areas and among ethnic minorities, as evidenced by the continued birth of affected children each year. While several studies have reported carrier rates across different ethnic groups in Vietnam, data on clinical characteristics, particularly among pediatric patients, remain scarce.[6] This study, therefore, aims to describe the prevalence of Thalassemia among children from various ethnicities and regions in Northern Vietnam to support genetic counseling and targeted prevention strategies.
Methods
Study design and setting. This retrospective descriptive study was conducted at the Thalassemia Center, a national tertiary referral institution in Vietnam. The study cohort comprised 1,240 children diagnosed with Thalassemia who were younger than 10 years at the time of their initial treatment at the NIHBT between January 01, 2014, and December 31, 2023. Demographic, clinical, and laboratory data were collected retrospectively. Data analysis and study implementation were carried out at the same center from June 2024 to May 2025.Study subjects. During the study period, all patients who satisfied the inclusion criteria were consecutively enrolled without the use of sampling methods. The eligible cohort comprised children diagnosed with any subtype of Thalassemia, including α-thalassemia, β-thalassemia, and β-thalassemia/HbE, before reaching 10 years of age, who commenced treatment at the Thalassemia Center within the specified timeframe. Patients with incomplete or missing medical records were excluded from the study.
Data Collection and Variables. Data were retrospectively extracted from paper-based case files and the hospital’s electronic database. Demographic and clinical variables were collected using a standardized template by two independent investigators to ensure accuracy, with data verification and cleaning performed by a designated member of the research team. All records were anonymized and encrypted before statistical processing.
The demographic characteristics included:
• Year of birth: recorded according to the Gregorian calendar. This variable was used to determine the age at first treatment and the timing of treatment initiation at NIHBT.
• Sex: classified as male or female.
• Ethnicity: obtained from administrative records, including the Kinh majority and ethnic minority groups such as Tay, Thai, Muong, ...
• Place of residence: derived from the administrative information registered at the institute and categorized according to the geographical regions of Vietnam.
The clinical characteristics included:
• Age at treatment initiation: was defined as the age at the first blood transfusion, calculated in months from birth to treatment. For comparison across age groups, ages for children younger than 6 years (originally recorded in months) were converted to years (12 months = 1 year).
• Thalassemia subtype: This study population was classified into three groups: α-thalassemia, β-thalassemia, and β-thalassemia/HbE based on hemoglobin electrophoresis (measured using high-performance liquid chromatography on the Ultra2 system- Trinity Biotech Branch) and genetic testing results (identified using polymerase chain reaction (PCR) and Sanger sequencing). PCR assays, adapted from the Thalassaemia International Federation (TIF) guidelines, were used to identify population-specific common variants.[10] Samples that tested negative or carried only a single heterozygous variant were subjected to comprehensive Sanger sequencing using the AB3500 Genetic Analyzer (Thermo Fisher Scientific, USA), with the BigDye Terminator v3.1 Kit and DyeEx 96 Kit (QIAGEN, Germany). Sequencing data analysis and variant calling were performed using CLC Genomics Workbench version 20 (QIAGEN, Germany). The variant analysis was specifically directed toward the HBA1, HBA2, and HBB genes, concerning the transcript sequences NM_000558.3, NM_000517.4, and NM_000518.4, respectively. Nomenclature of identified variants at both the cDNA (c.) and protein (p.) levels was assigned following the recommendations of the Human Genome Variation Society (HGVS).
Data analysis. Categorical variables, including sex, ethnicity, place of residence, disease subtype, and genetic variants, were summarized as frequencies and percentages (%). The variables of average age and age at treatment initiation were presented as medians with their ranges. An area chart was used to illustrate the distribution of age at treatment initiation; a boxplot was employed to describe the characteristics of the mean age at treatment initiation; and stacked bar charts were used to present the distribution of disease subtypes by ethnicity and place of residence.
This study was exclusively descriptive; therefore, no inferential statistical analyses were performed. All analyses and data visualizations were performed using SPSS software (version 16.0; SPSS Inc., Chicago, IL, USA).
Ethical considerations. The study was approved by the institutional medical research ethics committees of the National Institute of Hematology and Blood Transfusion (Vietnam; approval No. 964/QD-HHTM, dated July 25, 2025).
