S. maltophilia pneumonia ranks among the top ten causative agents of nosocomial pneumonia in intensive care units and accounts for approximately 0.4% to 8.7% of all nosocomial pneumonia cases.[6] It is particularly associated with high mortality rates in patients monitored in intensive care settings.[7] Advanced age, elevated organ failure scores (SOFA (Sequential Organ Failure Assessment), APACHE II), corticosteroid use, neutropenia, prior carbapenem exposure, and concurrent infections are among the most frequently reported risk factors associated with mortality.[3,7]
In this study, we aimed to describe the clinical characteristics of patients presenting with S. maltophilia pneumonia and to identify the risk factors independently associated with 30-day mortality among hospitalized patients diagnosed with this infection.
Materials and Methods
Study design and Patient groups. This study was designed as a retrospective, single-center cohort study. Patients over the age of 18 who were hospitalized between January 2018 and December 2021, with S. maltophilia isolated from respiratory secretions (sputum, endotracheal aspirate, or bronchoalveolar lavage) and clinical and/or radiological findings consistent with pneumonia, were enrolled in the study. Only the first episode of pneumonia for each patient was included in the study, and any subsequent recurrent pneumonia episodes in the same patient were excluded from the analysis. Data on patient demographics, comorbid conditions, and laboratory findings were obtained from the hospital’s electronic medical record system. Patients who met the inclusion criteria were categorized into two groups based on 30-day mortality status. The Ethics Committee approved the study with decision number 13 on September 7, 2021. Due to the retrospective design, informed consent was waived. Patient identifiers were removed before analysis.Definitions. The diagnosis of S. maltophilia pneumonia was established based on the presence of new or progressive pulmonary infiltrates (on chest radiography and/or pulmonary CT), a positive microbiological culture, and at least one of the following clinical symptoms: fever (≥ 38 °C), newly developed cough, chest pain, dyspnea, or worsening oxygenation. S. maltophilia colonization was defined as a positive microbiological culture for S. maltophilia in the absence of the previously described clinical signs of infection. In lower respiratory tract samples, growth of at least 10⁴ CFU/mL for bronchoalveolar lavage and at least 10⁵ CFU/mL for endotracheal aspirate was considered significant. Inflammatory biomarkers were not used in the standard case definition; procalcitonin values above 0.5 ng/mL were considered supportive when consistent with clinical and radiological findings. Patients who did not meet the clinical-radiological criteria for pneumonia despite significant growth in respiratory tract samples and who received an alternative non-infectious diagnosis during file review were classified as colonized and excluded from the study. Hospital-acquired pneumonia is defined as pneumonia that occurs ≥48 hours after hospital admission and was not incubating at the time of admission.[8] Polymicrobial infection was defined as the presence of any organism other than S. maltophilia in the same index sample. Coinfection was defined as the isolation of an additional bacterial pathogen from any clinical culture, except the index respiratory specimen, within 72 hours of initial sample collection. Appropriate therapy was defined as the initiation of treatment following the identification of Stenotrophomonas maltophilia in respiratory cultures, using at least one antimicrobial agent with proven clinical efficacy against this pathogen. The choice of antimicrobial and intravenous dosing was guided by the Sanford Guide, with dose adjustments made based on estimated creatinine clearance when clinically necessary.
Microbiological Identification. MALDI-TOF MS (VITEK MS, bioMérieux, France) was used for the identification of the isolates, and VITEK 2 (bioMérieux, Marcy l'Étoile, France) was used for phenotypic AST. Susceptibility results were interpreted according to EUCAST clinical breakpoint versions implemented during the study period (2018–2021, depending on the year of isolation).
