The patient, a 31-year-old woman, had been diagnosed with CLL (Binet B, Rai III, A group). She was treated with Zanubrutinib. She had a good response, and her condition has remained stable at a dose of 160mg twice daily for more than 2 years. On October 3, 2024, the patient was admitted to the emergency department due to a sudden onset of fever. Bilateral tonsillar enlargement was noted, along with multiple painless lymphadenopathies in the neck, right axilla, and inguinal region. The patient had a persistent high fever, with a maximum body temperature of 40.9°C. Laboratory tests showed: hypersensitive C-reactive protein (hs-CRP) 56.94mg/L (normal range 0-4 mg/L), white blood cell (WBC) count 11.98 x 109/L(normal range 3.69-9.16 x 109/L), absolute neutrophil count 6.92 x 109/L (normal range: 2.04-8.1 x 109/L), absolute lymphocyte count: 4.28 x 109/L (normal range: 0.8-4.32 x 109/L), absolute monocyte absolute count 0.46 x 109/L (normal range: 0.12-0.86 x 109/L), absolute eosinophil count 0.28 x 109/L (normal range: 0.2-0.54 x 109/L), absolute basophil count 0.04 x 109/L (normal range: 0.01-0.11 x 109/L), HGB 105g/L (normal range 113-151g/L), platelet was at normal range, the procalcitonin (PCT) 0.36ng/ml (normal range ≤0.1 ng/ml), and negative blood cultures. The globulin level was 45.1 g/L (normal range: 20-40g/L). Serological tests for mycoplasma and chlamydia were negative; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), respiratory syncytial virus (RSV), influenza A, influenza B viruses, and Epstein-Barr virus (EBV) tests were all negative. Her liver and kidney functions were normal. Chest computed tomography (CT) showed small patchy areas of increased density in the bilateral lower lungs. She was administered anti-infective treatment with ceftazidime at a dose of 3g intravenously every 12 hours. However, there was no reduction in body temperature after 4 days of treatment.
Upon detailed inquiry of the patient and her family, it was revealed that the patient had recently taken in stray cats and dogs. However, she denied any definite history of scratches from cats or dogs, and no scratch marks were found during physical examination. Given the possibility of infection with atypical pathogens or rare pathogenic bacteria, a TORCH test (Toxoplasma gondii, rubella virus, cytomegalovirus, and herpes simplex virus) was performed, with negative results. Ferritin level was tested at 73.6 ng/mL (normal range 11-306 ng/mL), and ceftazidime was replaced with moxifloxacin 0.4g once daily. Meanwhile, metagenomic next-generation sequencing (mNGS) of peripheral blood was performed. The results indicated 38 Bartonella henselae sequences, with a relative abundance of 71.765%. Our hospital is unable to perform polymerase chain reaction (PCR) or serology tests for CSD, and the patient refused out-of-hospital self-funded tests for the condition. Combining the patient's medical history and laboratory findings, a diagnosis of CSD was considered.
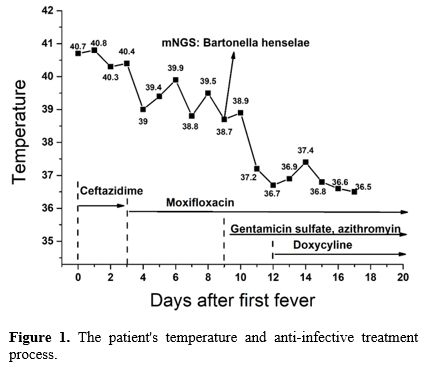
The anti-infective regimen was adjusted to a combination of moxifloxacin, gentamicin sulfate, azithromycin, and doxycycline. After 6 days of treatment, the patient's body temperature gradually decreased and returned to normal, inflammatory markers improved compared with previous results, and the lymphadenopathies observed during physical examination shrank. The patient was then discharged from the hospital and educated to avoid any contact with cats (including stray, domestic, or other cats) going forward. She continued the oral antibiotic treatment for 1 month after discharge and had no recurrence of fever thereafter. Her globulin level decreased and then increased again because she discontinued Zanubrutinib on her own initiative, so psychological counseling was recommended for her. The changes in her body temperature and the anti-infective treatment process are shown in Figure 1.
