Syphilis, caused by Treponema pallidum, is a multisystem infection that may involve the nervous system at any stage. Neurosyphilis, ocular syphilis, and otosyphilis can present with meningitis, stroke, optic neuropathy, or sensorineural hearing loss. Diagnosis relies on clinical context supported by cerebrospinal fluid (CSF) testing; however, CSF-VDRL is insensitive, and seronegative neurosyphilis remains a recognized diagnostic challenge.[2]
We report a unique seven-year longitudinal observation of a patient in whom secondary syphilis and neurosyphilis coincided with the emergence of hypoplastic MDS. The case illustrates how chronic infection may act as a “second hit,” revealing an underlying clonal hematopoietic disorder, and underscores key diagnostic and management lessons for internists and hematologists.
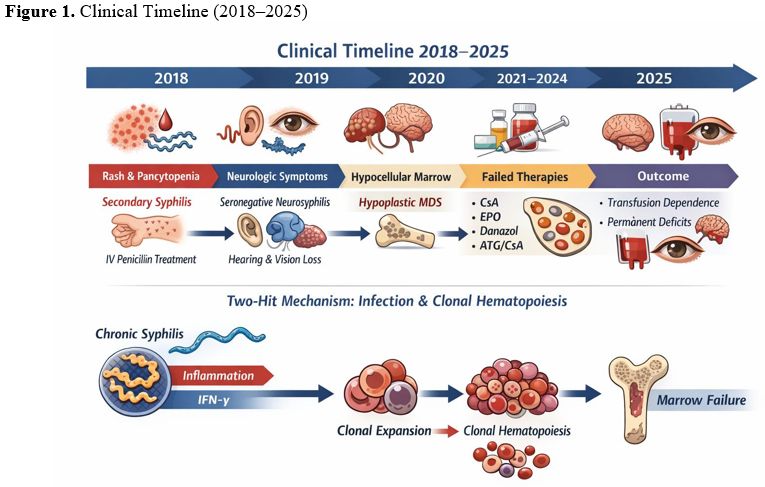
A 54-year-old man presented in early 2018 with bruising, fever, arthralgia, and a purpuric rash. Skin biopsy showed leukocytoclastic vasculitis. Complete blood counts revealed pancytopenia (WBC 1.0×10⁹/L, hemoglobin 6.0 g/dL, platelets 60×10⁹/L). Bone marrow evaluation demonstrated trilineage dysplasia without excess blasts and normal cellularity. Syphilis serology was strongly positive, consistent with secondary syphilis (VDRL titer 1:640; treponemal test positive). The patient had no relevant exposure to toxins and no prior cytotoxic therapy. He received intravenous penicillin G followed by ceftriaxone; fever and rash resolved, yet cytopenias persisted, requiring regular red cell transfusions. Serial VDRL titers declined over time and became nonreactive by April 2022, supporting microbiologic cure; nevertheless, transfusion dependence continued and iron overload developed (ferritin >2500 ng/mL), requiring chelation.
In 2019, the patient developed progressive neurologic symptoms (hearing loss, tinnitus, blurred vision). Examination demonstrated bilateral sensorineural hearing loss and optic pallor. CSF analysis was unremarkable, and both CSF-VDRL and CSF treponemal tests were negative. Brain MRI showed nonspecific white matter lesions and mild atrophy. Despite negative CSF serology, neurosyphilis was considered based on compatible clinical and radiologic findings. Supportive management, including corticosteroids and rehabilitation, was administered. During the same year, the patient developed warm autoimmune hemolytic anemia (DAT positive, haptoglobin undetectable), which responded to rituximab.
From 2020 onward, pancytopenia worsened. A repeat marrow in 2020 showed marked hypocellularity (~20%) with persistent dysplasia and no blast excess, compatible with hypoplastic MDS; cytogenetics remained normal. Multiple therapies were attempted, including prolonged cyclosporine, darbepoetin alfa, danazol, and, finally, horse antithymocyte globulin (ATG) plus cyclosporine, without achieving a durable hematologic response. The patient remained transfusion-dependent with persistent severe marrow failure. Allogeneic hematopoietic stem cell transplantation (HSCT) was not performed because a suitable donor could not be identified. By 2025, after seven years of follow-up, the patient had not transformed to acute leukemia but continued to have profound pancytopenia and irreversible neurologic sequelae (permanent sensorineural hearing loss and optic atrophy).
