The clinical spectrum of CMV ranges from asymptomatic reactivation to life-threatening organ involvement. In immunocompromised transplant cohorts, CMV syndrome (fever, malaise, and cytopenia) and CMV disease (organ involvement) are clearly defined.[4,5] Conversely, in critically ill patients, it is difficult to suspect and define CMV disease. At the same time, the necessity of monitoring CMV reactivation and the optimal strategies for treatment or prophylaxis remain unclear.[6]
In critically ill patients, CMV reactivation is associated with increased mortality, prolonged mechanical ventilation (MV), and extended hospital stay.[7-10] Evidence shows that mortality rates among patients with CMV reactivation are nearly double those without reactivation.[3,6] In critically ill patients, CMV reactivation can cause worse clinical outcomes with direct and indirect lung injury.[11] Recent data indicated that CMV pneumonitis may occur in approximately 50% of intensive care unit (ICU) patients with acute respiratory distress syndrome (ARDS). Furthermore, CMV reactivation may exacerbate the clinical course of ARDS. Given that the lungs are a primary site of latent CMV, understanding the relationship between CMV reactivation and the duration of mechanical ventilation is clinically important. [9,12,13]
Up to the present, risk factors such as high disease severity, prolonged ICU stay, MV, sepsis, steroid use, raised C-reactive protein (CRP), and lower hemoglobin have been associated with CMV reactivation in immunocompetent critically ill patients.[6,11,14]
Determining whether CMV reactivation is pathogenic or coincidental is crucial for guiding ICU management.[9] While an animal model suggests that ganciclovir blocks CMV reactivation and can prevent pulmonary fibrosis,[15] antiviral therapy in critically ill patients published to date has been limited.[16-18]
Although clinically significant, the definitive impact of CMV reactivation on outcomes in critically ill populations remains poorly defined, necessitating further investigation. This study aimed to identify risk factors for CMV reactivation by comparing patients who received antiviral therapy with those who did not. Additionally, we performed a subgroup analysis of patients with CMV reactivation to identify parameters associated with mortality.
Methods
Approval of the local ethics committee was obtained for this study (Confirmation date and number: 12.01.2022/ E1-22-2276). This study was conducted in accordance with the principles of the Declaration of Helsinki.Study Design and Participants. From February 1, 2021, to March 1, 2022, mechanically ventilated patients with COVID-19 were retrospectively screened. All patients included in this study (age ≥ 18 years) had no history of pre-existing immunosuppressive conditions such as hematological malignancy, solid organ transplantation, HIV infection, or long-term immunosuppressive therapy before ICU admission. Although COVID-19 itself and corticosteroids may exert immunomodulatory effects, patients were classified as immunocompetent based on the absence of established chronic immunosuppression before hospitalization. In the 24-bed ICU, patients (reactivation and control groups) who underwent CMV monitoring via quantitative polymerase chain reaction (PCR; Rotor-Gene Q, QIAGEN) weekly were included in the study. CMV reactivation was treatment-defined. Patients with a viral load threshold ≥1000 U/mL and assessed clinical conditions (fever, diarrhea, absence of bacterial diagnosis for pneumonia, cytopenia, and hepatitis) who received ganciclovir treatment (5 mg/kg twice daily for 14 days for induction, followed by 5 mg/kg once daily for maintenance) were included in the reactivation group. Nine patients with viral loads above 1000 copies/mL were not treated with ganciclovir because DNA levels decreased during follow-up, and no clinical indicators were present. Due to the very small number of patients, a control group could not be formed. The CMV reactivation group was matched to the control group according to the following criteria: age within ±10 years, similar SAPS (Simplified Acute Physiology Score), and admission date. The control group included patients with CMV PCR consistently <50 copies/mL monitored weekly.
Clinical data, outcomes, laboratory findings (hematological parameters, liver function tests, acute-phase reactants), and CMV PCR results were obtained from patients’ files and electronic medical records. The laboratory parameters were recorded twice (on admission and on the 14th day of treatment).
