Introduction
The spleen plays a multifaceted role in the management of TDT, serving as both an immune organ and the second-largest site for iron sequestration. Although current guidelines prioritize medical management, splenectomy is still indicated when annual transfusion needs increase significantly or when hypersplenism leads to clinical complications.[1,2,3] Following splenectomy, total body iron storage capacity is reduced, forcing excess iron to be redistributed to vital organs, including the heart, liver, and endocrine system.[1,4,5,6]While the association between splenectomy and myocardial iron overload or endocrinopathies is documented,[4,7,8,9] the long-term impact on the liver remains under-researched. Historical pathology-based studies noted a higher incidence of irregular cirrhosis in liver specimens from splenectomised patients compared to those with an intact spleen.[10] However, these early studies lacked non-invasive, quantitative tools to establish a clear statistical relationship. We utilized transient elastography (FibroScan®) and R2-MRI (FerriScan®) to investigate this association in a modern cohort of TDT patients.
Methods
This study utilized secondary data from a prospective cohort at the North Colombo Teaching Hospital, Sri Lanka. Ethical approval was obtained from the Ethics Review Committee (ERC) of the Faculty of Medicine, University of Kelaniya, Sri Lanka. The study cohort consisted of 45 heavily transfused TDT patients receiving dual intensive chelation: oral deferasirox (40 mg/kg/bw) and subcutaneous deferoxamine (45 mg/kg/bw) 5-7 days per week.Patients were followed for 2 to 2.5 years. At the end of the study, we assessed LSM using transient elastography (TE; FibroScan® 502 Touch) and liver iron concentration (LIC) using R2-MRI. Drug compliance was monitored using the “Brief Medication Questionnaire” (BMQ), a tool developed by B.L. Svarstad.[11] Statistical analysis included group comparisons based on splenectomy status and a multivariable linear regression to identify factors independently associated with LSM, adjusting for age, gender, BMI, diabetes, and chelation compliance. The distribution of continuous variables was expressed as mean (SD), and group comparisons were made using the Student t-test and Mann-Whitney U test for continuous variables and the chi-square test for categorical variables as appropriate. The data analysis was carried out in R (version 3.4.2), and p-values < 0.05 were considered statistically significant.
Results
Of the 45 patients studied, 33% (n=15) were splenectomised and required significantly less blood (164 ml/kg/year) than the unsplenectomised group (228.6 ml/kg/year; p < 0.001). Despite the reduced transfusion burden, splenectomised patients exhibited a dramatically higher mean LSM of 21.87 kPa compared to 6.94 kPa in those with an intact spleen (p < 0.001). Interestingly, LIC was higher in the splenectomy group (20.27 vs. 14.77 mg Fe/g dw), while this difference did not reach statistical significance (p = 0.117). Detailed laboratory results are provided in Table 1.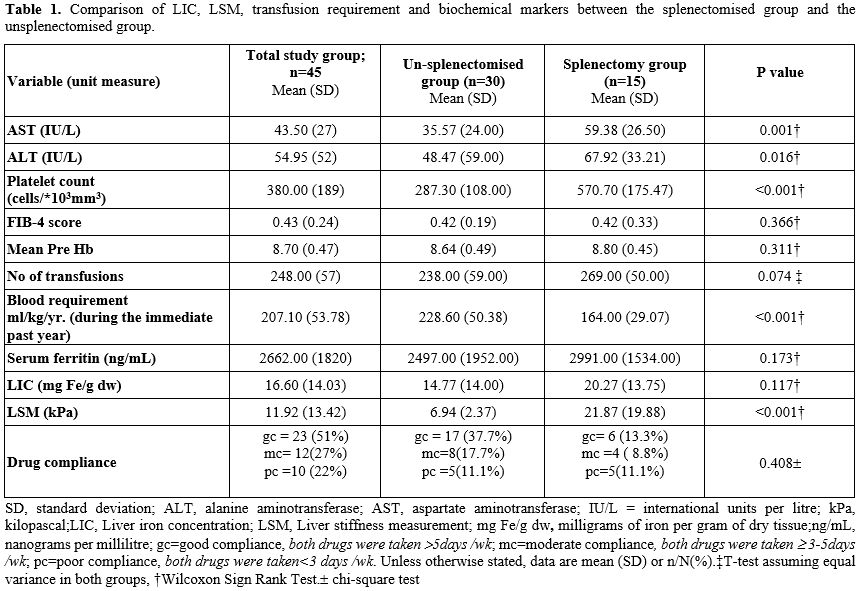 |
