During the transplantation process, the risk of febrile neutropenia (FN) increases substantially due to intensive chemoradiotherapy-induced immunosuppression, neutropenic failure, prolonged retention of central venous catheters, and mucositis.[8] In patients who develop FN, bacterial, fungal, or viral infections may follow a severe course, be rapidly progressive, and be fatal.[9] In particular, bloodstream infection (BSI) is a common infectious complication in the early period following allo-HSCT, with reported incidences ranging from 13.6% to 38.9%.[10-12] In addition, laboratory findings, such as elevated procalcitonin and high C-reactive protein (CRP) levels, are associated with poor prognosis.[13-14]
The aim of this study was to compare the incidence of FN, infection characteristics, and the effect of FN on mortality in patients with hematologic malignancies who received either fresh or cryopreserved stem cell infusions. Additionally, the independent effects of variables, such as patients’ demographic and clinicopathological data, duration of FN episodes, depth of neutropenia, length of hospital stay, infectious agents, and patients’ comorbidity scores on FN-related mortality were investigated.
Materials and Methods
Study design and population. In this study, the data of 155 patients who underwent allo-HSCT at our hematology clinic between 2010 and 2023 were retrospectively reviewed. A total of 143 patients aged ≥18 years with FN and a hematological disease were included in the study. Twelve patients who did not develop FN during allo-HSCT were excluded. Patient data were obtained from the hospital information system and patient files.Mobilization and apheresis procedures for allo-HSCT were performed according to international standards. All donors were mobilized with G-CSF alone (10 μg/kg/day for 4–5 days); plerixafor was not used in healthy donors in this cohort. Apheresis was performed using the Spectra Optia (Terumo BCT, Lakewood, CO, USA) cell separators, and CD34⁺ cell counts were monitored by flow cytometry. No collection failures occurred during the study period. Peripheral blood stem cells collected from donors after mobilization were obtained using an apheresis device. The collected fresh cell products were preserved under appropriate conditions (+4°C) on the same day and infused into the recipient within 24 h at the latest. No freezing or cryoprotectant agents were used for fresh products.[15] For cryopreserved products, cells were frozen at a controlled rate with a cryoprotectant solution containing 10% DMSO and stored long-term at –80°C.[16] According to the ASTCT guidelines, the minimum acceptable CD34⁺ cell dose for transplantation is≥2 × 10⁶ CD34⁺ cells/kg, while the ideal collection target is 2–5 × 10⁶ CD34⁺ cells/kg.
A febrile episode during FN was defined as a single oral or axillary temperature measurement>38.3°C or a sustained temperature>38°C for at least 1 h. Neutropenia was defined as either an expected neutrophil count of <500/µL or a neutrophil level between 500–1000/µL anticipated to fall to <500/µL within 48 h.[17] All patients received ciprofloxacin prophylaxis.
We performed computed tomography scans and serum galactomannan measurements to identify patients with invasive pulmonary aspergillosis (IPA). Starting on the first day of the FN episode, serum samples were collected twice weekly for galactomannan testing. According to the European Organization for Research and Treatment of Cancer/Mycoses Study Group (EORTC/MSG) revised definitions of invasive fungal disease, IPA was categorized as “possible,” “probable,” or “proven”.[18]
The Hematopoietic Cell Transplantation–Comorbidity Index (HCT-CI) was used to evaluate the patients’ pre-transplant comorbidity burden. According to the original definition by Sorror et al., patients were evaluated in three risk groups: a score of 0 was classified as low risk, 1–2 as intermediate risk, and ≥3 as high risk.[19]
Bacterial identification was performed by matrix-assisted laser desorption ionization–time-of-flight–mass spectrometry (MALDI–TOF–MS) using a Bruker Daltonics 5 system from Germany. Antimicrobial susceptibility testing encompassed the PhoenixTM 100 System Kirby–Bauer Disk Diffusion test (Oxoid, UK) and gradient diffusion methods (bioMérieux, France). The recommendations of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) were applied, and, according to CDC recommendations, carbapenem resistance was defined as resistance to at least one carbapenem.[20,21]
The primary outcome was to compare the incidence and duration of FN between recipients of fresh and cryopreserved grafts. Secondary outcomes included evaluating BSI and IPA and identifying independent risk factors for FN-related mortality.
Statistical Analysis. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0. Descriptive statistics were presented as n (%) for categorical variables and as median for continuous variables. Continuous variables were compared using the Mann–Whitney U test. Categorical variables were compared using the chi-square test. Factors affecting FN-related mortality were first analyzed by univariate logistic regression. Variables with p-values of <0.05 in univariate analysis were included in the multivariate logistic regression model. A p-value of <0.05 was considered statistically significant in all analyses.