Statistical analysis. All statistical calculations were made using the “SPSS for Windows version 26” software program (IBM Corporation, IL). Comparisons for categorical variables were executed using the Pearson chi-square test or Fisher’s exact test. The Shapiro-Wilk test was performed to check the normality of the continuous variables. Differences between the two groups were compared using the Mann-Whitney U and Independent Samples T-tests. Multivariate logistic regression (Forward LR) was performed and found to be significant in the univariate analysis to assess the associated factors for CMV reactivation. The odds ratio (OR) was calculated for variables with significant associations. Receiver operating characteristic (ROC) curve analysis was performed to assess the efficacy of laboratory parameters. Statistical significance was defined as p<0.05.
Results
In total, 39 patients with CMV reactivation and 39 controls participated in the study. In the reactivation group, the day of steroid treatment, length of MV, cytopenia, and elevated liver function tests were significantly higher than in the control group. The reactivation group had significantly higher alanine aminotransferase (ALT) levels and lower hemoglobin levels (Table 1).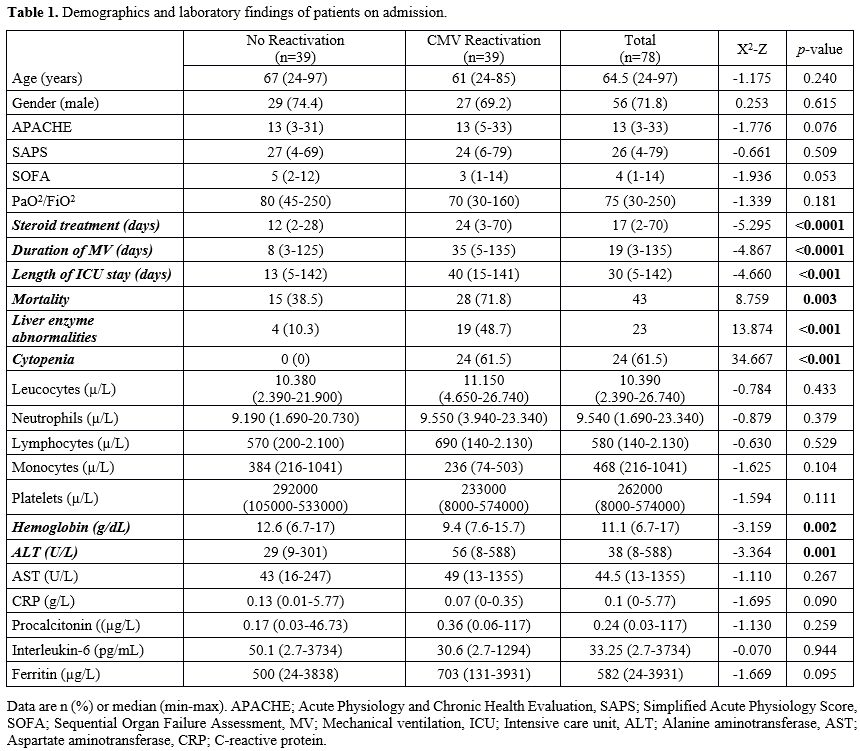 |
|
Univariate logistic regression analysis showed that ICU length of stay, the day of steroid treatment, MV duration, ALT, and hemoglobin levels were associated with reactivation. In the model created with the variables found to be significant in univariate logistic regression, it was found that the duration of MV, steroid treatment, and hemoglobin level had a statistically significant effect in the 4th step (p<0.05) (Nagelkerke R2 = 0.756), showing that the model has high explanatory power over the data (Table 2). After the ROC analysis for laboratory parameters, the optimal cut-off value of ALT was found to be >58 IU/ml (p<0.001, AUC: 0.721, sensitivity: 56.41, specificity: 87.18), and hemoglobin was found to be ≤ 9.8 g/dL (p<0.001, AUC: 0.708, sensitivity: 56.41, specificity: 84.62) (Figures 1 and 2).
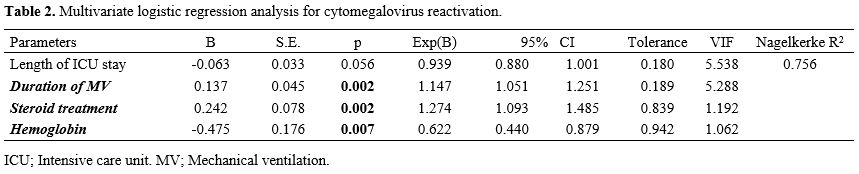 |
Table 2. Multivariate logistic regression analysis for cytomegalovirus reactivation. |
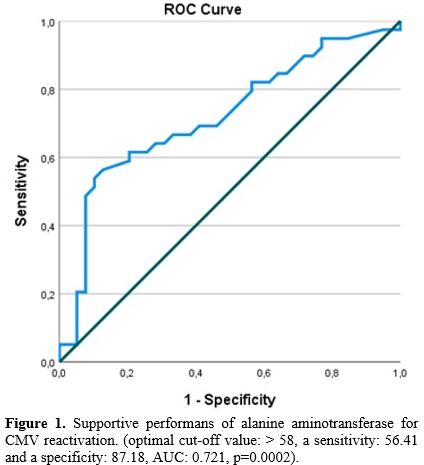 | Figure 1.