|
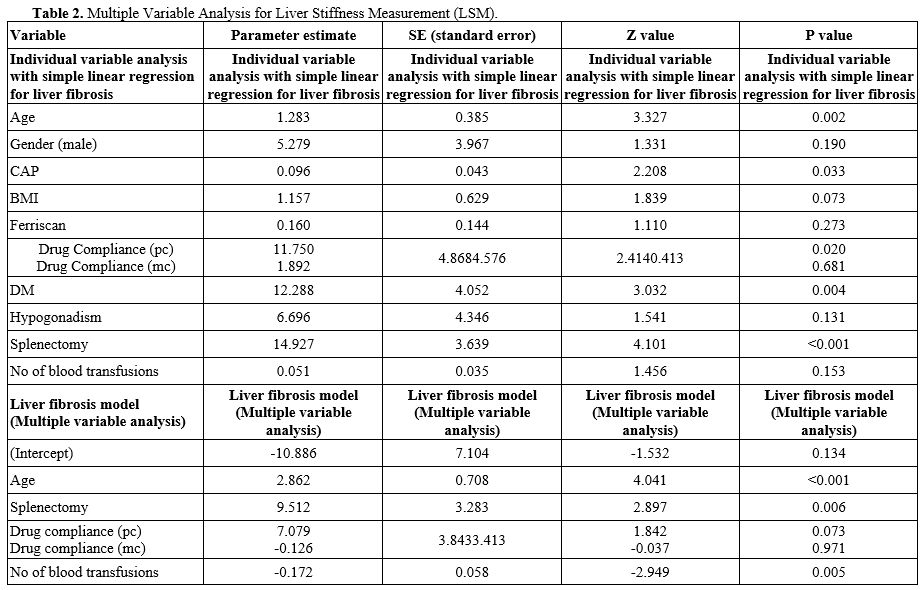
Multivariable regression analysis confirmed that splenectomy was a powerful independent predictor of liver stiffness, associated with a 9.51 kPa rise in LSM in splenectomised patients compared to the unsplenectomised group (p = 0.006) (Table 2).
 |
|
Discussion
The strong association between splenectomy and increased liver stiffness in our contemporary cohort identifies a significant clinical paradox: surgery intended to reduce iron loading through transfusions may actually accelerate liver injuryThe "LIC-LSM Paradox" — where stiffness is significantly higher despite similar steady-state iron concentrations — suggests that the liver in splenectomised patients is subject to a higher iron flux once the splenic buffer is removed. This higher rate of hepatocyte iron loading likely drives oxidative stress and fibrogenesis more aggressively than absolute concentration alone.[1]
Furthermore, the significant thrombocytosis observed in our cohort (570.7 vs. 287.3 cells/*103mm3) points toward vascular drivers of injury (Table 1). Chronic microthrombi in the portal circulation, a known complication post-splenectomy, may cause congestive stiffness, which elastography records as a high kPa value.[3] Importantly, our regression model adjusted for the total lifetime number of blood transfusions. This confirms that the observed fibrosis is not merely a consequence of "more severe disease" or higher iron intake,[12] but is independently linked to the absence of the spleen.
Conclusions
Splenectomy is an independent risk factor for increased liver stiffness in TDT patients. These results emphasize that the surgical reduction of transfusion burden is not a surrogate for organ protection. Careful long-term monitoring of hepatic outcomes is mandatory for this high-risk subgroup.Acknowledgements
This work was supported by a grant from the University Grant Commission, Colombo, Sri Lanka. (https://ugc.ac.lk/; Grant number: UGC/VC/DRIC/PG2017(I)/KLN/03).Additionally, this research was supported by a grant from the Research and Publication Division, University of Kelaniya, Sri Lanka (https://administration.kln.ac.lk/index.php/administration/research-and-publication-division).
All the staff members of the Adolescent and Adult Thalassaemia Care Centre (University Medical Unit), North Colombo Teaching Hospital, No. 10, Sirima Bandaranayake Mawatha, Kadawatha.
Hemas Hospital, No. 389, Negombo-Colombo Main Rd, Wattala, Sri Lanka, for providing the FerriScan facility.
Nawaloka Hospital PLC, Colombo 2, Sri Lanka, for providing the FibroScan facility.