 |
|
CSD is a zoonotic infection caused by Bartonella henselae, transmitted primarily through scratches or bites from infected cats (especially kittens), but sometimes through fleas without cat scratches or bites.[6] CSD usually infects children younger than 18 years old, while immunocompromised adults are also susceptible.[7] Young patients of CLL often have unique clinical characteristics (e.g., aggressive biological features, shorter survival, and shorter time to treatment, a higher proportion of non-white patients) and face distinct challenges, such as long-term treatment-related toxicity and impact on quality of life. Therefore, more complications are anticipated.[8]
The symptoms of CSD include swollen and tender lymph nodes, fever, skin pustules, headache, and fatigue etc. Among these manifestations, lymphadenopathy is the most typical, though not specific, and is often misdiagnosed as other conditions.[9] The overlap of symptoms between CLL and CSD creates significant diagnostic challenges. For patients with CLL, Richter’s syndrome must be ruled out. Razaq M. et al. reported a case of CLL in which CSD mimicked Richter’s syndrome: the patient was a 52-year-old male diagnosed with CLL 2 months prior, who presented with rapidly enlarging lymph nodes and systemic symptoms such as night sweats, fever, and weight loss. Lymph node biopsy showed no evidence of high-grade lymphoma, thus excluding Richter’s syndrome. CSD was then suspected and subsequently confirmed via serological testing.[10]
In CLL patients with fever, infection should be excluded before performing a lymph node biopsy to assess the risk of Richter’s syndrome. This is because infection is the most common cause of fever in CLL patients.[5] In our case, the patient’s CLL condition remained stable after treatment with Zanubrutinib, and her WBC count was comparable to the level before this hospitalization. Therefore, we attributed her fever and lymphadenopathy to an underlying infection rather than disease progression. There is no gold standard for diagnosing CSD. The serology test is commonly used for CSD, as other diagnostic methods may require specialized equipment. However, the serology test exhibits variability in sensitivity and specificity. IgG titers >1:256 are considered diagnostic. PCR has been reported to be less variable: one study demonstrated that, among patients definitively diagnosed with CSD, PCR yielded a sensitivity of 76% and a specificity of 100%. However, PCR is more suitable for diagnosis rather than screening. Consequently, clinicians depend on a set of criteria to establish a definitive diagnosis.[11] NGS has become a powerful tool for diagnosing fever, particularly FUO, by identifying a wide range of pathogens that are often missed by traditional methods and overcomes the limitations of traditional methods by enabling unbiased, high-sensitivity detection of pathogens which is also useful for CSD.[12]
The treatment of CSD patients with concurrent CLL differs from that of patients with CSD alone. Due to their impaired immunity, these patients require individualized treatment, combined drug therapy, and a sufficient course of treatment. For ordinary CSD patients, a single antibiotic (such as azithromycin) administered for approximately 5 days is usually sufficient to control the disease. In contrast, for CSD patients with concurrent CLL, combined medication with drugs like rifampin, trimethoprim-sulfisoxazole, and ciprofloxacin is necessary, and the treatment course can last for one month or longer. This duration depends on factors such as the patient's clinical manifestations, imaging findings, and immune status, and close monitoring is required throughout treatment.[13]
In summary, while cat ownership offers numerous mental, physical, and social benefits, patients with CLL should be informed of potential infection sources — such as Bartonella henselae transmitted by cats — even in the absence of scratches or bites. For CLL patients presenting with FUO, atypical pathogens must be considered. A detailed history taking (including pet ownership history) and a thorough physical examination are therefore vital for identifying diagnostic clues. Diversified detection methods, particularly NGS, should be employed to identify the underlying pyrogen. Young CLL is already uncommon, and co-infection with CSD adds diagnostic complexity — clinicians should maintain a high index of suspicion for infections in young CLL patients with new lymphadenopathy or systemic symptoms. Meanwhile, individualized management strategies are essential, including extending treatment courses for immunocompromised patients beyond those recommended for immunocompetent individuals, as well as providing psychological support for patients who may need to give up their pet cats. Given that cats are common pets and the tourism industry has developed, CSD should not be overlooked even in non-endemic regions — especially among immunocompromised patients such as those with CLL.