Supportive performans of alanine aminotransferase for CMV reactivation.
(optimal cut-off value: > 58, a sensitivity: 56.41 and a
specificity: 87.18, AUC: 0.721, p=0.0002). |
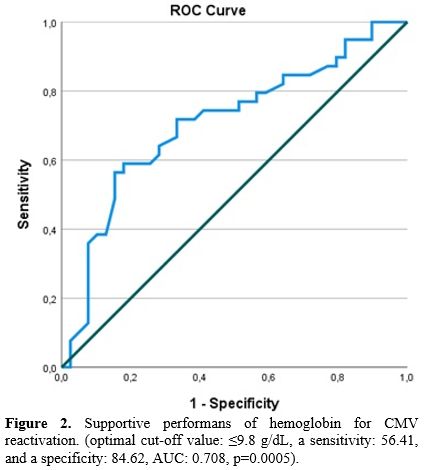 |
Figure 2. Supportive performans of hemoglobin for CMV reactivation. (optimal cut-off value: ≤9.8 g/dL, a sensitivity: 56.41, and a specificity: 84.62, AUC: 0.708, p=0.0005). |
The reactivation group had higher mortality rates (n=28, 71.8%) than the control group (n=15, 28.5%). The patients with CMV reactivation were analyzed into non-survivor (n=28) and survivor (n=11) groups. In the non-survivor group, no patients achieved successful weaning from mechanical ventilation (MV), a finding that was statistically significant compared with survivors (p<0.001). Higher CRP levels and lower monocytes and platelets were found in the non-survivor group on admission. On the 14th day of the treatment, higher aspartate aminotransferase (AST), CRP, procalcitonin, IL-6, ferritin, and lower lymphocytes and platelets were found in the non-survivor group (Tables 3 and 4).
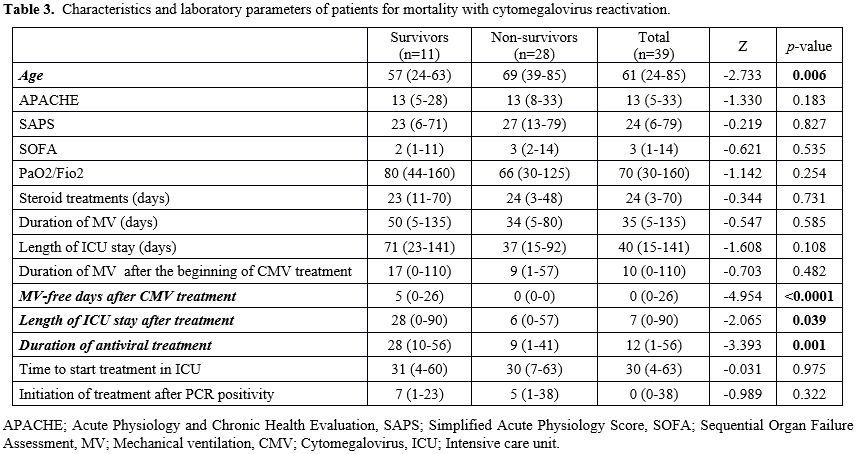 |
Table 3. Characteristics and laboratory parameters of patients for mortality with cytomegalovirus reactivation. |
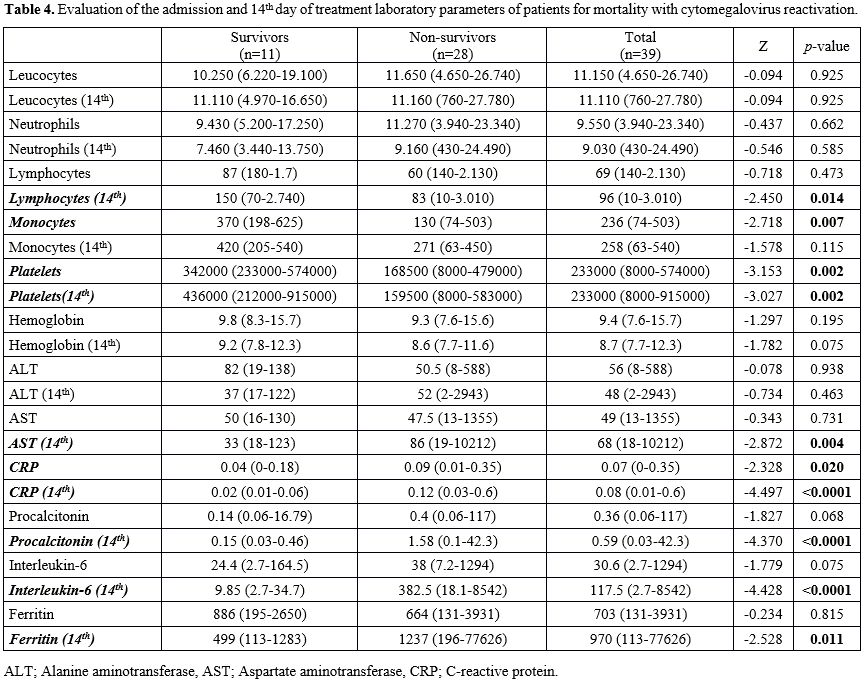 |
Table 4.
Evaluation of the admission and 14th day of treatment laboratory
parameters of patients for mortality with cytomegalovirus reactivation. |
Mean±SD value of CMV DNA levels of patients with CMV reactivation is shown in Table 5. Baseline DNA (mean±SD) levels were higher in the non-survivor group, but no statistically significant difference was detected. A downward trend was seen in both groups (Figure 3).
