The typical features of TB (prolonged fever, systemic symptoms, and lymphadenopathy) often overlap with those of acute leukemia, leading to frequent diagnostic delays.[6,7] As a result, even in high-burden regions, clinicians may underestimate the possibility of TB reactivation, and imaging findings suggestive of TB are often attributed to fungal or bacterial infections or leukemic infiltration unless confirmed otherwise.[8] Metagenomic next-generation sequencing (mNGS) has emerged as a valuable tool for rapid and accurate TB diagnosis, particularly in immunocompromised hosts.[9,10] In a study of 48 patients with suspected disseminated TB, blood-based mNGS identified 28 cases and showed higher MTB detection rates in patients with elevated procalcitonin, HIV co-infection, and low CD4 counts.[10] Immunosuppression increases the complexity of tuberculosis management. While the WHO recommends that TB patients with HIV should not receive shorter treatment courses than their HIV-negative counterparts, the Infectious Diseases Society of America recommends up to 9 months of anti-tuberculosis therapy (ATT) for those not on antiretroviral therapy (ART) with drug-susceptible TB.[11,12] Both guidelines, however, lack specific recommendations for patients with hematological malignancies. A study of 59 patients with hematological malignancies who received ATT reported a median treatment duration of 9 months (range: 6-20), with no cases of tuberculosis relapse.[13] Evidence remains limited, underscoring the need for further research. Against this background, we report a case of hematogenously disseminated pulmonary TB in a patient with acute myeloid leukemia (AML), diagnosed by mNGS and successfully treated.
An 80-year-old Chinese man was admitted on March 26, 2024, with a recurrent fever for more than two months, accompanied by chills, fatigue, night sweats, weight loss, cough, dyspnea, palpitations, anorexia, and abdominal distention. Laboratory testing showed hemoglobin (HGB) 5.8 g/dL, red blood cells (RBC) 2.35 × 10¹²/L, white blood cells (WBC) 15.47 × 10⁹/L, neutrophils (NEUT) 2.59 × 10⁹/L, monocytes (MONO) 11.34 × 10⁹/L, and platelets (PLT) 112.4 × 10⁹/L. CT imaging confirmed pneumonia (Figure 1 A1, A2), and elevated procalcitonin, C-reactive protein, and IL-6 prompted empiric piperacillin-tazobactam. Bone marrow morphologic and flow cytometric evaluation confirmed acute myeloid leukemia (AML), M4 subtype (Figure 2). The latter revealed 14.33% primitive granulocytes and 45.65% primitive monocytes, which expressed CD13, CD33, cMPO, CD38, CD34, CD117, partial HLA-DR, CD36, CD11b, CD64, and CD14. Next-generation sequencing identified RUNX1, TET2, WT1, and ZRSR2 mutations. Cytogenetics showed a normal karyotype, and no common leukemia fusion genes were detected.