Ethics approval and consent to participate
Ethical clearance was obtained from the Ethics Review Committee (ERC) of the Faculty of Medicine, University of Kelaniya, Sri Lanka. The study was performed in accordance with the declaration of Helsinki.Reference number/ID: P/89/02/2017
Authorship Contribution
PP was involved in designing the study, performing the research, analysing data, and drafting the paper. DE was involved in data analysis and interpretation and critically revising the paper. MN was involved in drafting the paper and critically revising the paper. AS contributed to carrying out the Transient Elastography and critically revising the paper. DK was involved in the patients' endocrinology assessment and critically revised the paper. AP conceptualised the study and was involved in designing the research protocol, interpreting it, drafting it, and critically revising it. All the authors read and approved the final version of the article.References
- Casale M, Cinque P, Ricchi P, Costantini S,
Spasiano A, Prossomariti L, Minelli S,Frega V,Filosa A. Effect of
splenectomy on iron balance in patients with β-thalassemia major: a
long-term follow-up. Eur J Haematol. 2013 Jul;91(1):69-73. https://doi.org/10.1111/ejh.12121 PMid:23581970
- Tahir
F, Ahmed J, Malik F. Post-splenectomy Sepsis: A Review of the
Literature. Cureus [Internet]. [cited 2024 Jun 28];12(2):e6898.
Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7059871/
- Guidelines
for the Management of Transfusion Dependent Thalassaemia (4th edition -
Version 2.0) [Internet]. TIF. [cited 2023 Jun 20]. Available from: https://thalassaemia.org.cy/publications/tif-publications/guidelines-for-the-management-of-transfusion-dependent-thalassaemia-4th-edition-2021-v2/
- Kolnagou
A, Michaelides Y, Kontoghiorghe CN, Kontoghiorghes GJ. The importance
of spleen, spleen iron, and splenectomy for determining total body iron
load, ferrikinetics, and iron toxicity in thalassemia major patients.
Toxicol Mech Methods. 2013 Jan;23(1):34-41. https://doi.org/10.3109/15376516.2012.735278 PMid:23039902
- Pootrakul
P, Vongsmasa V, La-ongpanich P, Wasi P. Serum ferritin levels in
thalassemias and the effect of splenectomy. Acta Haematol.
1981;66(4):244-50. https://doi.org/10.1159/000207129 PMid:6800190
- Gamberini
MR, De Sanctis V, Gilli G. Hypogonadism, diabetes mellitus,
hypothyroidism, hypoparathyroidism: incidence and prevalence related to
iron overload and chelation therapy in patients with thalassaemia major
followed from 1980 to 2007 in the Ferrara Centre. Pediatr Endocrinol
Rev PER. 2008 Oct;6 Suppl 1:158-69.
- Belhoul
KM, Bakir ML, Saned MS, Kadhim AMA, Musallam KM, Taher AT. Serum
ferritin levels and endocrinopathy in medically treated patients with β
thalassemia major. Ann Hematol. 2012 Jul;91(7):1107-14. https://doi.org/10.1007/s00277-012-1412-7 PMid:22281991
- Jaruratanasirikul
S, Chareonmuang R, Wongcharnchailert M, Laosombat V, Sangsupavanich P,
Leetanaporn K. Prevalence of impaired glucose metabolism in
beta-thalassemic children receiving hypertransfusions with a suboptimal
dosage of iron-chelating therapy. Eur J Pediatr. 2008 Aug;167(8):873-6.
https://doi.org/10.1007/s00431-007-0602-0 PMid:17899188
- Mandal
PK, Ghosh MK, Bhattacharyya M. Does Profile of Hemoglobin
Eβ-thalassemia Patients Change After Splenectomy? Experience of a
Tertiary Thalassemia Care Centre in Eastern India. Indian J Hematol
Blood Transfus Off J Indian Soc Hematol Blood Transfus. 2015
Dec;31(4):446-52. https://doi.org/10.1007/s12288-014-0498-6 PMid:26306069 PMCid:PMC4542765
- Okon
E, Levij IS, Rachmilewitz EA. Splenectomy, Iron Overload and Liver
Cirrhosis in β-Thalassemia Major. Acta Haematol [Internet]. 2009 Mar 3
[cited 2024 Jan 17];56(3):142-50. https://doi.org/10.1159/000207931 PMid:826069
- Svarstad
BL, Chewning BA, Sleath BL, Claesson C. The brief medication
questionnaire: A tool for screening patient adherence and barriers to
adherence. Patient Educ Couns [Internet]. 1999 Jun 1 [cited 2023 Sep
2];37(2):113-24. https://doi.org/10.1159/000207931 PMid:826069
- Khan
H., Panjwani V., Al Rahbi S., Eltigani A., Qureshi R.N., Unissa K.,
Sehar N., Mittal A., Pathare A.V. Correlation of transient elastography
with liver iron concentration and serum ferritin levels in patients
with transfusion-dependent thalassemia major from Oman.Mediterr J
Hematol Infect Dis 2023, 15(1): e2023048 https://doi.org/10.4084/MJHID.2023.048 PMid:37705529 PMCid:PMC10497312