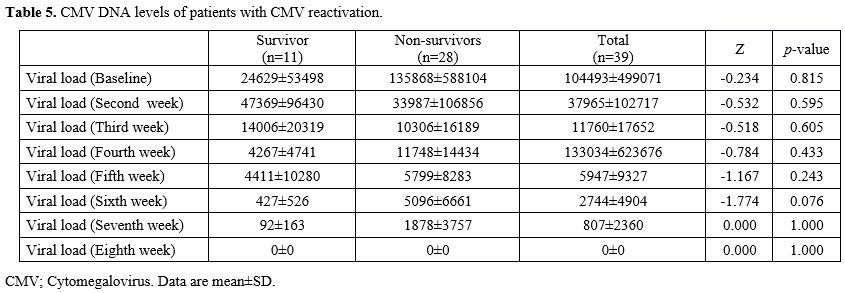 |
Table 5. CMV DNA levels of patients with CMV reactivation. |
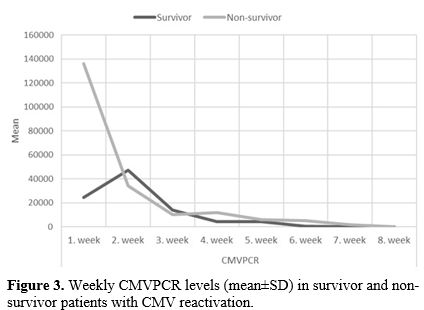 |
Figure 3. Weekly CMVPCR levels (mean±SD) in survivor and non-survivor patients with CMV reactivation. |
Discussion
CMV reactivation in this cohort was linked to extended ICU stay and prolonged MV. Lower Hb levels were associated with CMV reactivation. Based on these results, critically ill patients with prolonged hospitalization and mechanical ventilation should be monitored for CMV reactivation. Clinicians should maintain a higher index of suspicion for CMV reactivation in patients presenting with supportive laboratory indicators, such as decreased hemoglobin and elevated ALT levels. While these parameters lack primary diagnostic specificity, they may serve as useful signals to initiate closer virological monitoring.In this study, the baseline CMV DNA level was higher in non-survivor patients than in survivors in the reactivation group. However, during follow-up, CMV levels declined similarly in both survivors and non-survivors, eventually reaching undetectable levels in both groups. This finding suggested that, while initial DNA levels are a marker of severity, viremia clearance occurs regardless of clinical outcome. However, it is essential to recognize that clinical outcomes in critically ill patients are multifactorial and are significantly influenced by a wide array of confounding variables beyond viral reactivation.
