Even in publicly funded healthcare systems, such as those in Western Europe, including Italy, where cancer care is delivered for free, patients may experience considerable direct non-medical costs and indirect costs.[3]
Importantly, financial concerns may arise early in the disease trajectory. Patients often begin to anticipate financial difficulties as soon as they receive a diagnosis, before substantial costs are incurred. In the broader context of mental health, future-oriented stressors activate neural and psychological systems that partially overlap with those involved in traumatic stress and produce higher levels of anxiety and depressive symptoms.[4-5] However, while a wide literature has reported how financial burden is associated with adverse outcomes in both mental and physical health,[1,6-8] little is known about whether expectations of financial burden at diagnosis are associated with trauma-related psychological symptoms in patients with hematologic malignancies.
Post-traumatic stress symptoms (PTSS), including the intrusive re-experiencing of the traumatic event, the physiological hyperarousal, the negative thoughts or feelings, and the avoidance of trauma-related stimuli,[9] are frequently reported following a cancer diagnosis.[10] The present study aimed to examine whether the expectation of a deteriorating economic situation at diagnosis is associated with PTSS in patients newly diagnosed with leukemia or lymphoma.
Patients and Methods
Fifty-nine patients with leukemia or lymphoma (27 females; age range 23-77 years) were consecutively recruited at the time of diagnosis. Diagnoses included acute myeloid leukemia (n = 25), non-Hodgkin lymphoma (n = 16), acute lymphoblastic leukemia (n = 9), Hodgkin lymphoma (n = 5), and acute promyelocytic leukemia (n = 4). Post hoc power analyses were conducted to estimate the statistical power achieved in the main analysis (i.e., repeated-measures ANOVA). With α = 0.05 and N = 59, the study showed adequate power (≥ 0.80) to detect medium effect sizes for both the between-subjects factor (f > 0.30) and the within-subjects and the interaction effects (f > 0.16).The study was approved by the Local Ethics Committee (343/2024-DB id 14068), and all subjects gave their written informed consent.
Participants completed self-report questionnaires assessing socio-demographic variables, expectations of financial burden, perceived information about assistance rights, and PTSS related to the cancer diagnosis.
Expectations about financial burden were assessed using a single item adapted from the financial difficulties question of the EORTC QLQ-C30 [e.g., 2]. The wording was modified to capture anticipated difficulties (“Do you expect financial difficulties caused by your physical condition or medical treatment?”). Responses were dichotomized to indicate the presence or the absence of expected financial burden.
The received information was assessed using two ad hoc developed items. Participants were asked to rate the extent to which they felt they had received useful information regarding state and work-related assistance rights using a 5-point Likert-type scale from 0 (“Not at all”) to 4 (“Very much”). An additional response option, “Does not apply to me,” was provided for participants who considered the question irrelevant to their situation. These kinds of responses were treated as missing values.
PTSS was assessed through the Impact of Event Scale-Revised (IES-R),[11] referring specifically to the cancer diagnosis. This is a 22-item self-report measure that assesses subjective distress caused by traumatic events. It is made of three subscales representing the major symptom clusters of post-traumatic stress, namely intrusion, avoidance, and hyperarousal. Participants had to rate each item on a 5-point Likert-type scale ranging from 0 ("not at all") to 4 ("extremely"). Following the scoring guidelines, the three subscales' score was calculated by averaging the corresponding items within each (score ranged from 0 to 4).
Descriptive statistics and preliminary analyses (t-tests and χ² tests) were conducted to explore possible risk factors for expectations about financial burden. Our primary research objective (i.e., the possible association between expectations of financial hardship and PTSS) was assessed using an independent repeated-measures ANOVA with the PTSS subscales (intrusion, avoidance, hyperarousal) as the within-subjects factor and expectation of financial hardship as the between-subjects factor.
Results
The descriptive statistics of all continuous variables are shown in Table 1.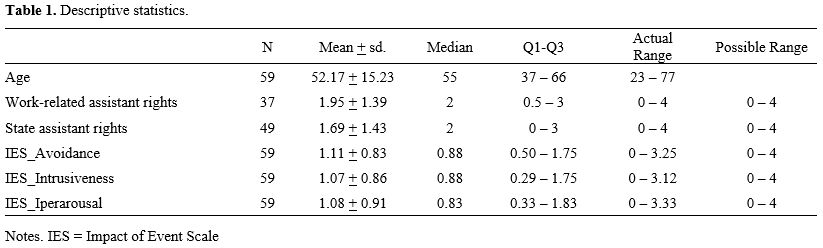 |
|
Regarding information about work-related assistance rights, the question did not apply to about 37% of participants. Among the 63% of participants who responded to the question, we observed a broad range of responses: 54% reported receiving little to no information (i.e., “not at all/little/very little”), while 46% indicated they had received a significant amount of information (“much/very much”).