Statistical Analysis. The groups were compared statistically with respect to demographic characteristics, underlying comorbidities, mortality-associated risk factors, and administered antimicrobial therapies. Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 22.0 (IBM Corp., Armonk, NY, USA). The normality of data distribution was evaluated through histograms, Q-Q plots, and the Shapiro-Wilk test. Categorical variables are expressed as frequencies and percentages, and comparisons were made using the chi-square test. Continuous variables are presented as mean ± standard deviation (SD) or as median values with interquartile ranges (IQR, 25th–75th percentiles). For comparing continuous variables, the independent-samples t-test was used for normally distributed data, and the Mann-Whitney U test was used for non-normally distributed data. To identify risk factors influencing 30-day mortality, variables with a p-value <0.20 in univariate analysis-including age, hematologic malignancy, SOFA score at diagnosis, chronic kidney disease, Charlson Comorbidity Index, presence of a central venous catheter, mechanical ventilation, chemotherapy, history of surgery within 30 days, prior use of carbapenems, tigecycline, quinolones, or polymyxins within 30 days, as well as treatment regimens involving quinolones and polymyxins-were entered into a multivariate logistic regression model using the backward likelihood ratio (LR) method, after confirming that the variables were not correlated with each other. A p-value of <0.05 was considered statistically significant.
Results
A total of 200 hospitalized patients with S. maltophilia isolated from respiratory secretions were screened. Ninety-six patients (48%) who met the criteria for colonization were excluded, and the data of a final 104 patients were analysed (Figure 1).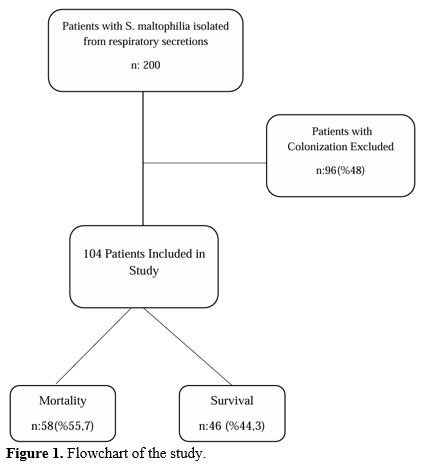 |
|
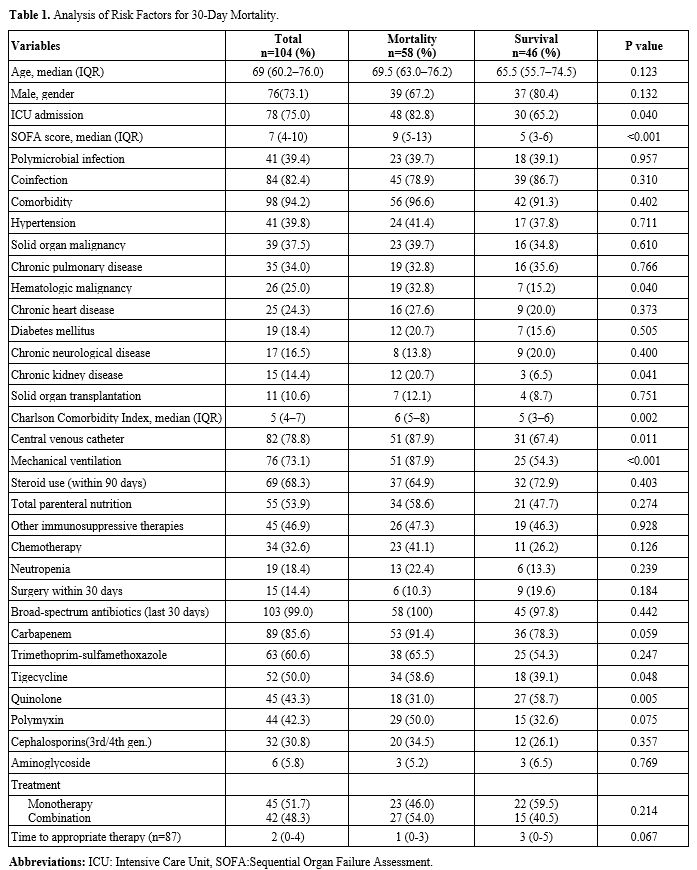
The 30-day mortality rate among the patients included in the study was 55.7%. Seven patients had concomitant S. maltophilia bacteremia. Solid organ malignancies were present in 37.5%, and hematological malignancies in 25%. Polymicrobial infections and coinfections were observed in 39.4% and 82.4%, respectively. Patient characteristics according to 30-day mortality status are presented in Table 1. In univariate analysis, hematologic malignancy (32.8% (n=19) vs. 15.2% (n=7), p=0.040), SOFA score (9 (5-13) vs. 5 (3-7), p<0.001),chronic kidney disease (20.7% (n=12) vs. 6.5% (n=3), p=0.041), Charlson Comorbidity Index (6 (5–8) vs. 5 (3–6), p=0.002), presence of a central venous catheter (87.9% (n=51) vs. 67.4% (n=31), p=0.011), mechanical ventilation (87.9% (n=51) vs. 54.3% (n=25), p <0.001), and the use of carbapenems (91.4% (n=53) vs. 78.3% (n=36), p=0.059), tigecycline (58.6% (n=34) vs. 39.1% (n=18), p =0.048) within the past 30 days were all significantly associated with increased 30-day mortality. Prior quinolone exposure within 30 days was significantly associated with reduced 30-day mortality (31.0% vs. 58.7%, p=0.005). No resistance to TMP-SXT was detected in any of the isolates.
 |
|
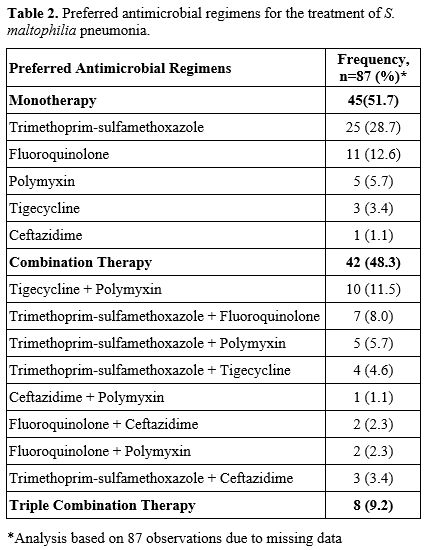
Preferred antimicrobial regimens for the treatment of S. maltophilia pneumonia are presented in Table 2. The analysis was based on 87 observations due to missing data. A total of 45 patients (51.7%) received monotherapy, whereas 42 patients (48.3%) were administered combination therapy. The most frequently preferred treatment was TMP-SXT (28.7%).
 |
|
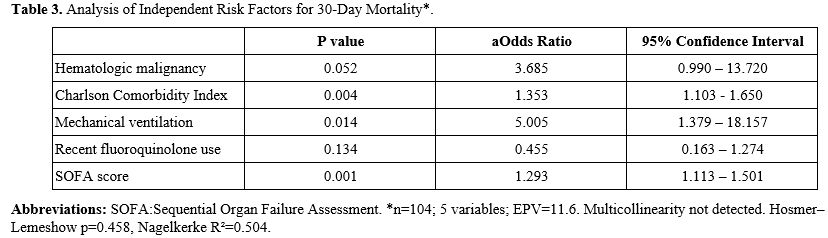
In the multivariate analysis SOFA score (OR = 1.293, 95% CI [1.113-1.501], p = 0.001), mechanical ventilation (OR = 5.005, 95% CI [1.379-18.157], p = 0.014), and a high Charlson Comorbidity Index (OR = 1.353, 95% CI [1.103-1.650], p = 0.004) were identified as independent risk factors significantly associated with mortality (Table 3).
 |
|
Discussion
S. maltophilia pneumonia predominantly occurs in critically ill patients in intensive care units, particularly those requiring mechanical ventilation support. In our study, similar to the literature, approximately three-quarters of the patients had ICU admission with ventilator support..[9] Moreover, well-known risk factors for S. maltophilia infection – such as solid organ malignancies and hematologic malignancies – were present in 37.5% and 25% of our patients, respectively, consistent with prior reports.[10] Antibiotic exposure (notably prior carbapenem use) is also a recognized risk factor associated with S. maltophilia infections.[11] Polymicrobial infections and co-infections were frequently observed (39.4% and 82.4% of cases, respectively). About half of the patients (48.3%) received combination antimicrobial therapy; however, we did not find any significant impact of combination therapy on 30-day mortality (p = 0.214).Our results highlight the frequent occurrence of S. maltophilia colonization in the respiratory tract (48%). Recent multicenter studies have reported colonization rates ranging from 56% to 79% in hospitalized patients.[12,13] These findings support the notion that a significant proportion of S. maltophilia isolations are attributable to colonization rather than infection.