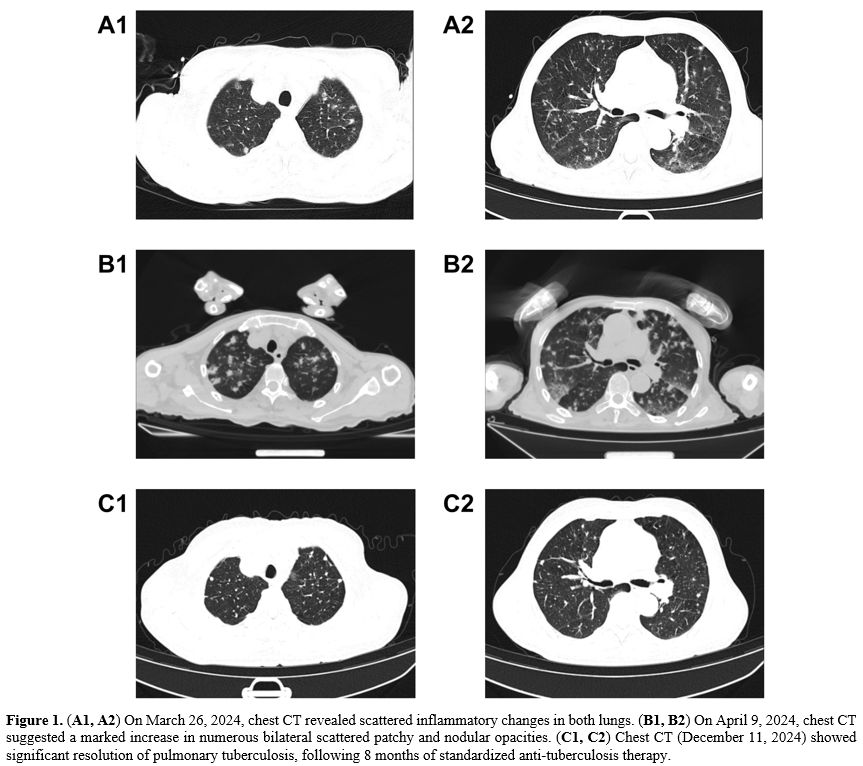 |
Figure 1. (A1, A2) On March 26, 2024, chest CT revealed scattered inflammatory changes in both lungs. (B1, B2) On April 9, 2024, chest CT suggested a marked increase in numerous bilateral scattered patchy and nodular opacities. (C1, C2) Chest CT (December 11, 2024) showed significant resolution of pulmonary tuberculosis, following 8 months of standardized anti-tuberculosis therapy. |
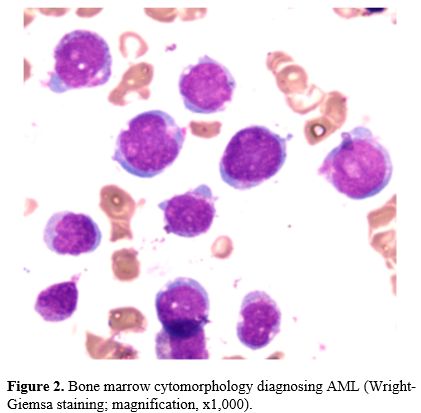 |
Figure 2. Bone marrow cytomorphology diagnosing AML (Wright-Giemsa staining; magnification, x1,000). |
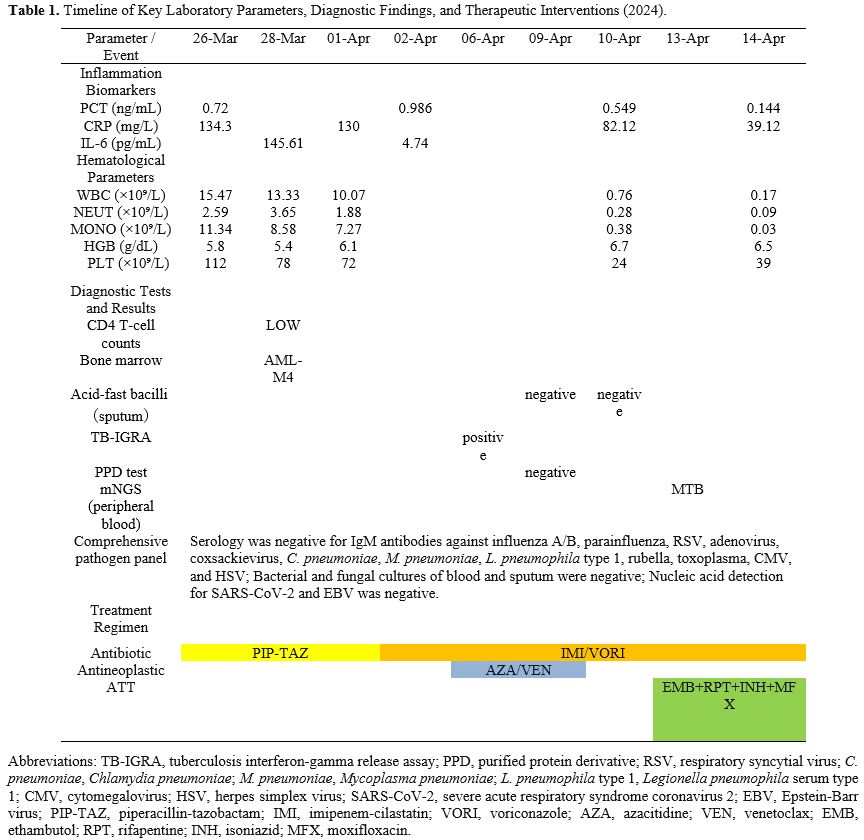
Due to persistent fever (peak temperature, 39.5°C) and unimproved inflammatory markers after a 7-day course of piperacillin-tazobactam, the antimicrobial regimen was escalated to imipenem-cilastatin combined with voriconazole. This change was motivated by concern for uncontrolled bacterial infection and possible fungal co-infection in the context of the patient's immunocompromised state. Continued fever after four days raised concern for tumor-associated fever, and azacitidine plus venetoclax was initiated on April 6, 2024. Daily afternoon fevers persisted, and positive TB serology and T-SPOT.TB prompted reevaluation. A repeat CT on April 9, 2024, showed rapidly progressive bilateral nodular and patchy opacities (Figure 1 B1, B2), consistent with hematogenous dissemination. On April 10, 2024, the patient developed agranulocytosis (NEUT 0.28 × 10⁹/L) and severe thrombocytopenia (PLT 24 × 10⁹/L), requiring cessation of chemotherapy. Peripheral blood mNGS on April 13, 2024, detected MTB complex (13.22% relative abundance; 11 reads), confirming hematogenously disseminated pulmonary TB. Under specialist guidance, ATT was initiated on April 13, 2024, consisting of ethambutol 0.75 g daily, rifapentine 0.45 g twice weekly, isoniazid 0.3 g daily, and moxifloxacin 0.4 g daily. Table 1 summarizes the patient's clinical course and key laboratory findings. After defervescence on therapy, the patient left the hospital against medical advice on April 15, 2024, despite