Regarding information about state assistance rights, the question did not apply to about 17% of participants. Among the 83% of participants who responded to the question, we observed a broad range of responses: 63.3% reported receiving little to no information (i.e., “not at all/little/very little”), while 36.7% indicated they had received a significant amount of information (“much/very much”).
Regarding PTSS, we observed that around 55.9% of participants had a normal level of PTSS, whereas 16.9% of patients experienced mild to moderate PTSS, and 27.2% of them experienced severe PTSS.
Regarding expectations of financial burden, 42,4% of patients expected financial difficulties due to their physical condition or medical treatment. Preliminary analyses revealed a significant age difference between individuals who expected financial difficulties due to the disease and those who did not, t(57) = 2.74, p = .008. Additionally, a significant difference was observed with regard to the presence of minor children, χ2 = 18.31, p < 0.001. In detail, the expected financial burden is more frequent in younger people and in patients with minor children. Received information about assistance rights was not linked to these expectations. Indeed, with regards to received information about state and work-related assistance rights, we did not find significant differences between people who expected financial difficulties due to the disease and people who did not, t(47) = -1.42, p = 0.161, t(35) = 0.24, p = 0.812, respectively.
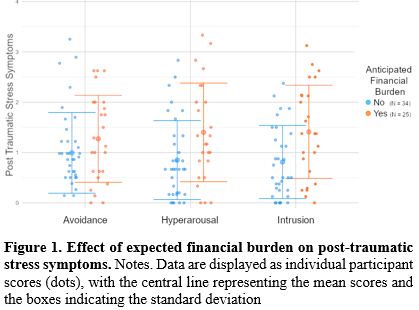
Repeated measure ANOVA revealed a significant main effect of the expected financial burden on PTSS, F(57,1) = 6.31, p = 0.015, η2 = 0.10, indicating higher overall PTSS levels among patients expecting financial difficulties. However, we did not find a significant effect of PTSS type, F(56,2) = 0.03, p = 0.969, η2 < 0.01, and of its interaction with FT, F(56,2) = 1.12, p = 0.333, η2 = 0.04, suggesting similar symptom levels across intrusion, avoidance, and hyperarousal (see Figure 1).
 |
|
Discussion
In this exploratory study, nearly half of patients newly diagnosed with hematologic malignancies reported at least mild post-traumatic stress symptoms, and more than 40% anticipated financial difficulties related to their disease or treatment. These findings confirm the substantial psychological burden associated with a hematologic cancer diagnosis[12-13] and suggest that concerns about future financial strain emerge very early in the disease trajectory, even before substantial costs are incurred. Importantly, such expectations may serve as early indicators of the actual financial difficulties that arise in later stages of the disease trajectory.[1]Expectations of financial burden were more frequent among younger patients and those with minor children. Younger individuals may be particularly vulnerable because they are more likely to face employment instability related to prolonged hospitalization and treatment-related side effects, potentially leading to job loss and reduced income.[14-15] In addition, younger patients often have ongoing financial commitments and fewer opportunities to accumulate financial reserves, which may increase their susceptibility to cancer-related financial demands.[16] Accordingly, both material and psychological financial toxicity have been reported to be higher in younger compared with older adults.[17] Similarly, patients with dependent children may experience heightened concerns related to household expenses and caregiving responsibilities, which can amplify worries about income disruption and additional treatment-related costs. Changes in family roles and caregiving arrangements may further contribute to these concerns.[18] These findings identify specific patient subgroups who may be at increased risk of anticipatory financial stress at diagnosis. Main results revealed that patients who anticipated financial difficulties reported significantly higher levels of PTSS at diagnosis across symptom domains (avoidance, intrusiveness, and hyperarousal). This association supports models of future-oriented stress[5] and suggests that concerns about future financial hardship may represent an additional psychological burden at the time of diagnosis. Even before tangible financial strain occurs, worries about future economic stability may be linked to heightened distress. However, given the cross-sectional design of the study, conclusions about directionality cannot be drawn, and these findings should be interpreted as associations rather than causal relationships. Additionally, no domain-specific effects were observed across the PTSS symptom clusters. These null findings should be interpreted cautiously, as the modest sample size may have limited statistical power, increasing the risk of Type II errors and reducing the ability to detect small within-subject or interaction effects. Finally, some relevant clinical and socioeconomic variables (e.g., disease severity, treatment line, transplant eligibility, and employment status), which may represent additional sources of confounding, were not systematically collected. Importantly, factors such as younger age and the presence of dependent children, which we found to be linked to PTSS, may independently contribute to psychological distress at diagnosis and therefore partly account for the observed association between anticipated financial burden and PTSS. As a result, the relationship identified in this study may reflect shared vulnerability factors rather than financial expectations per se. Longitudinal studies with larger samples and more comprehensive repeated assessments, using multivariable approaches, are needed to disentangle these effects and clarify temporal and causal pathways.