Results
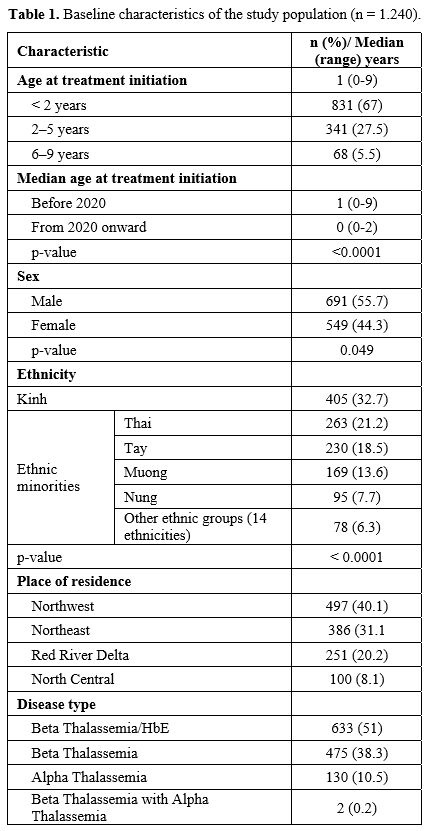
Baseline characteristics of the study population. The demographic characteristics of the study cohort are presented in Table 1. The median age at treatment initiation was 1 year, with most patients starting therapy before age 2. Notably, children born from 2020 onward were diagnosed and treated earlier compared to those born before 2020 (0 vs. 1 year, p < 0.0001). The majority of Thalassemia patients in this cohort belonged to ethnic minority groups. Four groups (Thai, Muong, Tay, and Nung) comprised 61% of the study population. The proportion of Kinh patients was 32.7%, despite the Kinh accounting for more than 85% of Vietnam’s population.[7,8]Most patients resided in mountainous regions, mainly the Northwest (40.1%) and Northeast (31.1%). The predominant subtypes were Beta Thalassemia/HbE (51%) and Beta Thalassemia (38.3%). Alpha Thalassemia accounted for 10.5% of cases (Table 1).
 |
|
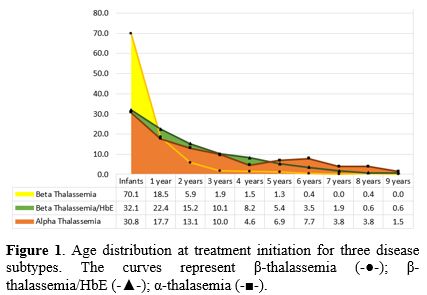
Age at onset of treatment. The distribution of Thalassemia subtypes among pediatric patients aged 0–9 years was shown in Figure 1. Most Thalassemia cases were diagnosed early, with the highest prevalence observed in children under one year of age, followed by a gradual decline with increasing age, particularly among those with Beta Thalassemia. This group was markedly predominant in the under one-year-of-age category (70.1%), and 94.5% of these patients were aged from 0 to 2 years. Among patients with Beta Thalassemia/HbE, 54.5% began transfusions before age 2, while 42.4% initiated transfusions between ages 2 and 6. The proportion of Alpha Thalassemia patients who initiated treatment before age 1 was relatively high (30.8%).
 |
|
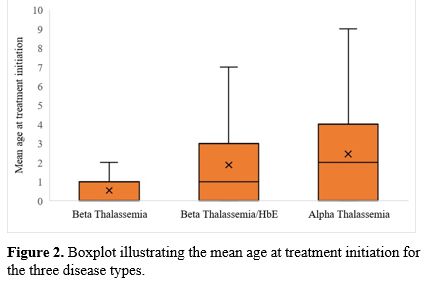
The mean age at treatment initiation varied substantially among the three Thalassemia subtypes (Figures 1 and 2). In the Beta Thalassemia group, 88.6% of patients began treatment before age 2, with a mean age of 0.54 years. Among those with Beta Thalassemia/HbE, 93.4% initiated treatment at or before 5 years of age, with a mean age of 1.88 years. In the Alpha Thalassemia group, 90.9% of patients initiated treatment before age 7, with a mean age at treatment initiation of 2.45 years. The difference in age at treatment initiation between the Beta Thalassemia group and the other two subtypes was statistically significant (p < 0.0001). Additionally, the mean age at treatment initiation also differed significantly between the Beta Thalassemia/HbE and Alpha Thalassemia groups (p = 0.00012).