severe bone marrow suppression. He remained on oral ATT and reported no recurrence of fever during the following week. After completing a two-month intensive phase, he entered a seven-month continuation phase with isoniazid, rifapentine, and ethambutol. Follow-up CT on December 11, 2024, showed complete resolution of the pulmonary lesions (Figure 1 C1, C2).
 |
|
In conclusion, this case highlights the characteristic imaging features of hematogenously disseminated pulmonary TB in AML and demonstrates the diagnostic value of mNGS in immunocompromised patients. It also provides practical insight into the management of TB co-infection in elderly patients with leukemia.
Ethics approval and consent to participate
The study protocol was approved by the Medical Ethics Committee of the First People’s Hospital of Zigong. The patient gave informed consent for the publication of this case report.References
- Advani SH, Banavali SD. Pattern of infection in
hematologic malignancies: an Indian experience. Rev Infect Dis. 1989;11
Suppl 7:S1621-8. https://doi.org/10.1093/clinids/11.Supplement_7.S1621 PMid:2602780
- Nunzi
A, Della Valle L, Lindfors Rossi EL, Ranucci G, Mallegni F, Moretti F,
Meddi E, Guarnera L, Tiravanti I, Taka K, Buzzatti E, Esposito F,
Secchi R, Di Giuliano F, Chirico F, Palmieri R, Maurillo L, Buccisano
F, Gurnari C, Paterno G, Venditti A, Del Principe MI. Acute Leukemia
and Latent Tuberculosis Infection in Italy: Quantiferon-Tb Test
Screening in a Low Tuberculosis Incidence Country. Mediterr J Hematol
Infect Dis. 2024;16:e2024054 https://doi.org/10.4084/MJHID.2024.054 PMid:38984098 PMCid:PMC11232683
- Dannenberg AM, Jr. Immune mechanisms in the pathogenesis of pulmonary tuberculosis. Rev Infect Dis. 1989;11 Suppl 2:S369-78. https://doi.org/10.1093/clinids/11.Supplement_2.S369 PMid:2496453
- Maison DP. Tuberculosis pathophysiology and anti-VEGF intervention. J Clin Tuberc Other Mycobact Dis. 2022;27:100300. https://doi.org/10.1016/j.jctube.2022.100300 PMid:35111979 PMCid:PMC8790470
- Li
F, Ma Y, Li X, Zhang D, Han J, Tan D, Mi Y, Yang X, Wang J, Zhu B.