Ethical Approval. The ethics committee of the Faculty of Medicine, Bursa Uludag University, approved this study (decision number: 2023-7/9).
Results
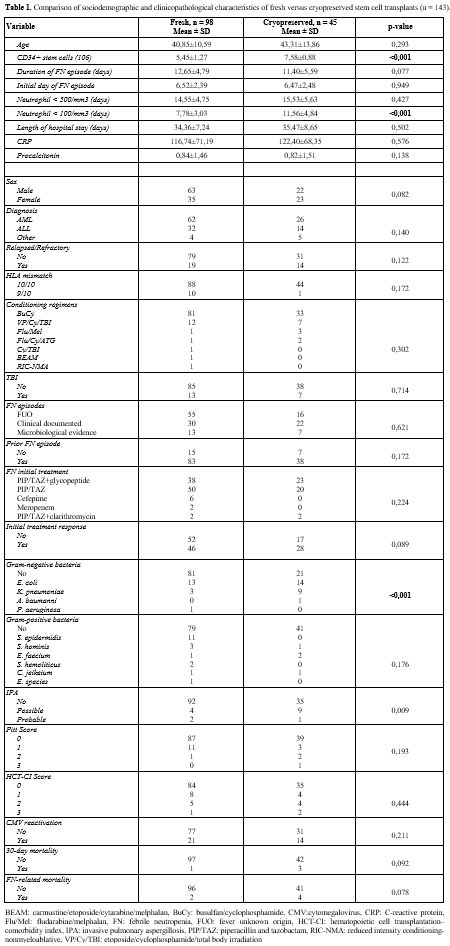
A total of 143 patients were included in the study; 98 underwent allo-HSCT with fresh stem cells and 45 with cryopreserved stem cells. Of the patients, 88 had acute myeloid leukemia (AML), and 46 had acute lymphoblastic leukemia (ALL). Additionally, 98 transplants were performed prior to the COVID-19 pandemic. No significant differences were found between the two groups regarding age, sex distribution, type of diagnosis, rate of relapsed/refractory disease, HLA compatibility, conditioning regimens used, or the application of total body irradiation (TBI) (p > 0.05). The CD34+ cell count was significantly higher in the cryopreserved group (7.58 ± 0.88 × 10⁶/kg vs. 5.45 ± 1.27 × 10⁶/kg; p <0.001). The duration of the FN episode was similar between the groups (11.40 ± 5.59 vs. 12.65 ± 4.79 days; p = 0.077). However, the duration of deep neutropenia (ANC <100/mm³) was significantly longer in the cryopreserved group (11.56 ± 4.84 vs. 7.78 ± 3.03 days; p <0.001). There was no significant difference between the groups in the number of days with neutrophils <500/mm³ or in length of hospital stay (p > 0.05).No significant differences were observed between groups regarding the day of onset of the FN episode, etiology of FN (Fever of unknown, clinical, microbiological), initial treatment regimens, or treatment response. Gram-positive bacterial (GPB) infections were similar between the groups (p = 0.176). Gram-negative bacteria (GNB) were more frequent in the cryopreserved group (p <0.001). The probability of invasive fungal infection (IFA) was also higher in the cryopreserved group (p = 0.009). Although 30-day mortality (fresh 1% vs. cryopreserved 6.8%; p = 0.092) and FN-related mortality (fresh 2% vs. cryopreserved 6.8%; p = 0.078) were higher in the cryopreserved group, these differences did not reach statistical significance (Table 1).
 |
|
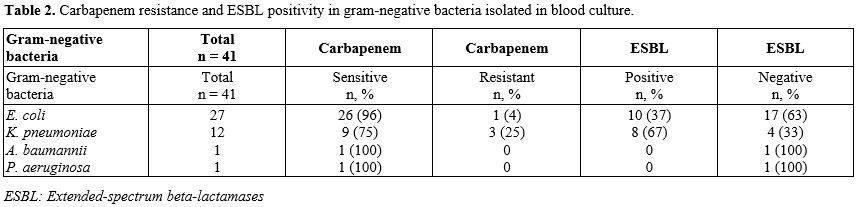
GNB accounted for 64% (41/63) of BSI episodes, and GPB for 36% (22/63). The most frequently isolated GPBs were S. epidermidis (8%) and S. hominis (3%). The most frequently isolated GNB were E. coli (n = 27, 19%) and K. pneumoniae (n = 14, 8%). Among E. coli isolates, 96% were carbapenem-sensitive, and 4% were carbapenem-resistant. Among K. pneumoniae isolates, 75% were carbapenem-sensitive, and 25% were carbapenem-resistant. Thirty-seven percent of E. coli isolates were ESBL-positive, and 63% were ESBL-negative. Sixty-seven percent of K. pneumoniae isolates were ESBL-positive, and 33% were ESBL-negative (Table 2).