In our study, the mortality rate was 55%, and the SOFA score, the need for mechanical ventilation, and a high Charlson Comorbidity Index are significant risk factors for 30-day mortality in patients with S. maltophilia pneumonia. S. maltophilia infections are particularly associated with high mortality rates among intensive care patients and immunosuppressed individuals. Although mortality data often derive from single-center studies, overall mortality rates have been reported to range from 18% to 69%, with attributable mortality rates ranging from 24% to 58%.[1] Pneumonia is the infection type with the highest mortality rate.[14] In the ICU, mortality rates as high as 82.1% have been documented.[9] A study from Turkey investigating all S. maltophilia infections reported a mortality rate of 53% among patients with pneumonia.[15] Consistent with these findings, our study also revealed a high mortality rate of 55.7%, further supporting the data reported in the literature.
In our study, the SOFA score was significantly higher in the mortality group and was identified as an independent predictor of mortality (OR = 1.293, 95% CI [1.113–1.504], p = 0.001). This finding suggests that mortality in S. maltophilia infections is not only related to the pathogen’s resistance profile or the treatment used, but also closely linked to the patient’s level of organ dysfunction and physiological reserve at the time of infection. Our results align with previous studies showing a link between higher SOFA scores and increased mortality.[9,13] Similarly, in the study by Hasbek et al., the SOFA score was identified as an independent risk factor for 28-day mortality in patients with S. maltophilia infections, supporting its value as a prognostic tool in this patient group.[15] Therefore, early and systematic evaluation of the SOFA score in patients with S. maltophilia infections appears clinically important for quickly identifying high-risk individuals and more accurately predicting mortality risk.
Another independent risk factor identified in our study was the Charlson Comorbidity Index (CCI) (OR = 1.353, 95% CI [1.103-1.650], p = 0.004). In a national cohort study in the United Kingdom that included all S. maltophilia infections, researchers demonstrated that a CCI score of 4 or higher was associated with a 36% increase in mortality.[19] In a recent study from Turkey by Hasbek et al., which included cases of primary bacteremia and pneumonia, a high CCI score (≥5) was significantly associated with increased mortality, particularly in the pneumonia subgroup.[15] Our findings support previous data indicating that mortality is significantly higher in patients with S. maltophilia infections who have underlying comorbidities.
Approximately 76–80% of S. maltophilia pneumonia cases have been reported to manifest as ventilator-associated pneumonia (VAP).[9,20] In our study, the rate of patients requiring mechanical ventilation was similarly high, at 73.1%. Moreover, mechanical ventilation was identified as an independent risk factor for 30-day mortality, increasing the risk of death by fivefold (OR = 5.005, 95% CI [1.379-18.157], p = 0.014). In a large multicenter cohort, the rate of invasive mechanical ventilation was significantly higher among patients who died within 30 days compared to those who survived.[18] Other studies have likewise shown that mechanical ventilation raises mortality risk by 4.4 to 5.7 times.[21,22] These findings suggest that the need for mechanical ventilation is a critical factor that directly increases mortality risk.