Severe persistent mycobacteria antigen stimulation causes lymphopenia
through impairing hematopoiesis. Front Cell Infect Microbiol.
2023;13:1079774. https://doi.org/10.3389/fcimb.2023.1079774 PMid:36743311 PMCid:PMC9889370
- Wang
ST, Chen CL, Liang SH, Yeh SP, Cheng WC. Acute myeloid leukemia with
leukemic pleural effusion and high levels of pleural adenosine
deaminase: A case report and review of literature. Open Med (Wars).
2021;16:387-96. https://doi.org/10.1515/med-2021-0243 PMid:33748423 PMCid:PMC7957840
- Mkrtchyan S. Spinal Tuberculosis Mimicking Metastatic Lung Cancer: A Case of Misdiagnosis. Cureus. 2025;17:e91815. https://doi.org/10.7759/cureus.91815
- Jain
A, Prakash G, Singh C, Lad D, Khadwal A, Suri V, Malhotra P, Kumari S,
Varma N, Varma S. Analysis of Clinical Profile and Outcome of
Tuberculosis in Patients with Acute Leukemia. Indian J Hematol Blood
Transfus. 2018;34:430-42. https://doi.org/10.1007/s12288-017-0875-z PMid:30127549 PMCid:PMC6081343
- Yan
H, Wen Q, Zhang X. Refractory splenic tuberculosis in acute myeloid
Leukemia: The role of advanced diagnostics and surgical intervention. J
Clin Tuberc Other Mycobact Dis. 2025;40:100525. https://doi.org/10.1016/j.jctube.2025.100525 PMid:40469259 PMCid:PMC12133704
- Ma
J, Jiang Y, He Y, Zhou H. The value of metagenomic next-generation
sequencing with blood samples for the diagnosis of disseminated
tuberculosis. Front Cell Infect Microbiol. 2024;14:1456119. https://doi.org/10.3389/fcimb.2024.1456119 PMid:39717545 PMCid:PMC11663735
- Huang
T, Chen Q, Wu GH, Tang SJ. Interpretation of the World Health
Organization consolidated guidelines on tuberculosis Module 4:
treatment and care (2025 Edition). Zhonghua Jie He He Hu Xi Za Zhi.
2025;48:708-18.
- Nahid
P, Dorman SE, Alipanah N, Barry PM, Brozek JL, Cattamanchi A, Chaisson
LH, Chaisson RE, Daley CL, Grzemska M, Higashi JM, Ho CS, Hopewell PC,
Keshavjee SA, Lienhardt C, Menzies R, Merrifield C, Narita M, O'Brien
R, Peloquin CA, Raftery A, Saukkonen J, Schaaf HS, Sotgiu G, Starke JR,
Migliori GB, Vernon A. Official American Thoracic Society/Centers for
Disease Control and Prevention/Infectious Diseases Society of America
Clinical Practice Guidelines: Treatment of Drug-Susceptible
Tuberculosis. Clin Infect Dis. 2016;63:e147-e95. https://doi.org/10.1093/cid/ciw376 PMid:27516382 PMCid:PMC6590850
- Dewan
A, Singh R, Sachdeva I, Bhurani D, Agrawal N, Ahmed R, Halder R, Patra
PC, Debadwar SR, Bansal N. Tuberculosis and Hematological Malignancies:
Real-world Experience and Key Insights into Drug-Drug Interactions.
Journal of Clinical Infectious Diseases Society. 2023;1:227-32. https://doi.org/10.4103/CIDS.CIDS_20_23