Declarations
Written informed consent was obtained from the patient.Acknowledgement
This work was supported by the 2025 Tianchi Talent Project of Xinjiang Uygur Autonomous Region.Authors’ contributions
C.L. and X.Y. collected and analyzed the data and wrote the paper; L.D. and Y.Z. helped collect data; H.Z. helped analyze the data and revised the paper.Data Availability Statement
The datasets are available from the corresponding author (Dr. Luan, luanchengxinxjb@163.com) on reasonable request.References
- Hallek M. Chronic Lymphocytic Leukemia: 2025 Update
on the Epidemiology, Pathogenesis, Diagnosis, and Therapy. American
Journal of Hematology. 2025;100(3). https://doi.org/10.1002/ajh.27546 PMid:39871707 PMCid:PMC11803567
- Tian
Z, Liu M, Fang X, Zhou X, Li P, Li Y, et al. Distinct Age-Related
Clinical Features and Risk Assessment in Chinese With Chronic
Lymphocytic Leukemia. Frontiers in Oncology. 2022;Volume 12 - 2022. https://doi.org/10.3389/fonc.2022.885150 PMid:35646669 PMCid:PMC9135454
- Sachanas
S, Vassilakopoulos T, Angelopoulou M, Papageorgiou S, Spanoudakis E,
Bouzani M, et al. Greek Consensus on Chronic Lymphocytic Leukemia (CLL)
Treatment. Mediterr J Hematol Infect Dis. 2025;17(1):e2025014. https://doi.org/10.4084/MJHID.2025.014 PMid:40084092 PMCid:PMC11906138
- Sun
C, Wiestner A. Can Immunocompetence Be Restored in Chronic Lymphocytic
Leukemia? Hematol Oncol Clin North Am. 2021;35(4):827-45. https://doi.org/10.1016/j.hoc.2021.03.010 PMid:34174988 PMCid:PMC8269747
- Guarana M, Nucci M. Infections in patients with chronic lymphocytic leukemia. Hematol Transfus Cell Ther. 2023;45(3):387-93. https://doi.org/10.1016/j.htct.2023.05.006 PMid:37407362 PMCid:PMC10499585
- Puspitasari
Y, Khairullah AR, Raharjo HM, Fauziah I, Tyasningsih W, Kurniasih DAA,
et al. Uncovering the truth about cat-scratch disease. Open Vet J.
2025;15(5):1895-906. https://doi.org/10.5455/OVJ.2025.v15.i5.5 PMid:40557109 PMCid:PMC12184452
- Oksi
J, Rantala S, Kilpinen S, Silvennoinen R, Vornanen M, Veikkolainen V,
et al. Cat scratch disease caused by Bartonella grahamii in an
immunocompromised patient. J Clin Microbiol. 2013;51(8):2781-4. https://doi.org/10.1128/JCM.00910-13 PMid:23740723 PMCid:PMC3719609
- Parikh
SA, Rabe KG, Kay NE, Call TG, Ding W, Schwager SM, et al. Chronic
lymphocytic leukemia in young (≤ 55 years) patients: a comprehensive
analysis of prognostic factors and outcomes. Haematologica.
2014;99(1):140-7. https://doi.org/10.3324/haematol.2013.086066 PMid:23911703 PMCid:PMC4007929
- Dhal
U, Hicklen RS, Tarrand J, Kontoyiannis DP. Cat Scratch Disease as a
Mimicker of Malignancy. Open Forum Infect Dis. 2021;8(11):ofab500. https://doi.org/10.1093/ofid/ofab500 PMid:34926712 PMCid:PMC8675392
- Razaq
M, Godkar D, Mankan N, Sridhar S, Hussain S, Ohri A. Cat scratch
disease mimicking Richter's Syndrome in a patient with chronic
lymphocytic leukemia. Leuk Lymphoma. 2005;46(3):443-5. https://doi.org/10.1080/10428190400004489 PMid:15621836
- Khalfe N, Lin D. Diagnosis and interpretation of testing for cat scratch disease. Proc (Bayl Univ Med Cent). 2022;35(1):68-9. https://doi.org/10.1080/08998280.2021.1984791 PMid:34970038 PMCid:PMC8682836
- Gao
Z, Jiang Y, Chen M, Wang W, Liu Q, Ma J. Enhancing fever of unknown
origin diagnosis: machine learning approaches to predict metagenomic
next-generation sequencing positivity. Front Cell Infect Microbiol.
2025;15:1550933. https://doi.org/10.3389/fcimb.2025.1550933 PMid:40302920 PMCid:PMC12037494
- Guiyedi
V, Haddad H, Okome-Nkoumou M, Gire F, Ongali B, Lore P, et al.
Cat-scratch disease in an adult hospitalized for prolonged-Fever
associated with multiple lymphadenopathies and weight loss. Open
Microbiol J. 2013;7:152-5. https://doi.org/10.2174/1874285801307010152 PMid:24403980 PMCid:PMC3882904