 |
|
Distribution of Thalassemia subtypes by ethnicity and place of residence. In Figures 3 and 4, ethnic groups and geographic regions with larger patient populations were highlighted. Ethnic groups with fewer than 30 patients were not presented due to their limited representativeness; they included 29 Dao patients, 10 San Diu patients, 4 Tho patients, and 3 San Chay patients. The Cao Lan, Giay, Kho Mu, and La Ha groups each comprised 6 patients, while the Khang and H’Mong groups each had two patients. The Kho Me, Hoa, Lao, and Xinh Mun groups each accounted for one patient. For the analysis of distribution by place of residence, only four main regions were considered: The Northeastern, Northwestern, Red River Delta, and North Central regions. Two cases of Beta Thalassemia combined with Alpha Thalassemia were excluded due to their very low number, to maintain the completeness of the dataset.
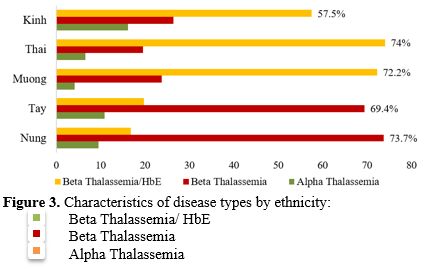 |
Figure 3. Characteristics of disease types by ethnicity |
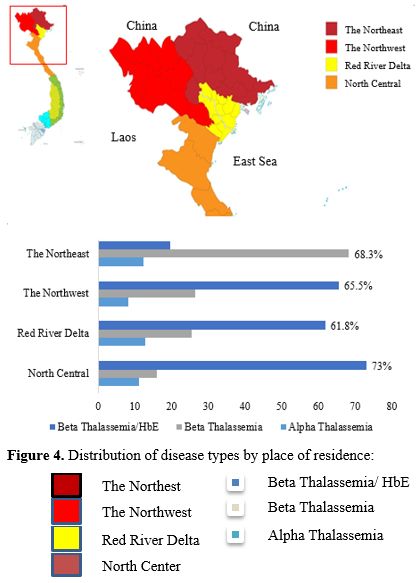 |
Figure 4. Distribution of disease types by place of residence |
The analysis revealed a marked variation in the distribution of Thalassemia subtypes across ethnic groups and geographic regions. Beta Thalassemia/HbE was predominant among the Kinh, Thai, and Muong ethnic groups, particularly in the Thai and Muong populations, whereas Beta Thalassemia was more common among the Tay and Nung groups (Figure 3). The Northeastern region had the highest proportion of Beta Thalassemia cases, accounting for 68.3%. In contrast, Beta Thalassemia/HbE was more prevalent in the Northwestern, Red River Delta, and North Central regions, with the highest proportion observed in the North Central region (73%). Alpha Thalassemia was present across all ethnic groups and geographic regions, accounting for the lowest proportion (Figure 4).
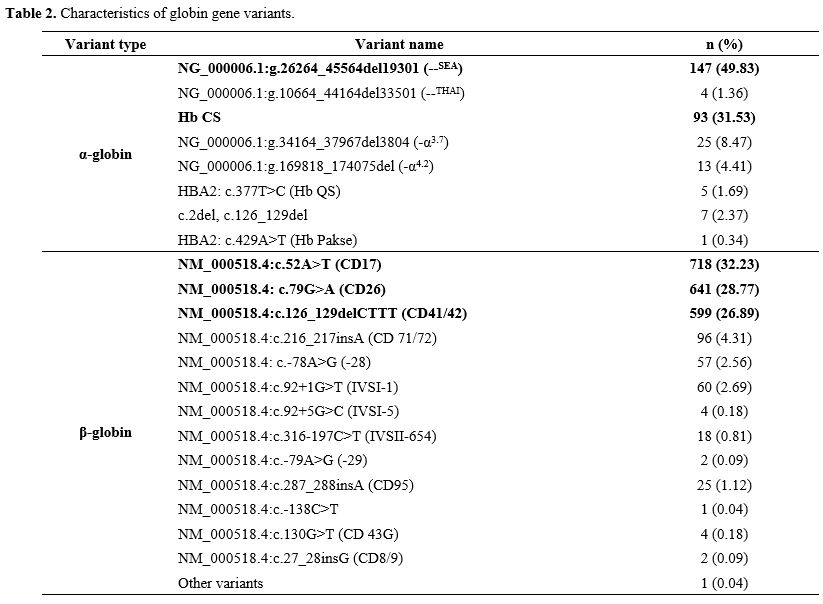
Characteristics of globin gene variants. Data from 1,240 Thalassemia patients were grouped into seven clinical groups: Alpha Thalassemia, Alpha Thalassemia combined with Beta Thalassemia, Alpha Thalassemia with HbE, Beta Thalassemia, Beta Thalassemia/HbE, and Beta Thalassemia or Beta Thalassemia/HbE carrying co-inherited alpha-globin gene variants. A total of 2,523 mutated alleles were identified, including 295 α-globin gene variants and 2,228 β-globin gene variants, with eight α-globin and thirteen β-globin mutated types being detected. These types were represented in Table 2.