 |
|
Univariate logistic regression analysis for FN-related mortality revealed that the significant risk factors were duration of FN episode (16.67±7.06 vs. 12.07 ± 4.91 days; p = 0.038), higher procalcitonin level (2.30 ± 2.31 vs. 0.77 ± 1.40; p = 0.046), and higher HCT-CI score (p = 0.037) (Table 3). In the multivariable logistic regression analysis, prolonged FN episode duration (OR 1.18; 95% CI 0.99–1.41; p = 0.046) and higher HCT-CI scores (Score 1: OR 20.80; p = 0.014; Score 2: OR 22.88; p = 0.039) were identified as independent risk factors for FN-related mortality. No significant correlation was found between procalcitonin level and risk of FN-related mortality (Table 4).
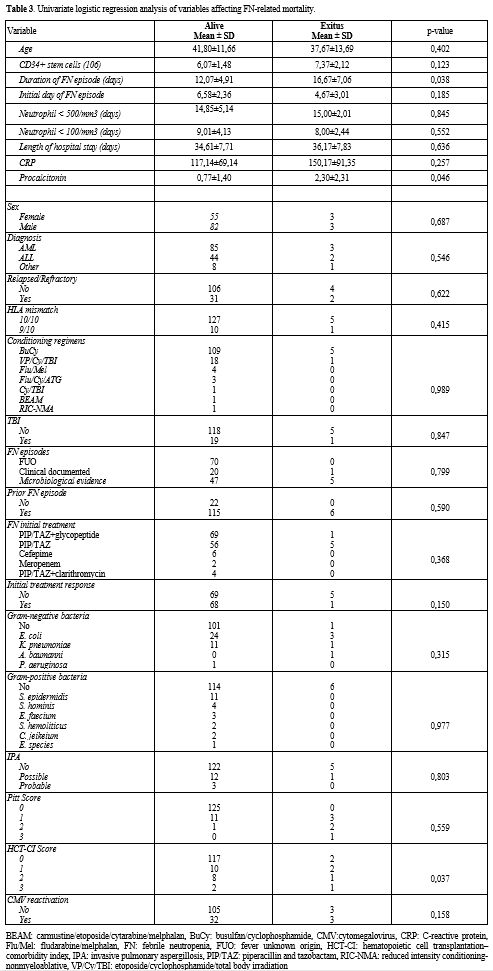 |
Table 3. Univariate logistic regression analysis of variables affecting FN-related mortality. |
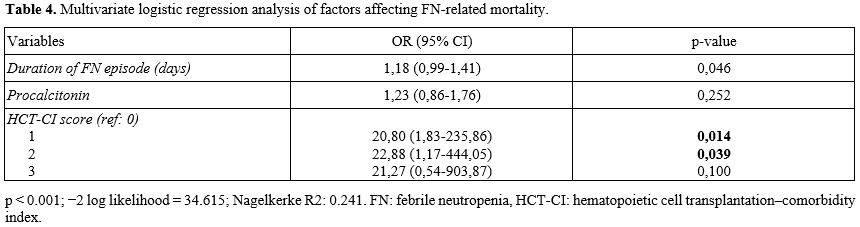 |
Table 4. Multivariate logistic regression analysis of factors affecting FN-related mortality. |
Discussion
This study provides significant data on the incidence, course, and mortality of FN in patients undergoing allo-HSCT with fresh and cryopreserved grafts. Although cryopreserved stem cell grafts prolonged the duration of deep neutropenia and increased the risk of GNB and fungal infections, they did not translate into increased FN-related mortality. This study demonstrated that, irrespective of graft type, prolonged FN duration and high HCT-CI comorbidity score are the primary determinants of mortality.Nevertheless, most studies reported no effect of cryopreservation on engraftment and hematopoietic recovery.[22,23] There was also biological evidence that the different cell types comprising the graft exhibit varying degrees of sensitivity to cryopreservation and storage. In recent years, knowledge in this field has expanded significantly, indicating that cryopreservation, as well as the various variables associated with it, may differentially affect not only the viability but also the function of various graft components.[24]
Prolonged and deep neutropenia is a strong factor that increases mortality risk in patients with hematological malignancies and those undergoing allo-HSCT. Moreover, prolonged neutropenia increases the risk of gram-negative bacteremia and sepsis by facilitating bacterial translocation, which significantly elevates FN-related mortality.[25,26] Islas-Muñoz et al. reported that prolonged neutropenia significantly increases the risk of BSI and 30-day mortality in patients with hematological malignancies.[27] Cao et al. showed that prolonged neutropenia (>21 days) is an independent risk factor for BSI in patients with allo-HSCT.[28] Our findings are consistent with these reports and indicate that prolonged neutropenia is associated with increased FN-related mortality during allo-HSCT.