Conclusions
In conclusion, these findings suggest that not only the experience of financial hardship, but also its anticipation, are associated with psychological well-being and PTSS at the time of diagnosis in patients with hematologic malignancies. Recognizing anticipatory financial concerns may therefore help clinicians identify patients at higher psychological risk early in the disease trajectory. Integrating routine screening and clear referral pathways to social services, financial counseling, and psycho-oncology support could facilitate timely, targeted interventions. Embedding these steps within multidisciplinary hematology care may represent a practical strategy to mitigate the emotional impact of financial uncertainty and improve patient well-being and overall outcomes. This is consistent with the recent ESMO Expert Consensus Statements, which emphasize the need to assess financial concerns in patients with hematologic malignancies as early as diagnosis and before treatment initiation.[5] Early screening for financial distress, combined with timely supportive interventions and appropriate counseling, may represent an important component of routine clinical care and contribute to improving patient experience and outcomes. Increasing awareness and training among healthcare professionals may further facilitate the timely identification of financial distress and the provision of appropriate support.[19-20] Incorporating such measures into multidisciplinary cancer care can play a vital role in mitigating financial toxicity and improving the overall experience and outcomes for patients with hematologic malignancies.Author Contributions: data availability statement
Data supporting this study are available under direct request to the corresponding author.Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.Ethics approval statement
This study was approved by the Local Ethics Committee (343/2024 - DB id 14068).Author Contributions
Fabio Guolo: conceptualization, funding acquisition, investigation, writing - review and editing. Paola Del Sette: formal analysis, writing - original draft. Francesca Riccardi: writing - review and editing. Paola Minetto: investigation, writing - review and editing. Andrea Todiere: investigation, writing - review and editing. Filippo Ballerini: investigation, writing - review and editing. Carola Riva: investigation, writing - review and editing. Michele Cea: investigation, writing - review and editing. Roberto Massimo Lemoli: investigation, writing - review and editing. Elena Sarcletti: conceptualization, writing - original draft.All authors gave their final approval.
References
- Ouchveridze E, Banerjee R, Desai A, et al. Financial toxicity in
hematological malignancies: a systematic review. Blood Cancer J.
2022;12(4):74. https://doi.org/10.1038/s41408-022-00671-z PMid:35459862
PMCid:PMC9033803
- Sparano F, Giesinger JM, Gaidano G, et al.
Financial Toxicity and Health-Related Quality of Life Profile of
Patients With Hematologic Malignancies Treated in a Universal Health
Care System. JCO Oncol Pract. 2024;20(3):438-447.
https://doi.org/10.1200/OP.23.00434 PMid:38207239
- Carrera PM,
Curigliano G, Santini D, et al. ESMO expert consensus statements on the
screening and management of financial toxicity in patients with cancer.
ESMO Open. 2024;9(5):102992.
https://doi.org/10.1016/j.esmoop.2024.102992 PMid:38626634
PMCid:PMC11033153
- Farina, M. P., Zhang, Z., & Donnelly, R.
(2023). Anticipatory stress, state policy contexts, and mental health
during the COVID-19 pandemic. SSM Popul Health. 2023;23:101415.
https://doi.org/10.1016/j.ssmph.2023.101415 PMid:37200581
PMCid:PMC10129343
- Grupe DW, Nitschke JB. Uncertainty and
anticipation in anxiety: an integrated neurobiological and
psychological perspective. Nat Rev Neurosci. 2013;14(7):488-501.
https://doi.org/10.1038/nrn3524 PMid:23783199 PMCid:PMC4276319
- Pail
O, Knight TG. Financial toxicity in patients with leukemia undergoing
hematopoietic stem cell transplantation: A systematic review. Best
Pract Res Clin Haematol. 2023;36(2):101469.