Among α⁰-globin alleles, the --SEA deletion was predominant (49.83%), whereas the --THAI deletion was rare (1.4%). The α⁺-α-globin variants mainly comprised Hb CS (31.53%), while small deletions (-α3.7 and -α4.2) were less frequent (12.88%). Other rare variants, including Hb QS, c.2delT, and Hb Pakse, just accounted for 4.4% (Table 2).
For the β-globin gene, the majority of variants were point mutations. β⁰-globin variants (abolishing β-globin chain production); including Codon 17 (A>T), Codon 41/42 (-TTCT), Codon 71/72 (+A), IVSI-1 (G>T), IVSI-5 (G>C), CD95, CD43, and Codon 8/9 (+G); accounted for 67.69% of all β-globin variants. The structural variant HbE (CD26) was also highly prevalent (28.77%). Additionally, a small proportion of β⁺-globin variants, such as –28 (A>G), –29 (A>G), IVSII-654 (C>T), and c.-138 (C>T), was observed.
 |
|
Discussion
Thalassemia is a genetic disorder caused by variants that disrupt the synthesis of globin chains. The severity of this condition can vary significantly based on the specific genetic mutations and their combinations. An analysis of 1,240 children with Thalassemia under age 10 at NIHBT (Table 1) revealed that treatment typically commenced at a young age, with a median age of initiation of 1 year. Notably, 94.5% of these patients began treatment before age 6, and 67% were diagnosed within the first 2 years of life. A comparison between children born before 2020 and those born in 2020 or later revealed a discernible trend of earlier diagnosis and intervention in more recent birth cohorts. Children born after 2020 initiated treatment at a median age of 0 years (range 0-2 years), compared to a median age of 1 year (range 0-9 years) for those born earlier (p < 0.0001). This shift is likely associated with Decision No. 1807/QD-BYT in Vietnam (2020),[11] which includes Thalassemia in the list of conditions to be screened and diagnosed during the first trimester of pregnancy. The implementation of this regulation, along with coordinated efforts by national health authorities to raise community awareness and expand screening programs, has contributed to increased recognition and early detection of Thalassemia across Vietnam.Upon closer examination of age at treatment initiation across the various disease subgroups, a pronounced disparity emerges. β-Thalassemia requires the earliest initiation, typically within the first year of life, reflecting its more severe clinical manifestations. The proportion of Alpha Thalassemia patients initiating treatment before age 1 was not low (30.8%), likely attributable to the study population consisting predominantly of moderate-to-severe Alpha Thalassemia cases. However, when considering the entire study cohort (n=1240), the proportion of Alpha Thalassemia patients who required a transfusion before 1 year of age was small, at approximately 3.2%. In other words, α-Thalassemia was characterized by a later and more variable onset. β-Thalassemia/HbE occupied an intermediate position between the two types (Figures 1 and 2).
Following the analysis of the age at treatment initiation, the examination of geographical and ethnic characteristics further contributes to elucidating the overall profile of the study population. Northern Vietnam can be divided into several major regions, including the Northeast, which borders Guangxi Province of China to the North; the Northwest and North Central regions, both adjoining Laos to the west; and the Red River Delta in the heart. Analysis of Table 1, Figure 3, and Figure 4 revealed marked differences in the distribution of Thalassemia genotypes across geographical areas and ethnic groups. Notably, Beta Thalassemia/HbE was highly concentrated in the North Central region (73%) and the Northwest (65.5%), making these areas epidemiologically "hotspots" for this type. These findings are consistent with the genetic background of the two regions, which not only share geographical proximity through land borders with Laos, where the HbE carrier rate is extremely high (50–60%),[12] but also are home to ethnic minorities with elevated carrier frequencies.[13-15] Beyond geography, ethnicity plays a critical role. The Thai and Muong, the predominant ethnic groups in the North Central region, exhibit high HbE carrier rates of 18.7% and 17.9%, respectively.[13] These groups also demonstrate the highest prevalence of the Beta Thalassemia/HbE genotype, with 74% among the Thai and 72.2% among the Muong. Collectively, these findings highlight that the interaction of geographical factors, cross-border genetic exchange, and ethnic-specific mutation patterns plays a critical role in shaping the unique distribution of β-Thalassemia/HbE in Vietnam.