The rate of infection, particularly bacterial infections, is high in patients with FN and is frequently observed in the early post-transplant period.[29] Zhang et al. showed that 70.8% of BSIs during FN were caused by GNB, among which high rates of ESBL and carbapenem-resistant strains were noted, and mortality was higher in the presence of resistant GNB.[30] A multicenter study in Argentina involving patients with hematological malignancies and HSCT recipients demonstrated that carbapenem-resistant strains were strongly associated with mortality when GNB were isolated.[31] In the present study, similar to published reports, GNB-related BSIs were significantly more frequent in the cryopreserved graft cohort.[32-34] However, no statistically significant difference in FN-related mortality was observed between the groups.
Among the six patients who died, GNB were isolated in five cases, whereas no GPB were isolated in any of these patients. Of the isolates, three had E. coli (2 ESBL+, 1 carbapenem-resistant), one was K. pneunomiae (ESBL+ and carbapenem-resistant), and one was A. baumannii (ESBL- and carbapenem-sensitive). In one patient, no bacteria were isolated in the culture. Our findings indicate that GNB in BSIs were more closely associated with mortality than GPB.
Pagano et al. and his group showed that invasive fungal infections significantly reduced 1-year survival in patients undergoing allo-HSCT and that Aspergillus infections were particularly associated with high mortality.[35,36] Neofytos et al. reported a 12-week mortality rate of 46.7% among HSCT recipients who developed invasive aspergillosis.[37] A meta-analysis including 51 studies found that prolonged neutropenia after HSCT is associated with an increased risk of invasive fungal infections.[38] In the present study, the incidence of IPA was higher among recipients of cryopreserved grafts; however, IPA was not significantly associated with FN-related mortality. This suggests that although IPA may occur more frequently in cryopreserved graft recipients, it does not alone determine early FN-related mortality.
Another finding of the present study is that patients with a high HCT-CI score had a markedly increased risk of FN-related mortality. HCT-CI is an index developed by Sorror et al. to quantify the burden of pretransplant comorbidities in allo-HCT recipients and to predict non-relapse mortality (NRM) and survival.[19] Acosta-Medina et al. demonstrated that a high HCT-CI score was associated with reduced long-term OS in 87 patients with myelofibrosis who underwent allo-HSCT.[39] Bayrakter et al. reported that in-hospital mortality was significantly higher among patients with HCT-CI ≥ 2 who were admitted to the intensive care unit within the first 100 days after allo-HSCT.[40] Our results suggest that HCT-CI may be useful for predicting long-term mortality and estimating the risk of early FN-related mortality.
Unlike previous studies focused on engraftment and GVHD, our research examines infection-related outcomes and FN-related mortality in allo-HSCT. We provide novel insights by identifying that prolonged FN duration and comorbidity burden (HCT-CI), rather than graft cryopreservation, are the primary drivers of FN-related mortality. This distinction shifts the focus from graft processing to patient-specific risk factors in clinical management.
Limitations of the present study include its retrospective, single-center design, limited sample size, and temporal changes in transplant care standards. One limitation of our study is the relatively small number of mortality events, which may have led to high and less stable Odds Ratio estimates for certain predictors, such as the HCT-CI score. While these results underscore the clinical importance of pre-transplant comorbidities and FN duration, the exact magnitude of their impact should be interpreted with caution and validated in larger, prospective multicenter cohorts. Although the optimal storage condition for hematopoietic stem cells is widely considered to be -163°C, another limitation of our study is the use of mechanical freezers at -80°C for graft preservation. However, recent evidence and clinical reviews suggest that storage at -80°C is a safe and effective alternative for periods of up to several years, with no significant compromise in cell viability or engraftment kinetics.[41,42]
Conclusions
The results of the present study showed that infections were more frequent in cases that received cryopreserved grafts, although this did not have a direct effect on FN-related mortality. In contrast, multivariable analysis suggested that prolonged neutropenia duration and high HCT-CI scores may be more critical risk factors for FN-related mortality. However, due to the limited number of deaths, the high odds ratio estimates should be interpreted with caution. Although the associations were statistically significant, the exact effect sizes may reflect the high-risk nature of the cohort and require confirmation in larger multicenter studies. Overall, patient-related factors, including comorbid conditions and the duration of neutropenia, may be more relevant to FN-related outcomes than graft source.Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.References