There are significant uncertainties regarding CMV infection in immunocompetent critically ill patients monitored in intensive care units. CMV reactivation episodes, during critical illness, are associated with worsened outcomes.[8] CMV reactivation has been shown in many studies to increase mortality, duration of intensive care, and mechanical ventilation.[5,19,20] In a meta-analysis, all-cause mortality of patients with CMV reactivation was 2.16-fold higher compared with those without infection.[10] A systematic review including 13 studies (n=1258) revealed that the mortality rate is significantly increased by 2-fold with CMV.[3] In this study, mortality was found to be higher in patients with reactivation than in those with no reactivation (71.8% vs. 38.5%, p=0.003). The duration of MV was found to be associated with reactivation. (OR:1.15). Heininger et al. reported that prolonged MV (HR: 2.6) was associated with CMV reactivation.[21] Steroid use was found to be another factor contributing to reactivation in this study, consistent with previous reports in the literature.[5,19] In this study, all patients were treated with steroids, so the duration of steroid treatment was evaluated, and it was found that steroid treatment was associated with reactivation (OR: 1.27, p<0.001).
Immunocompetent ICU patients in whom CMV reactivation is frequently underrecognized and rarely considered in the differential diagnosis of worsening breathing and unexplained cytopenias. In this study, a lower hemoglobin level was defined as an associated factor for reactivation. Cytopenia is part of CMV syndrome, and lower hemoglobin levels have previously been identified as a predictor of reactivation.[3,14,22] Zhang et al. reported that AST and hemoglobin levels were found to be higher in patients with CMV reactivation.[22] They also found that hemoglobin was a predictor of reactivation. (with the cut-off:≤ 8.7 g/dL, p=0.02, AUC: 0.70, sensitivity: 100, specificity: 48.3). In this study, the optimal cut-off value for hemoglobin level≤9.8 g/dL was found to have a limited sensitivity of 56.41% and specificity of 84.62% (p<0.001, AUC: 0.708) for CMV reactivation.[14] This study also showed that ALT levels increase during reactivation. However, ALT may be considered a non-specific marker because its elevation may reflect certain conditions such as drug-induced liver injury, hypoxic hepatitis, and COVID-19-related inflammation. But in the intensive care, making a clear distinction between these conditions is often not possible.
The diagnosis of CMV infection is difficult in ICU patients because clinical signs are nonspecific.[5] Plasma CMV viral load is used by clinicians to guide initiation of antiviral treatment and to monitor treatment response.[3] In this study, although the initial viral load was higher in survivors, the course of viral load during follow-up was similar in survivors and non-survivors. This observation hypothesis-generating suggests whether weekly viral load monitoring is necessary or not in patients who have received treatment.
Antiviral therapy for CMV in critically ill patients published to date has been limited. Some experts recommend against antiviral therapy in critically ill immunocompetent patients.[8] However, others suggested that regular viral load monitoring of patients in the ICU, and treatment initiated only in those patients with viral reactivation above a certain threshold.[9,23] Hraiech et al. reported that no difference in clinical outcomes was found between treated (n=34) and untreated (n=33) patients with herpes virus reactivation, except for a trend towards longer duration of MV.[12] The question of whether treatment should be initiated in patients with CMV reactivation remains. Since there was no comparator group (untreated CMV-positive patients) in this study, it is not possible to comment on the treatment's effectiveness. However, given the high mortality rate observed, the treatment's clinical benefit is debatable. On the other hand, it should be noted that CMV reactivation may be an indicator of immune dysfunction and disease severity rather than a direct cause of poor outcomes. Randomized controlled trials are needed on these subject issues.
Several limitations of this study warrant consideration. First, its retrospective nature and a relatively small sample size (n=78) may limit the statistical power of the findings. Second, there is potential selection bias, as the reactivation group was defined by the initiation of antiviral therapy. This treatment-dependent definition may have led to an overestimation of the association between CMV reactivation and clinical outcomes. Furthermore, the limited number of untreated patients with CMV reactivation (n=9) precluded the determination of a definitive viral load cut-off value or a comparative analysis. Finally,as the study population was focused on patients with severe COVID-19, the generalizability of the findings to other critically ill cohorts remains to be established.