The optimal treatment strategy for S. maltophilia infections has not been definitively established, although TMP-SXT remains the most commonly used agent for susceptible strains. Fluoroquinolones, another frequently employed therapeutic option, are widely used in patients who are either resistant to or intolerant of TMP-SXT. While increasing resistance to TMP-SXT has been reported in the literature, no resistance to TMP-SXT was detected in our study. Among the 10 levofloxacin-tested isolates, resistance was identified in 2. A meta-analysis evaluating resistance rates of S. maltophilia worldwide, including data from Turkey, reported a global levofloxacin resistance rate of 14.4% and a TMP-SMX resistance rate of 9.2%, with an upward trend in resistance to both agents over time.[23] Another Turkish study found resistance rates of 5.6% for tigecycline, 7% for levofloxacin, and 8.5% for TMP-SXT.[24] Although TMP-SXT and levofloxacin remain among the most frequently preferred agents in treatment, the increasing resistance observed in various bacterial pathogens underscores the importance of monitoring antimicrobial susceptibility patterns.
In our study, the most frequently preferred therapeutic agents were TMP-SXT and fluoroquinolones. Notably, the proportion of patients receiving combination regimens was relatively high. This finding may be attributable to the high prevalence of polymicrobial infections and coinfections among our cohort. However, combination therapy did not confer an additional survival benefit. Guerci P et al. reported that appropriate antibiotic use, timing of initiation, combination therapy, and treatment duration have not generally had a significant impact on mortality in S. maltophilia pneumonia.[20] Combination therapy also did not affect 30-day mortality. Liang et al. reported no mortality benefit from combination therapy in the general cohort, though a potential benefit was observed in immunocompromised patients and those with APACHE II scores≥15.[18] Another ICU-based study found no effect of appropriate or combination therapy on mortality.[9] These findings support the idea that mortality is more influenced by host-related risk factors than by therapeutic interventions.
Our study has several limitations. This study was conducted in a single center with a retrospective design and a relatively small sample size, which may limit the generalizability of the findings to other patient populations and healthcare settings. Due to the retrospective design, certain potentially important clinical parameters — such as the exact timing and appropriateness of antimicrobial initiation, dosing adjustments, and detailed severity scores — could not be consistently obtained, which may have affected the interpretation of treatment outcomes. Finally, the comparison between combination therapy and monotherapy is observational and may be biased by confounding by indication and immortal time bias; therefore, differences in outcomes may not solely reflect the effect of the treatment regimen.
Conclusions
S. maltophilia pneumonia is a severe nosocomial infection associated with high mortality, particularly among intensive care patients with malignancies. Polymicrobial infections and coinfections are also common. In this study, SOFA score, mechanical ventilation, and a high Charlson Comorbidity Index were identified as independent risk factors for mortality. No significant impact of combination therapy on 30-day mortality was detected. Risk stratification and individualized monitoring may play a critical role in reducing mortality in this vulnerable patient population.References