- Yang, M., Xin, L., Li, H., Lu, X., Pan, X., Lei,
S., Li, Y., Zhu, L., Zhu, Q., Jiang, R., Jia, Z., Cheng, G., Zeng, L.,
& Zhang, L. Risk factors for bloodstream infection in paediatric
haematopoietic stem cell transplantation: a systematic review and
meta-analysis. J Hosp Infect 2023; 139: 11–22. http://doi.org/10.1016/j.jhin.2023.06.003
- Giaccone
L, Faraci DG, Butera S, Lia G, Di Vito C, Gabrielli G, Cerrano M,
Mariotti J, Dellacasa C, Felicetti F, Brignardello E, Mavilio D, Bruno
B. Biomarkers for acute and chronic graft versus host disease: state of
the art. Expert Rev Hematol 2021; 14(1): 79–96. http://doi.org/10.1080/17474086.2021.1860001
- Bembnista
E, Stawicka P, Matuszak P, Łojko-Dankowska A, Dytfeld D, Matuszak M,
Wache A, Kaźmierska K, Majewska E, Lewandowski K, Gil L Should we
cryopreserve allogenic hematopoietic stem cell grafts? In Vivo 2025;
39(2): 870–876. http://doi.org/10.21873/invivo.13890
- Strzelec
A, Gawlik-Rzemieniewska N, Klima A, Panek K, Helbig G. The impact of
cryopreservation on hematopoietic stem cell engraftment and
post-transplant outcome during the COVID-19 pandemic. In Vivo 2024;
38(3): 1271–1277. http://doi.org/10.21873/invivo.13565
- Ersal
T, Özkocaman V, Yalçın C, Orhan B, Candar Ö, Çubukçu S, Koca TG, Pınar
İE, Hunutlu FÇ, Özkalemkaş F. The effect of cryopreservation on
engraftment kinetics in fully matched allogeneic stem cell
transplantation: Real-life data and literature review. Transfus Apher
Sci 2023; 62(6): 103821. http://doi.org/10.1016/j.transci.2023.103821
- Medd
P, Nagra S, Hollyman D, Craddock C, Malladi R. Cryopreservation of
allogeneic PBSC from related and unrelated donors is associated with
delayed platelet engraftment but has no impact on survival. Bone Marrow
Transplant 2013; 48(2): 243–248. http://doi.org/10.1038/bmt.2012.118
- Hsu
JW, Farhadfar N, Murthy H, Logan BR, Bo-Subait S, Frey N, Goldstein SC,
Horowitz MM, Lazarus H, Schwanke JD, Shah NN, Spellman SR, Switzer GE,
Devine SM, Shaw BE, Wingard JR. The effect of donor graft
cryopreservation on allogeneic hematopoietic cell transplantation
outcomes: a center for international blood and marrow transplant
research analysis. Implications during the COVID-19 pandemic.
Transplant Cell Ther 2021; 27(6): 507–516. http://doi.org/10.1016/j.jtct.2021.03.015
- Yan
CH, Wang Y, Mo XD, Sun YQ, Wang FR, Fu HX, Chen Y, Han TT, Kong J,
Cheng YF, Zhang XH, Xu LP, Liu KY, Huang XJ. Incidence, risk factors,
mic2robiology and outcomes of pre-engraftment bloodstream infection
after haploidentical hematopoietic stem cell transplantation and
comparison with HLA-identical sibling transplantation. Clin Infect Dis
2018; 67(suppl 2): S162–S173. http://doi.org/10.1093/cid/ciy658
- Freifeld
AG, Bow JE, Sepkowitz KA, Boeckh MJ, Ito J, Mullen CA, Raad I, Rolston
KV, Young JH, Wingard JR; Infectious Diseases Society of America.
Clinical practice guideline for the use of antimicrobial agents in
neutropenic patients with cancer: 2010 update by the Infectious
Diseases Society of America. Clin Infect Dis 2011; 52(4): e56–e93. http://doi.org/10.1093/cid/cir073
- Kikuchi
M, Akahoshi Y, Nakano H, Ugai T, Wada H, Yamasaki R, Sakamoto K,
Kawamura K, Ishihara Y, Sato M, Ashizawa M, Terasako-Saito K, Kimura S,
Yamazaki R, Kanda J, Kako S, Nishida J, Kanda Y. Risk factors for pre-
and post-engraftment bloodstream infections after allogeneic
hematopoietic stem cell transplantation. Transpl Infect Dis 2015;
17(1): 56–65. http://doi.org/10.1111/tid.12345
- Mori
Y, Yoshimoto G, Nishida R, Sugio T, Miyawaki K, Shima T, Nagasaki Y,
Miyake N, Harada Y, Kunisaki Y, Kamezaki K, Numata A, Kato K,
Shiratsuchi M, Maeda T, Takenaka K, Iwasaki H, Shimono N, Akashi K,
Miyamoto T. Gastrointestinal graft-versus-host disease is a risk factor
for postengraftment bloodstream infection in allogeneic hematopoietic
stem cell transplant recipients. Biol Blood Marrow Transplant 2018;
24(11): 2302–2309. http://doi.org/10.1016/j.bbmt.2018.06.002
- Zhang
R, Xiong Y, Zhang L, Liu L. Epidemiology, microbiology, and risk
factors of bacterial bloodstream infections in patients after
allogeneic hematopoietic stem cell transplantation. Infect Drug Resist
2024; 17: 1561–1569. http://doi.org/10.2147/IDR.S451781
- Lee
SJ, Kim JH, Han SB, Paik JH, Durey A. Prognostic factors predicting
poor outcome in cancer patients with febrile neutropenia in the
emergency department: usefulness of qsofa. J Oncol 2018; 2018: 2183179.