 |
|
Mechanistic interpretation (“two-hit” model). This clinical course supports a model in which chronic infection served as an inflammatory selection pressure that unmasked a latent predisposition to clonal hematopoiesis rather than acting as a reversible cause of marrow failure. Emerging experimental data demonstrate that chronic infection and cytokine signaling can expand mutant hematopoietic stem cell clones; in murine models, chronic infection drives the expansion of DNMT3A loss-of-function clones via interferon-γ signaling, and recombinant interferon-γ can reproduce clonal expansion. This framework provides a plausible mechanistic bridge between chronic infection and subsequent overt marrow failure.[3]
In our patient, eradication of T. pallidum did not restore hematopoiesis, supporting the interpretation that infection was a trigger that accelerated or revealed clonal disease rather than a direct cause of persistent marrow failure. However, the relationship between myelodysplastic syndrome and neurosyphilis remains hypothetical, and in any case, this MDS is markedly different from the forms secondary to chemotherapy and radiotherapy.[4]
Diagnostic lesson: Neurosyphilis can be seronegative in CSF. Standard guidance emphasizes integrating neurologic and ocular symptoms with CSF testing; the CSF-VDRL is highly specific but has limited sensitivity. When the CSF-VDRL is negative but suspicion persists, CSF treponemal testing is typically recommended; negative CSF treponemal tests generally make neurosyphilis unlikely.[5]
Nonetheless, this case illustrates a real-world scenario where the clinical phenotype strongly supported neurosyphilis despite negative CSF assays, reminding clinicians that late presentations and testing limitations may necessitate judgment-driven decisions to prevent irreversible deficits.
Clinical message for internists and hematologists. Cytopenias in patients with treatable infections are often assumed to be reactive and reversible. This case highlights that persistent cytopenias after microbiologic cure should prompt evaluation for clonal hematopoiesis/MDS, especially when marrow dysplasia is present. Hypoplastic MDS shares immune-mediated features with aplastic anemia and may be associated with autoimmune manifestations; response rates to immunosuppressive strategies remain limited in many patients.[6]
Advanced therapies for transfusion-dependent lower-risk MDS have evolved rapidly. Luspatercept improves red blood cell maturation and increases transfusion independence; imetelstat demonstrated superiority over placebo in a phase 3 trial of transfusion-dependent MDS and received regulatory approval in 2024.[7,8] These agents, however, require adequate marrow reserve and are less effective in profound hypocellular disease. Curative HSCT should be considered early, and donor search should begin promptly in appropriate candidates, because delays may narrow curative options.[9]
References
- García-Manero, G. (2023). Myelodysplastic
syndromes: 2023 update on diagnosis, risk stratification, and
management. American Journal of Hematology, 98(8), 1307-1325. https://doi.org/10.1002/ajh.26984 PMid:37288607 PMCid:PMC12002404
- Centers
for Disease Control and Prevention. (2021; updated 2024). Sexually
Transmitted Infections Treatment Guidelines: Syphilis. https://www.cdc.gov/std/treatment-guidelines/syphilis.htm
- Hormaechea-Agulla,
D., Matatall, K. A., Le, D. T., et al. (2021). Chronic infection drives
DNMT3A-loss-of-function clonal hematopoiesis via IFN-γ signaling. Cell
Stem Cell, 28(8), 1428-1442.e6. https://doi.org/10.1016/j.stem.2021.03.002 PMid:33743191 PMCid:PMC8349829
- Leone
G., Fabiani E., Voso M.T.De novo and therapy-related myelodysplastic
syndromes: analogies and differences.Mediterr J Hematol Infect Dis
2022, 14(1): e2022030. https://doi.org/10.4084/MJHID.2022.030 PMid:35615324 PMCid:PMC9083943
- Centers
for Disease Control and Prevention. (2023). Notes from the Field:
Neurosyphilis, Ocular Syphilis, and Otosyphilis - Chicago,
January-October 2023. MMWR Morbidity and Mortality Weekly Report,
72(8), 215-216. https://www.cdc.gov/mmwr/volumes/72/wr/mm7208a5.htm
- Rafiq, K., et al. (2024). The immunobiology of myelodysplastic neoplasms: A mini-review. Frontiers in Immunology, 15, 1419807. https://doi.org/10.3389/fimmu.2024.1419807 PMid:39355256 PMCid:PMC11443505
- Fenaux,
P., Platzbecker, U., Mufti, G. J., et al. (2020). Luspatercept in
patients with lower-risk myelodysplastic syndromes. New England Journal
of Medicine, 382(2), 140-151. https://doi.org/10.1056/NEJMoa1908892 PMid:31914241
- Platzbecker,
U., Santini, V., Fenaux, P., et al. (2024). Imetelstat for lower-risk
myelodysplastic syndromes refractory to erythropoiesis-stimulating
agents (IMerge): A phase 3 trial. The Lancet, 403(10423), 249-260. https://doi.org/10.1016/S0140-6736(23)01724-5 PMid:38048786
- National Cancer Institute. (2024, September 19). Myelodysplastic Syndromes Treatment (PDQ®) - Health Professional Version. https://www.cancer.gov/types/myeloproliferative/hp/myelodysplastic-treatment-pdq