https://doi.org/10.1016/j.beha.2023.101469 PMid:37353293
- Li T, Cui
P, Shao M, Guo S, Zhang M, Chen C. Financial toxicity and its
influencing factors in patients with non-Hodgkin lymphoma: A
cross-sectional study. Eur J Oncol Nurs. 2024;70:102619.
https://doi.org/10.1016/j.ejon.2024.102619 PMid:38797113
- Sears-Smith
M, Knight TG. Financial Toxicity in Patients with Hematologic
Malignancies: a Review and Need for Interventions. Curr Hematol Malig
Rep. 2023;18:158-166. https://doi.org/10.1007/s11899-023-00707-6
PMid:37490228
- American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders, Fifth Edition, Text Revision
(DSM-5-TR®). American Psychiatric Association Publishing; 2022.
https://doi.org/10.1176/appi.books.9780890425787
- Springer F,
Kuba K, Ernst J, et al. Symptoms of posttraumatic stress disorder and
adjustment disorder in hematological cancer patients with different
treatment regimes. Acta Oncol. 2023;62(9):1110-1117.
https://doi.org/10.1080/0284186X.2023.2239477 PMid:37517064
- Weiss,
D.S. The Impact of Event Scale: Revised. In: Wilson, J.P., Tang, C.Sk.
Cross-Cultural Assessment of Psychological Trauma and PTSD.
International and Cultural Psychology Series. Springer, Boston, MA;
2007;219-238. https://doi.org/10.1007/978-0-387-70990-1_10
- Springer
F, Esser P, Friedrich M, et al. Compliance with medical regimen among
hematological cancer patients and its association with symptoms of
posttraumatic stress disorder and adjustment disorder. Front Psychol.
2023;14:1278485. https://doi.org/10.3389/fpsyg.2023.1278485
PMid:38022979 PMCid:PMC10655000
- Springer F, Kuba K, Ernst J, et
al. Symptoms of posttraumatic stress disorder and adjustment disorder
in hematological cancer patients with different treatment regimes. Acta
Oncol. 2023;62(9):1110-1117.
https://doi.org/10.1080/0284186X.2023.2239477 PMid:37517064
- Parsons
SK, Kumar AJ. Adolescent and young adult cancer care: Financial
hardship and continued uncertainty. Pediatr Blood Cancer.
2019;66(4):e27587. https://doi.org/10.1002/pbc.27587 PMid:30556354
- Thom
B, Benedict C, Friedman DN, Kelvin JF. The intersection of financial
toxicity and family building in young adult cancer survivors. Cancer.
2018;124(16):3284-3289. https://doi.org/10.1002/cncr.31588
PMid:29924381 PMCid:PMC6108923
- McNulty J, Khera N. Financial
Hardship--an Unwanted Consequence of Cancer Treatment. Curr Hematol
Malig Rep. 2015;10(3):205-212.
https://doi.org/10.1007/s11899-015-0266-1 PMid:26112652
- Corrigan
KL, Fu S, Chen YS, Kaiser K, Roth M, Peterson SK, Shih YT, Jagsi R,
Giordano SH, Volk RJ, Yabroff KR, Banegas MP, Acquati C, Conti RM, Ma
HY, Ku K, You YN, Smith GL. Financial toxicity impact on younger versus
older adults with cancer in the setting of care delivery. Cancer.
2022;128(13):2455-2462. https://doi.org/10.1002/cncr.34220
PMid:35417565 PMCid:PMC9177670
- Zheng Z, Han X, Zhao J, Fan Q,
Yabroff KR. Parental Cancer History and Its Association With Minor
Children's Unmet Food, Housing, and Transportation Economic Needs. JAMA
Netw Open. 2023;6(6):e2319359.
https://doi.org/10.1001/jamanetworkopen.2023.19359 PMid:37347484
PMCid:PMC10288335
- Carrera PM, Kantarjian HM, Blinder VS. The
financial burden and distress of patients with cancer: Understanding
and stepping-up action on the financial toxicity of cancer treatment.
CA Cancer J Clin. 2018;68(2):153-165.
https://doi.org/10.3322/caac.21443 PMid:29338071 PMCid:PMC6652174
- Smith GL, Banegas MP, Acquati C, et al. Navigating financial toxicity in patients with cancer: A multidisciplinary management approach. CA Cancer J Clin. 2022;72(5):437-453. https://doi.org/10.3322/caac.21730 PMid:35584404