http://doi.org/10.1155/2018/2183179
- Coyne
CJ, Castillo EM, Shatsky RA, Chan TC. Procalcitonin as a predictive
tool for death and ICU admission among febrile neutropenic patients
visiting the emergency department. Medicina (Kaunas) 2022; 58(8): 985. http://doi.org/10.3390/medicina58080985
- Al-Anazi
KA. Autologous hematopoietic stem cell transplantation for multiple
myeloma without cryopreservation. Bone Marrow Res 2012; 2012: 917361. http://doi.org/10.1155/2012/917361
- Berz
D, McCormack EM, Winer ES, Colvin GA, Quesenberry PJ. Cryopreservation
of hematopoietic stem cells. Am J Hematol 2007; 82(6): 463–472. http://doi.org/10.1002/ajh.20707
- Yalçın
C, Özkalemkaş F, Özkocaman V, Ersal T, Pınar İE, Orhan B, Candar Ö,
Çubukçu S, Koca TG, Akyol MN, Ada NG, Özakın C, Kazak E, Akalın H, Ali
R. Evaluation of using empiric glycopeptides in accordance with the
IDSA guidelines in hematologic malignancy patients with febrile
neutropenia. Mediterr J Hematol Infect Dis 2022; 14(1): e2022039. http://doi.org/10.4084/MJHID.2022.039
- Donnelly
JP, Chen SC, Kauffman CA, Steinbach WJ, Baddley JW, Verweij PE, Clancy
CJ, Wingard JR, Lockhart SR, Groll AH, Sorrell TC, Bassetti M, Akan H,
Alexander BD, Andes D, Azoulay E, Bialek R, Bradsher RW, Bretagne S,
Calandra T, Caliendo AM, Castagnola E, Cruciani M, Cuenca-Estrella M,
Decker CF, Desai SR, Fisher B, Harrison T, Heussel CP, Jensen HE,
Kibbler CC, Kontoyiannis DP, Kullberg BJ, Lagrou K, Lamoth F,
Lehrnbecher T, Loeffler J, Lortholary O, Maertens J, Marchetti O, Marr
KA, Masur H, Meis JF, Morrisey CO, Nucci M, Ostrosky-Zeichner L, Pagano
L, Patterson TF, Perfect JR, Racil Z, Roilides E, Ruhnke M, Prokop CS,
Shoham S, Slavin MA, Stevens DA, Thompson GR, Vazquez JA, Viscoli C,
Walsh TJ, Warris A, Wheat LJ, White PL, Zaoutis TE, Pappas PG. Revision
and update of the consensus definitions of invasive fungal disease from
the European organization for research and treatment of cancer and the
mycoses study group education and research consortium. Clin Infect Dis
2020; 71(6): 1367–1376. http://doi.org/10.1093/cid/ciz1008
- Sorror
ML, Maris MB, Storb R, Baron F, Sandmaier BM, Maloney DG, Storer B.
Hematopoietic cell transplantation (HCT)-specific comorbidity index: a
new tool for risk assessment before allogeneic HCT. Blood 2005; 106(8):
2912–2919. http://doi.org/10.1182/blood-2005-05-2004
- European
Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint
tables for interpretation of MICS and zone diameters. Version 14.0,
2024. https://www.eucast.org/clinical_breakpoints. Accessed January 1, 2025.
- Centers
for Disease Control and Prevention (CDC). Healthcare-Associated
Infections (HAIs). Carbapenem-resistant Enterobacterales (CRE)
Technical Information. https://www.cdc.gov/cre/hcp/infection-control/index.html. Accessed April 12, 2024.