Conclusion
CMV reactivation is observed in critically ill patients; therefore, it should be considered and monitored in those with extended ICU stays and prolonged mechanical ventilation. Furthermore, lower hemoglobin and elevated ALT levels may serve as valuable laboratory indicators, aiding in the early clinical suspicion of reactivation.References
- Olivari E, Pavoni C, Algarotti A, Micò MC, Finazzi
MC, Cavallaro G, Rambaldi B, Rizzuto G, Lussana F, Rambaldi A. CMV
Reactivations During and After Letermovir Prophylaxis in Allogeneic
Hematopoietic Stem Cell Transplantation: A Single-Center Experience.
Mediterr J Hematol Infect Dis. 2025;17(1):e2025079. https://doi.org/10.4084/MJHID.2025.079 PMid:41235027 PMCid:PMC12611361
- Schattner
A. The wide spectrum of presentations of cytomegalovirus infection in
immunocompetent hosts: an exhaustive narrative review. Pathogens.
2024;13(8):667. https://doi.org/10.3390/pathogens13080667 PMid:39204267 PMCid:PMC11357360
- Kalil
AC, Florescu DF. Prevalence and mortality associated with
cytomegalovirus infection in nonimmunosuppressed patients in the
intensive care unit. Crit Care Med. 2009;37(8):2350-8. https://doi.org/10.1097/CCM.0b013e3181a3aa43 PMid:19531944
- Kalil
AC, Levitsky J, Lyden E, Stoner J, Freifeld AG. Meta-analysis: the
efficacy of strategies to prevent organ disease by cytomegalovirus in
solid organ transplant recipients. Ann Intern Med. 2005;143(12):870-80.
https://doi.org/10.7326/0003-4819-143-12-200512200-00005 PMid:16365468
- Chiche
L, Forel J-M, Roch A, Guervilly C, Pauly V, Allardet-Servent J,
Gainnier M, Zandotti C, Papazian L. Active cytomegalovirus infection is
common in mechanically ventilated medical intensive care unit patients.
Crit Care Med. 2009;37(6):1850-7. https://doi.org/10.1097/CCM.0b013e31819ffea6 PMid:19384219
- Bhide
M, Singh O, Nasa P, Juneja D. Cytomegalovirus infection in
non-immunocompromised critically ill patients: A management
perspective. World J Virol. 2024;13(1). https://doi.org/10.5501/wjv.v13.i1.89135 PMid:38616856 PMCid:PMC11008403
- Osawa R, Singh N. Cytomegalovirus infection in critically ill patients: a systematic review. Critical Care. 2009;13:1-10. https://doi.org/10.1186/cc7875 PMid:19442306 PMCid:PMC2717427
- Cook
CH, Trgovcich J. Cytomegalovirus reactivation in critically ill
immunocompetent hosts: a decade of progress and remaining challenges.
Antiviral Res. 2011;90(3):151-9. https://doi.org/10.1016/j.antiviral.2011.03.179 PMid:21439328 PMCid:PMC3129598
- Papazian
L, Hraiech S, Lehingue S, Roch A, Chiche L, Wiramus S, Forel J-M.
Cytomegalovirus reactivation in ICU patients. Intensive Care Med.
2016;42:28-37. https://doi.org/10.1007/s00134-015-4066-9 PMid:26424680 PMCid:PMC7095171
- Li
Xi LX, Huang YongBo HY, Xu ZhiHeng XZ, Zhang Rong ZR, Liu XiaoQing LX,
Li YiMin LY, Mao Pu MP. Cytomegalovirus infection and outcome in
immunocompetent patients in the intensive care unit: a systematic
review and meta-analysis. 2018. https://doi.org/10.1186/s12879-018-3195-5 PMid:29954328 PMCid:PMC6027797
- Imlay
H, Limaye AP. Current understanding of cytomegalovirus reactivation in
critical illness. The J Infect Dis. 2020;221(Supplement_1):S94-S102. https://doi.org/10.1093/infdis/jiz638 PMid:32134490 PMCid:PMC7057786
- Hraiech
S, Bonnardel E, Guervilly C, Fabre C, Loundou A, Forel J-M, Adda M,
Parzy G, Cavaille G, Coiffard B. Herpes simplex virus and
Cytomegalovirus reactivation among severe ARDS patients under
veno-venous ECMO. Ann. Intensive Care. 2019;9:1-8. https://doi.org/10.1186/s13613-019-0616-6 PMid:31872319 PMCid:PMC6928167
- Papazian
L, Doddoli C, Chetaille B, Gernez Y, Thirion X, Roch A, Donati Y,
Bonnety M, Zandotti C, Thomas P. A contributive result of open-lung
biopsy improves survival in acute respiratory distress syndrome
patients. Crit Care Med. 2007;35(3):755-62. https://doi.org/10.1097/01.CCM.0000257325.88144.30 PMid:17255856
- Zhang
Z, Liu X, Sang L, Chen S, Wu Z, Zhang J, Sun Y, Huang Y, Xu Y, He W.