While Beta Thalassemia/HbE clustered in the North Central and Northwest regions, Beta Thalassemia was predominantly observed in the Northeast, accounting for 68.3% of cases. The disease was particularly concentrated among the Tay (69.4%) and Nung (73.7%) ethnic groups. Notably, within the Dao group, although only 29 patients were included, 72.4% were affected. The Dao are a major ethnic population in the Northeast,[13] and the β0-globin carrier frequency among this group has been reported to be relatively high (9.3%).[16] However, in the present study, the number of Dao patients was considerably lower than expected; owing to insufficient data on globin mutations, this group was not included in the analysis. Future studies with more comprehensive data are needed to provide a more objective understanding of Thalassemia in the Dao community. Beyond the Dao, comparison with data on Thalassemia carrier status among ethnic groups in the Northeastern region of Vietnam demonstrates a clear consistency between the distribution of clinical phenotypes and carrier profiles within the community. Notably, the Tay and Nung populations exhibit relatively high carrier frequencies for the β0-globin gene (6.2% and 5.5%, respectively),[16] reflecting both increased hereditary risk and a higher disease burden. Importantly, this region shares borders with Guangxi, China, where the prevalence of Thalassemia carriers has also been reported to be high. A large-scale study in Guangxi in 2021 involving 71,459 children (1–10 years old) identified a carrier rate of 16.54% (11,821 children), including 4.9% carriers of the β-thalassemia gene, predominantly with CD41/42, CD17, CD71/72, and -28 mutations.[17] Comparable findings have been reported in neighboring Southeast Asian countries. In Thailand, β-thalassemia carrier frequencies range from 3–9%,[18] with CD41/42 and CD17 being the dominant mutations, and Hb E being widely prevalent.[18-20] In Laos, similar β-globin mutation patterns (CD17, CD41/42, CD71/72) have been observed, with Hb E carriers comprising up to half of some ethnic groups.[21] Together with data from Guangxi, these findings indicate a continuous thalassemia-endemic zone spanning southern China, northern Vietnam, Laos, and Thailand, highlight the epidemiological similarities between neighboring regions, and further reinforce the association between geographical and demographic factors and the epidemiology of Thalassemia.
Although the Kinh ethnic group accounted for the largest proportion of patients overall (32.7%), their prevalence of β-thalassemia or β-thalassemia/HbE was lower than that of ethnic minorities such as the Thai, Muong, Tay, and Nung. This distribution reflects the epidemiological pattern of Thalassemia carriers in Vietnam, particularly among ethnic minority communities in the northern mountainous regions (the Northeast and Northwest regions), where carrier frequencies remain high due to genetic predisposition and the marriage practices.[22] In addition, the majority of patients are concentrated in northern mountainous provinces, which are characterized by limited availability of healthcare services and socioeconomic hardship.[23] The disproportionate burden observed in these areas is not only shaped by genetic risk but also perpetuated by socio-cultural determinants, notably early marriage and consanguinity, which together reinforce the high prevalence of Thalassemia in these communities. According to Vietnam News, “20–40% of Thalassemia carriers belong to ethnic minority groups”.[24] This situation underscores the significant hereditary risk and highlights the urgent need for targeted health communication, genetic counseling, and early, focused carrier screening programs, particularly within high-risk ethnic minority populations.
Based on our findings highlighting the influence of ethnicity and geography on thalassemia epidemiology, we recommend developing tailored public health interventions, including targeted genetic counseling and community-based education, particularly for high-risk ethnic groups in Northern Vietnam. Future studies should further characterize mutation spectra and assess community-based screening strategies to inform precision public health efforts.