- Mojica MF, Humphries R, Lipuma JJ, Mathers AJ, Rao GG, Shelburne SA, Fouts DE, Van Duin D, Bonomo RA. Clinical challenges treating Stenotrophomonas maltophilia infections: an update. JAC-Antimicrobial Resistance 2022;4:dlac040. https://doi.org/10.1093/jacamr/dlac040 PMid:35529051 PMCid:PMC9071536
- Hafiz TA, Aldawood E, Albloshi A, Alghamdi SS, Mubaraki MA,
Alyami AS, Aldriwesh MG. Stenotrophomonas maltophilia epidemiology,
resistance characteristics, and clinical outcomes: understanding of the
recent three years' trends. Microorganisms 2022;10:2506. https://doi.org/10.3390/microorganisms10122506 PMid:36557759 PMCid:PMC9786049
- Senol E. Stenotrophomonas maltophilia: the significance and role
as a nosocomial pathogen. Journal of Hospital Infection 2004;57:1-7. https://doi.org/10.1016/j.jhin.2004.01.033 PMid:15142709
- Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clinical Microbiology Reviews 2012;25:2-41. https://doi.org/10.1128/CMR.00019-11 PMid:22232370 PMCid:PMC3255966
- Mendes ET, Paez JIG, Ferraz JR, Marchi AP, Silva ILAFE, Batista
MV, Lima ALMD, Rossi F, Levin AS, Costa SF. Clinical and
microbiological characteristics of patients colonized or infected by
Stenotrophomonas maltophilia: is resistance to
sulfamethoxazole/trimethoprim a problem? Revista do Instituto de
Medicina Tropical de São Paulo 2020;62:e96. https://doi.org/10.1590/s1678-9946202062096 PMid:33295480 PMCid:PMC7723352
- Wang Y, Wang Y, Rong H, Guo Z, Xu J, Huang X. Risk factors of
lower respiratory tract infection caused by Stenotrophomonas
maltophilia: systematic review and meta-analysis. Frontiers in Public
Health 2023;10:1035812. https://doi.org/10.3389/fpubh.2022.1035812 PMid:36703851 PMCid:PMC9871542
- Saugel B, Eschermann K, Hoffmann R, Hapfelmeier A, Schultheiss C,
Phillip V, Eyer F, Laugwitz K-L, Schmid RM, Huber W. Stenotrophomonas
maltophilia in the respiratory tract of medical intensive care unit
patients. European Journal of Clinical Microbiology & Infectious
Diseases 2012;31:1419-28. https://doi.org/10.1007/s10096-011-1459-8 PMid:22057419
- Guidelines for the management of adults with hospital-acquired,
ventilator-associated, and healthcare-associated pneumonia. American
Journal of Respiratory and Critical Care Medicine 2005;171:388-416. https://doi.org/10.1164/rccm.200405-644ST PMid:15699079
- Lee YH, Lee J, Yu B, Lee WK, Choi SH, Park JE, Seo H, Yoo SS, Lee
SY, Cha S-I, Kim CH, Park JY. Risk factors for mortality in intensive
care unit patients with Stenotrophomonas maltophilia pneumonia in South
Korea. Acute and Critical Care 2023;38:442-51. https://doi.org/10.4266/acc.2023.00682 PMid:37994018 PMCid:PMC10718495
- Ebara H, Hagiya H, Haruki Y, Kondo E, Otsuka F. Clinical
characteristics of Stenotrophomonas maltophilia bacteremia: a regional
report and a review of a Japanese case series. Internal Medicine
2017;56:137-42. https://doi.org/10.2169/internalmedicine.56.6141 PMid:28090041 PMCid:PMC5337456
- Dimopoulos G, Garnacho-Montero J, Paramythiotou E,
Gutierrez-Pizarraya A, Gogos C, Adriansen-Pérez M, Diakaki C, Matthaiou
DK, Poulakou G, Akinosoglou K. Upraising Stenotrophomonas maltophilia
in critically ill patients: a new enemy? Diagnostics 2023;13:1106. https://doi.org/10.3390/diagnostics13061106 PMid:36980413 PMCid:PMC10047194
- Hase R, Sakurai A, Suzuki M, Itoh N, Saito S, Hayakawa K, Uemura
K, Matsumara Y, Kato H, Van Duin D, Ohmagari N, Doi Y. Stenotrophomonas
maltophilia in Japanese hospitals: clinical characteristics and
molecular epidemiology of infection and colonization cases registered
in a multicenter surveillance network. Open Forum Infectious Diseases
2023;10:ofad500.781. https://doi.org/10.1093/ofid/ofad500.781 PMCid:PMC10677168
- Tanuma M, Sakurai T, Nakaminami H, Tanaka M. Risk factors and
clinical characteristics for Stenotrophomonas maltophilia infection in
an acute care hospital in Japan: a single-center retrospective study.