Cytomegalovirus reactivation in immunocompetent mechanical ventilation
patients: a prospective observational study. BMC Infect Dis.
2021;21:1-10. https://doi.org/10.1186/s12879-021-06698-0 PMid:34592936 PMCid:PMC8482357
- Cook
CH, Zhang Y, Sedmak DD, Martin LC, Jewell S, Ferguson RM. Pulmonary
cytomegalovirus reactivation causes pathology in immunocompetent mice.
Crit Care Med. 2006;34(3):842-9. https://doi.org/10.1097/01.CCM.0000201876.11059.05 PMid:16521279 PMCid:PMC1894751
- Limaye
AP, Stapleton RD, Peng L, Gunn SR, Kimball LE, Hyzy R, Exline MC, Files
DC, Morris PE, Frankel SK. Effect of ganciclovir on IL-6 levels among
cytomegalovirus-seropositive adults with critical illness: a randomized
clinical trial. JAMA. 2017;318(8):731-40. https://doi.org/10.1001/jama.2017.10569 PMid:28829877 PMCid:PMC5817487
- Papazian
L, Jaber S, Hraiech S, Baumstarck K, Cayot-Constantin S, Aissaoui N,
Jung B, Leone M, Souweine B, Schwebel C. Preemptive ganciclovir for
mechanically ventilated patients with cytomegalovirus reactivation.
Ann. intensive care. 2021;11:1-12. https://doi.org/10.1186/s13613-020-00793-2 PMid:33570708 PMCid:PMC7876264
- Cowley
NJ, Owen A, Shiels SC, Millar J, Woolley R, Ives N, Osman H, Moss P,
Bion JF. Safety and efficacy of antiviral therapy for prevention of
cytomegalovirus reactivation in immunocompetent critically ill
patients: a randomized clinical trial. JAMA Intern. Med.
2017;177(6):774-83. https://doi.org/10.1001/jamainternmed.2017.0895 PMid:28437539 PMCid:PMC5818821
- Jaber
S, Chanques G, Borry J, Souche B, Verdier R, Perrigault P-F, Eledjam
J-J. Cytomegalovirus infection in critically ill patients. Chest.
2005;127(1):233-41. https://doi.org/10.1378/chest.127.1.233 PMid:15653989
- Limaye
AP, Kirby KA, Rubenfeld GD, Leisenring WM, Bulger EM, Neff MJ, Gibran
NS, Huang M-L, Santo Hayes TK, Corey L. Cytomegalovirus reactivation in
critically ill immunocompetent patients. JAMA. 2008;300(4):413-22. https://doi.org/10.1001/jama.300.4.413 PMid:18647984 PMCid:PMC2774501
- Heininger
A, Haeberle H, Fischer I, Beck R, Riessen R, Rohde F, Meisner C, Jahn
G, Koenigsrainer A, Unertl K. Cytomegalovirus reactivation and
associated outcome of critically ill patients with severe sepsis.
Critical care. 2011;15:1-10. https://doi.org/10.1186/cc10069 PMid:21362193 PMCid:PMC3219329
- Zhang
Z, Zhang J, Dai S, Fan X, Liu Y, Sun J, Chen L, Song T, Li S, Zhang J.
Active cytomegalovirus infection in mechanically ventilated patients
with sepsis. BMC Infect Dis. 2024;24:1405. https://doi.org/10.1186/s12879-024-10304-4 PMid:39696007 PMCid:PMC11654325
- Kumar D, Humar A. Time to consider cytomegalovirus prevention in critically ill patients? JAMA. 2017;318(8):709-10. https://doi.org/10.1001/jama.2017.10132 PMid:28829852