- Valentini,
CG, Chiusolo P, Bianchi M, Metafuni, E, Orlando, N, Giammarco, S,
Bacigalupo, A, Sica, S, Teofili, L. Coronavirus disease 2019 pandemic
and allogeneic hematopoietic stem cell transplantation: a single center
reappraisal. Cytotherapy 2021; 23(7), 635–640. https://doi.org/10.1016/j.jcyt.2020.12.001
- Giammarco
S, Sica S, Metafuni E,Limongiello MA, Valentini CG, Sorà F, Marra JD,
Bacigalupo A, Teofili L, Chiusolo P. Impact of Covid COVID-19 pandemic
on hematopoietic stem cell transplantation activities: Report from a
single center. Transfus Apher Sci. 2023;62(4):103708. https://doi.org/10.1016/j.transci.2023.103708
- Tomblyn
M, Chiller T, Einsele H, Gress R, Sepkowitz K, Storek J, Wingard JR,
Young JA, Boeckh MJ. Guidelines for preventing infectious complications
among hematopoietic cell transplantation recipients: a global
perspective. Biol Blood Marrow Transplant 2009; 15(10): 1143–1238. http://doi.org/10.1016/j.bbmt.2009.06.019
- Valentini CG, Pellegrino C, Teofili L. Pros and Cons of Cryopreserving Allogeneic Stem Cell Products. Cells 2024; 21;13(6):552. https://doi.org/10.3390/cells13060552
- Styczyński
J, Tridello G, Koster L, Iacobelli S, van Biezen A, van der Werf S,
Mikulska M, Gil L, Cordonnier C, Ljungman P, Averbuch D, Cesaro S, de
la Camara R, Baldomero H, Bader P, Basak G, Bonini C, Duarte R, Dufour
C, Kuball J, Lankester A, Montoto S, Nagler A, Snowden JA, Kröger N,
Mohty M, Gratwohl A. Death after hematopoietic stem cell
transplantation: changes over calendar year time, infections and
associated factors. Bone Marrow Transplant 2020; 55(1): 126–136. http://doi.org/10.1038/s41409-019-0624-z
- Islas-Muñoz
B, Volkow-Fernández P, Silva-Zamora J, Ramírez-Ibarguen A,
Cornejo-Juárez P. Mortality in patients with hematological
malignancies, febrile neutropenia, and septic shock. J Infect Dev
Ctries 2024; 18(2): 235–242. http://doi.org/10.3855/jidc.17451
- Cao
W, Guan L, Li X, Zhang R, Li L, Zhang S, Wang C, Xie X, Jiang Z, Wan D,
Chi X. Clinical analysis of bloodstream infections during
agranulocytosis after allogeneic hematopoietic stem cell
transplantation. Infect Drug Resist 2021; 14: 185–192. http://doi.org/10.2147/IDR.S280869
- Nesher
L, Rolston KVI. Febrile neutropenia in transplant recipients. In:
Safdar A (ed). Principles and Practice of Transplant Infectious
Diseases. 1st ed. New York: Springer; 2018: 185–198. http://doi.org/10.1007/978-1-4939-9034-4_9
- Zhang
R, Xiong Y, Zhang L, Liu L. Epidemiology, microbiology, and risk
factors of bacterial bloodstream infections in patients after
allogeneic hematopoietic stem cell transplantation. Infect Drug Resist
2024; 17: 1561–1569. http://doi.org/10.2147/IDR.S451781
- Herrera
F, Torres D, Laborde A, Jordán R, Berruezo L, Roccia Rossi I, Mañez N,
Tula L, Pereyra ML, Nenna A, Costantini P, Benso J, González Ibañez ML,
Eusebio MJ, Baldoni N, Barcán LA, Lambert S, Luck M, Pasterán F, Corso
A, Rapoport M, Nicola F, García Damiano MC, Monge R, Carbone R,
Reynaldi M, Greco G, Blanco M, Chaves ML, Bronzi M, Carena A.
Epidemiology of bacteremia in patients with hematological malignancies
and hematopoietic stem cell transplantation and the impact of
antibiotic resistance on mortality: data from a multicenter study in
Argentina. Pathogens 2024; 13(11): 933. http://doi.org/10.3390/pathogens13110933
- Girmenia
C, Bertaina A, Piciocchi A, Perruccio K, Algarotti A, Busca A, Cattaneo
C, Raiola AM, Guidi S, Iori AP, Candoni A, Irrera G, Milone G, Marcacci
G, Scimè R, Musso M, Cudillo L, Sica S, Castagna L, Corradini P,
Marchesi F, Pastore D, Alessandrino EP, Annaloro C, Ciceri F, Santarone
S, Nassi L, Farina C, Viscoli C, Rossolini GM, Bonifazi F, Rambaldi A.