Journal of Pharmaceutical Health Care and Sciences 2025;11:24. https://doi.org/10.1186/s40780-025-00429-2 PMid:40155984 PMCid:PMC11951655
- Al Qura'an A, Salazar W, Al Khouri Z, Munshi R, Pichilingue Reto
P, Pinargote P. Risk factors for 90-day mortality among patients with
Stenotrophomonas maltophilia infection: a retrospective multicenter
study. Open Forum Infectious Diseases 2025;12:ofae631.477. https://doi.org/10.1093/ofid/ofae631.477 PMCid:PMC11779009
- Hasbek M, Aldemir Ö, Çakır Kıymaz Y, Baysal C, Yıldırım D,
Büyüktuna SA. Mortality rates and risk factors associated with
mortality in patients with Stenotrophomonas maltophilia primary
bacteremia and pneumonia. Diagnostic Microbiology and Infectious
Disease 2025;111:116664. https://doi.org/10.1016/j.diagmicrobio.2024.116664 PMid:39729953
- Aitken SL, Sahasrabhojane PV, Kontoyiannis DP, Savidge TC, Arias
CA, Ajami NJ, Shelburne SA, Galloway-Peña JR. Alterations of the oral
microbiome and cumulative carbapenem exposure are associated with
Stenotrophomonas maltophilia infection in patients with acute myeloid
leukemia receiving chemotherapy. Clinical Infectious Diseases
2021;72:1507-13. https://doi.org/10.1093/cid/ciaa778 PMid:32544947 PMCid:PMC8096257
- Safdar A, Rolston KV. Stenotrophomonas maltophilia: changing
spectrum of a serious bacterial pathogen in patients with cancer.
Clinical Infectious Diseases 2007;45:1602-9. https://doi.org/10.1086/522998 PMid:18190323
- Chen L, Hua J, Hong S, Yuan C, Jing R, Luo X, Zhu Y, Le L, Wang
Z, Sun X, He X. Assessment of the relative benefits of monotherapy and
combination therapy approaches to the treatment of hospital-acquired
Stenotrophomonas maltophilia pneumonia: a multicenter, observational,
real-world study. Annals of Intensive Care 2023;13:47. https://doi.org/10.1186/s13613-023-01144-7 PMid:37278862 PMCid:PMC10244312
- Appaneal HJ, Lopes VV, LaPlante KL, Caffrey AR. Treatment,
clinical outcomes, and predictors of mortality among a national cohort
of hospitalized patients with Stenotrophomonas maltophilia infection.
Public Health 2023;214:73-80. https://doi.org/10.1016/j.puhe.2022.10.025 PMid:36521275
- AZUREA Research Network, Guerci P, Bellut H, Mokhtari M,
Gaudefroy J, Mongardon N, Charpentier C, Louis G, Tashk P, Dubost C,
Ledochowski S, Kimmoun A, Godet T, Pottecher J, Lalot J-M, Novy E,
Hajage D, Bouglé A. Outcomes of Stenotrophomonas maltophilia
hospital-acquired pneumonia in intensive care unit: a nationwide
retrospective study. Critical Care 2019;23:371. https://doi.org/10.1186/s13054-019-2649-5 PMid:31752976 PMCid:PMC6873544
- Kızılırmak D, Havlucu Y. Clinical characteristics and prognostic
factors of patients with Stenotrophomonas maltophilia pneumonia:
10-year experience from a single center. Cureus 2023. https://doi.org/10.7759/cureus.47187 PMid:38021834 PMCid:PMC10652227
- Insuwanno W, Kiratisin P, Jitmuang A. Stenotrophomonas
maltophilia infections: clinical characteristics and factors associated
with mortality of hospitalized patients. Infection and Drug Resistance
2020;13:1559-66. https://doi.org/10.2147/IDR.S253949 PMid:32547125 PMCid:PMC7266396
- Dadashi M, Hajikhani B, Nazarinejad N, Noorisepehr N, Yazdani S,
Hashemi A, Hashemizadeh Z, Goudarzi M, Fatemeh S. Global prevalence and
distribution of antibiotic resistance among clinical isolates of
Stenotrophomonas maltophilia: a systematic review and meta-analysis.
Journal of Global Antimicrobial Resistance 2023;34:253-67. https://doi.org/10.1016/j.jgar.2023.02.018 PMid:36906172
- Karamanlıoğlu D, Dizbay M. Hospital-acquired Stenotrophomonas
maltophilia infections: epidemiology and risk factors for mortality.
FLORA 2024;29:422-9. https://doi.org/10.5578/flora.2024041112