Conclusions
In children under 10 years of age treated at the NIHBT, β-Thalassemia and β-Thalassemia/HbE accounted for 89.3% of all cases. The prevalence was notably higher among ethnic minorities in the northern mountainous regions, highlighting the critical need for targeted genetic counseling, early carrier screening, and community-based education to mitigate disease incidence in high-risk populations.Limitations
This study may have been influenced by referral bias, a specific form of selection bias, as the data were collected exclusively from the Thalassemia Center at the NIHBT, the premier hematology facility in Vietnam's healthcare system. Patients referred to this center are predominantly from northern provinces. They are more likely to present with severe or complicated disease, whereas milder cases may continue to receive care at provincial or district hospitals. Although the exact proportion of patients treated outside the NIHBT is not available, such referral patterns may limit the generalizability of our findings to all individuals with Thalassemia in northern Vietnam.Author contributions
Ha Thanh Nguyen, Ngoc Dung Nguyen, and Thi Thu Ha Nguyen contributed to the study conception and design. Phuong Linh Hoang, Thi Chi Nguyen, Thi Nguyet Anh Phi, and Thi Thu Huyen Le were responsible for data collection. Ha Thanh Nguyen, Ngoc Dung Nguyen, and Duc Binh Vu performed data analysis and literature review. Ngoc Dung Nguyen and Thi Chi Nguyen contributed to the discussion and conclusions. Thi Chi Nguyen and Thi Nguyet Anh Phi were involved in drafting the manuscript. All authors read and approved the final version of the manuscript.Ethics statement
The study was conducted with the approval of the NIHBT administration and the Thalassemia Center. All data were collected solely for research purposes and were anonymized to ensure the confidentiality of patient information.Acknowledgments
The authors express their sincere gratitude to the National Institute of Hematology and Blood Transfusion, Vietnam, and all physicians and nurses at the Thalassemia Center for their support during patient data collection.References
- E. S. Soteriades and D. Weatherall, "The
Thalassemia International Federation: A Global Public Health Paradigm,"
Thalassemia Reports, vol. 4, no. 2, Art. no. 2, Sep. 2014. https://doi.org/10.4081/thal.2014.1840
- S.
Soteriades, M. Angastiniotis, D. Farmakis, A. Eleftheriou, and A.
Maggio, "The Need for Translational Epidemiology in Beta Thalassemia
Syndromes: A Thalassemia International Federation Perspective,"
Hematology/Oncology Clinics of North America, vol. 37, no. 2, pp.
261-272, Apr. 2023. https://doi.org/10.1016/j.hoc.2022.12.011 PMid:36907602
- S.
Fucharoen and P. Winichagoon, "Haemoglobinopathies in Southeast Asia,"
Indian J Med Res, vol. 134, no. 4, pp. 498-506, Oct. 2011.
- B.
Modell and M. Darlison, "Global epidemiology of haemoglobin disorders
and derived service indicators," Bull World Health Organ, vol. 86, no.
6, pp. 480-487, Jun. 2008. https://doi.org/10.2471/BLT.06.036673 PMid:18568278 PMCid:PMC2647473
- D.
J. Weatherall and J. B. Clegg, "Inherited haemoglobin disorders: an
increasing global health problem," Bull World Health Organ, vol. 79,
no. 8, pp. 704-712, 2001.
- K.
Q. Bach, H. T. T. Nguyen, T. H. Nguyen, M. B. Nguyen, and T. A. Nguyen,
"Thalassemia in Viet Nam," Hemoglobin, vol. 46, no. 1, pp. 62-65, Jan.
2022. https://doi.org/10.1080/03630269.2022.2069032 PMid:35950578
- "Country Factsheet," The World Factbook. Central Intelligence Agency. Accessed: August 17, 2025. [Online]. Available: https://www.cia.gov/the-world-factbook/countries/vietnam/factsheets/
- "Press
Release: Preliminary results of the 2019 Population and Housing
census," National Statistics Office of Vietnam. Accessed: August 17,
2025. [Online]. Available: https://www.nso.gov.vn/en/data-and-statistics/2019/10/press-release-preliminary-results-the-2019-population-and-housing-census/
- "Completed
results of the 2019 Viet Nam population and housing census," National
Statistics Office of Vietnam. Accessed: August 17, 2025. [Online].
Available: https://www.nso.gov.vn/en/data-and-statistics/2020/11/completed-results-of-the-2019-viet-nam-population-and-housing-census/
- J.
Old, C. L. Harteveld, J. Traeger-Synodinos, M. Petrou, M.