Incidence, risk factors and outcome of pre-engraftment gram-negative
bacteremia after allogeneic and autologous hematopoietic stem cell
transplantation: an Italian prospective multicenter survey. Clin Infect
Dis 2017; 65(11): 1884–1896. http://doi.org/10.1093/cid/cix690
- Gill
J, Busca A, Cinatti N, Passera R, Dellacasa CM, Giaccone L, Dogliotti
I, Manetta S, Corcione S, De Rosa FG. Bacterial bloodstream infections
after allogeneic hematopoietic stem cell transplantation: etiology,
risk factors and outcome in a single-center study. Microorganisms 2023;
11(3): 742. http://doi.org/10.3390/microorganisms11030742
- Ogura
S, Kimura M, Takagi S, Mitsuki T, Yuasa M, Kageyama K, Kaji D, Nishida
A, Taya Y, Ishiwata K, Yamamoto H, Asano-Mori Y, Yamamoto G, Uchida N,
Wake A, Taniguchi S, Araoka H. Characteristics of gram-negative
bacteremia during febrile neutropenia am10ong allogeneic hematopoietic
stem cell transplant recipients on levofloxacin prophylaxis. Eur J Clin
Microbiol Infect Dis 2021; 40(5): 941–948. http://doi.org/10.1007/s10096-020-04096-z
- Pagano
L, Caira M, Nosari A, Van Lint MT, Candoni A, Offidani M, Aloisi T,
Irrera G, Bonini A, Picardi M, Caramatti C, Invernizzi R, Mattei D,
Melillo L, de Waure C, Reddiconto G, Fianchi L, Valentini CG, Girmenia
C, Leone G, Aversa F. Fungal infections in recipients of hematopoietic
stem cell transplants: results of the SEIFEM B-2004 study--Sorveglianza
Epidemiologica Infezioni Fungine Nelle Emopatie Maligne. Clin Infect
Dis 2007; 45(9): 1161–1170. http://doi.org/10.1086/522189
- Quattrone
M., Di Pilla A., Brunetti S., Giordano A., Fianchi L., Pagano L.,
Criscuolo M. Managing invasive fungal infections during allogeneic
hematopoietic transplantation: A2025Update. Mediterr J Hematol Infect
Dis 2025, 17(1): e2025064, http://dx.doi.org/10.4084/MJHID.2025.064
- Neofytos
D, Horn D, Anaissie E, Steinbach W, Olyaei A, Fishman J, Pfaller M,
Chang C, Webster K, Marr K. Epidemiology and outcome of invasive fungal
infection in adult hematopoietic stem cell transplant recipients:
analysis of multicenter prospective antifungal therapy (PATH) alliance
registry. Clin Infect Dis 2009; 48(3): 265–273. http://doi.org/10.1086/595846
- Biyun
L, Yahui H, Yuanfang L, Guo X, Wang D. Risk factors for invasive fungal
infections after haematopoietic stem cell transplantation: a systematic
review and meta-analysis. Clin Microbiol Infect 2024; 30(5): 601–610. http://doi.org/10.1016/j.cmi.2024.01.005
- Acosta-Medina
AA, Baranwal A, Johnson IM, Kharfan-Dabaja MA, Murthy H, Palmer JM,
Sproat L, Mangaonkar A, Shah MV, Hogan WJ, Litzow MR, Tefferi A,
Alkhateeb HB. Comparison of pretransplantation prediction models for
nonrelapse mortality in patients with myelofibrosis undergoing
allogeneic stem cell transplantation. Transplant Cell Ther 2023; 29(6):
360.e1–360.e8. http://doi.org/10.1016/j.jtct.2023.02.002
- Bayraktar
UD, Shpall EJ, Liu P, Ciurea SO, Rondon G, de Lima M, Cardenas-Turanzas
M, Price KJ, Champlin RE, Nates JL. Hematopoietic cell
transplantation-specific comorbidity index predicts inpatient mortality
and survival in patients who received allogeneic transplantation
admitted to the intensive care unit. J Clin Oncol 2013; 31(33):
4207–4214. http://doi.org/10.1200/JCO.2013.50.5867
- Yuan
Y, Yang Y, Tian Y, Park J, Dai A, Roberts RM, Liu Y, Han X. Efficient
long-term cryopreservation of pluripotent stem cells at -80 °C. Sci
Rep. 2016;6:34476. https://doi.org/10.1038/srep34476
- Pinar
IE, Sahin M, Gursoy V, Ersal T, Budak F, Ozkocaman V, Ozkalemkas F.
Viable and Functional: Long-Term -80 °C Cryopreservation Sustains
CD34+Integrity and Transplant Success. J Clin Med. 2025;14(19):7032. https://doi.org/10.3390/jcm14197032