Angastiniotis, and R. Galanello, Prevention of Thalassaemias and Other
Haemoglobin Disorders: Volume 2: Laboratory Protocols, 2nd ed. Nicosia
(Cyprus): Thalassaemia International Federation, 2012. Accessed: August
02, 2025. [Online]. Available: http://www.ncbi.nlm.nih.gov/books/NBK190576/
- "Decision
on promulgating Technical Guidelines on prenatal and neonatal
screening, diagnosis, and treatment". Vietnam Ministry of Health.
1807/QD-BYT (2020). https://www.scribd.com/document/735422154/1807-qd-byt-21042020-4-signed-1.
- Phengsavanh,
S. Sengchanh, C. Souksakhone, B. Souvanlasy, and V. Sychareun, "Current
Status of Thalassemia in Lao People's Democratic Republic," Hemoglobin,
vol. 46, no. 1, pp. 58-61, Jan. 2022. https://doi.org/10.1080/03630269.2022.2069034 PMid:35950579
- Khanh
B.Q., Ha N.T.T., Chi N.T., and Tri N.A., "Investigation of situation
about thalassemia and hemoglobinopathies in 6 ethnic groups in
Northeast of Vietnam," Vietnam Medical Journal, vol. 502. Special
Issue, pp. 49-57, 2021.
- Khanh
B.Q., Ha N.T.T., Chi N.T., and Tri N.A., "Research on characteristics
of thalassemia/hemoglobinopathy in the Thai and Muong ethnic groups,"
Vietnam Medical Journal, vol. 502. Special Issue, pp. 66-72, 2021.
- Khanh
B.Q., Ha N.T.T., and Tri N.A., "Study on thalassemia/hemoglobinopathy
in 7 ethnic minorities in Northwest Vietnam," Vietnam Medical Journal,
vol. 502. Special Issue, pp. 58-65, 2021.
- Ha
N.T.T., Khanh B.Q., and Tri N.A., "Estimating the risk of inheriting
Thalassemia and Hemoglobinopathies genes among 6 ethnic minority groups
in Northern region, Vietnam," Vietnam Medical Journal, vol. 502.
Special Issue, pp. 103-111.
- S.
He et al., "Molecular Characterization of α- and β-Thalassaemia Among
Children From 1 to 10 Years of Age in Guangxi, A Multi-Ethnic Region in
Southern China," Front. Pediatr., vol. 9, Aug. 2021. https://doi.org/10.3389/fped.2021.724196 PMid:34497785 PMCid:PMC8419341
- M.
Nuinoon, K. Kruachan, W. Sengking, D. Horpet, and U. Sungyuan,
"Thalassemia and Hemoglobin E in Southern Thai Blood Donors," Advances
in Hematology, vol. 2014, no. 1, p. 932306, 2014. https://doi.org/10.1155/2014/932306 PMid:25050123 PMCid:PMC4094851
- S.
Sirichotiyakul, R. Saetung, and T. Sanguansermsri, "Analysis of
beta-thalassemia mutations in northern Thailand using an automated
fluorescence DNA sequencing technique," Hemoglobin, vol. 27, no. 2, pp.
89-95, May 2003. https://doi.org/10.1081/HEM-120021541 PMid:12779270
- K.
Mankhemthong, A. Phusua, S. Suanta, P. Srisittipoj, P. Charoenkwan, and
T. Sanguansermsri, "Molecular characteristics of thalassemia and
hemoglobin variants in prenatal diagnosis program in northern
Thailand," Int J Hematol, vol. 110, no. 4, pp. 474-481, Oct. 2019. https://doi.org/10.1007/s12185-019-02694-y PMid:31240559
- K.
Singha et al., "β-Hemoglobinopathies in the Lao People's Democratic
Republic: Molecular diagnostics and implications for a prevention and
control program," Int J Lab Hematol, vol. 43, no. 3, pp. 500-505, Jun.
2021, doi: 10.1111/ijlh.13406. https://doi.org/10.1111/ijlh.13406 PMid:33244864
- Ha
N.T.T et al., "Overview of Thalassemia: Current Situation, Risks and
Control Strategies in Vietnam," Vietnam Medical Journal, vol. 502.
Special Issue, pp. 3-16, 2021.
- Luu B.T., "Health service accessibility and utilization among ethnic minorities in Northern Vietnam. Bangkok, Thammasat University, 2023.
- Vietnam+
(VietnamPlus), "Vietnam raises awareness about Thalassemia," Vietnam+
(VietnamPlus). Accessed: July 29, 2025. [Online]. Available: https://en.vietnamplus.vn/vietnam-raises-awareness-about-thalassemia-post199993.vnp