Immunoparesis refers to the suppression of one or more immunoglobulins (i.e., polyclonal immunoglobulins) in patients with MM, such as a reduction in IgA and/or IgM in IgG-type MM patients,[5,6] resulting in an immunodeficient state.[7] The incidence of immunoparesis is extremely high in newly diagnosed MM patients, reaching 80% to 95%.[8,9] Existing evidence suggests that immunoparesis has a negative impact on the survival prognosis of MM patients, with the degree of immunosuppression and its recovery serving as independent prognostic factors for the disease.[10,11] Studies have confirmed that immunoparesis is an independent risk factor for early infections.[12] However, to date, no research has examined the relationship between varying states of immunoparesis and early infections in patients with MM.
Therefore, we conducted an in-depth study of the impact of different immunoparesis states on early infections (within six months of diagnosis) in newly diagnosed multiple myeloma (NDMM) patients, using both qualitative classification (the number of polyclonal immunoglobulin types suppressed) and quantitative grading (the degree of polyclonal immunoglobulin reduction). This further explores the factors that contribute to infection susceptibility, aiming to assist clinicians in better preventing and managing infections, thereby reducing infection incidence and mortality rates in patients.
Study Design
Study Population Selection. This retrospective study included 411 patients with diagnosed MM who sought treatment at our hospital between 2016 and 2024. Diagnosis of MM was confirmed in all patients according to the criteria set by the International Myeloma Working Group (IMWG). Exclusion criteria included: (1) relapsed or refractory MM; (2) incomplete medical records or missing baseline laboratory data; (3) a follow-up duration of less than 6 months without reaching the study endpoint. Ultimately, 213 patients were included in the analysis. The detailed patient selection and exclusion process is illustrated in the flowchart in Figure S1 of the Supplementary Material. All procedures involving human participants were conducted in accordance with the Declaration of Helsinki.Data Collection. We collected various clinical data at the time of diagnosis and during the subsequent 6 months in NDMM patients. These data included baseline information such as age, gender, ISS stage, genetic high-risk status, laboratory indicators, imaging results, immunotyping, and first-line chemotherapy regimens. Infections were diagnosed based on clinical symptoms, radiologic findings, and microbiological cultures, supplemented by PCT, G, and GM tests. Events were graded per CTCAE v5.0. To ensure data robustness, the analysis focused on the first episode of grade ≥ 3 infections, defined as severe events requiring intravenous therapy or hospitalization. Prophylactic antimicrobial use was excluded. Early infection was defined as any grade ≥ 3 event occurring within 6 months of diagnosis.
Immunoparesis was defined as the reduction of one or more uninvolved or polyclonal immunoglobulins below the institutional lower limit of normal, specifically IgG < 7.0 g/L, IgA < 0.7 g/L, or IgM < 0.4 g/L. Uninvolved immunoglobulins were assigned based on the MM subtype. For patients with intact immunoglobulin myeloma, immunoglobulins of the non-involved classes (e.g., IgA and IgM in a patient with IgG-type MM) were assessed for suppression. For patients with light-chain or non-secretory myeloma, all three immunoglobulin classes (IgG, IgA, and IgM) were considered uninvolved and evaluated for immunoparesis. These components were identified via immunofixation electrophoresis. In this study, immunoparesis was assessed using both qualitative and quantitative methods. Qualitative classification was based on the number of immunoglobulin types suppressed: 1. No immunoparesis (all polyclonal immunoglobulins are above the lower limit of normal); 2. Partial immunoparesis (at least one but not all polyclonal immunoglobulins are suppressed); 3. Full immunoparesis (all polyclonal immunoglobulins are below the lower limit of normal). According to the criteria described by Chakraborty et al., quantitative classification involved calculating the extent of suppression for each polyclonal immunoglobulin, with the following categories: 1. No immunoparesis; 2. Shallow immunoparesis (decrease < 50%); 3. Deep immunoparesis (decrease ≥ 50%).[12]
Statistical Analysis. This study aimed to assess the relationship between the qualitative and quantitative states of immunoparesis and the risk of early infection. All statistical analyses were performed using SPSS software (version 26.0, IBM) and R software (version 4.3.3). Descriptive statistics were used to summarize the patients' baseline characteristics. Categorical variables were expressed as frequencies and percentages, while continuous variables were presented as means and standard deviations or medians and interquartile ranges, depending on the results of normality tests. Kaplan-Meier survival curves were used to evaluate the impact of the qualitative and quantitative states of immunoparesis on early infection risk, and Log-rank tests were used to assess the significance of intergroup differences. To further analyze the independent effects of different immunoparesis states on infection risk, we employed Cox proportional hazards regression models, adjusting for confounding factors such as age, ISS stage, hemoglobin, creatinine, β2-microglobulin, LDH levels, and treatment regimens. The proportional hazards assumption for the Cox models was rigorously verified using Schoenfeld residuals (Global P = 0.062). For continuous variables, the assumption of linearity was confirmed through Martingale residual analysis. All multivariate analyses were based on complete-case data from 213 patients, as no covariates were missing. Mann-Whitney U tests were used to compare immunoglobulin (IgM, IgA, IgG) levels between the bacterial and non-bacterial infection groups. The relationship between treatment regimens and infection types was analyzed using chi-square tests. All statistical tests were two-tailed, with P < 0.05 considered statistically significant.
Results
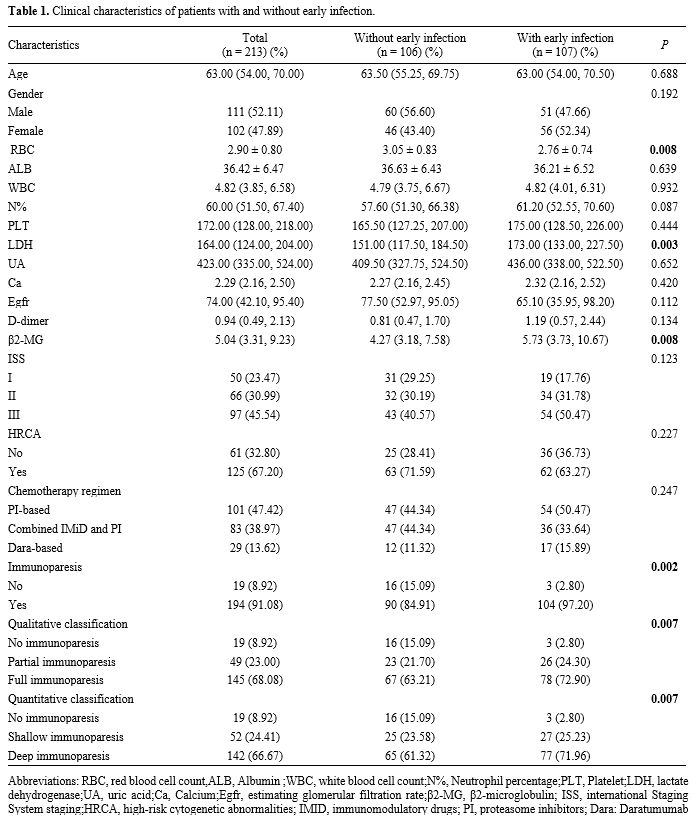
Characteristics of Early Infections. This study included 213 patients, with the patient selection process depicted in Supplementary Figure S1. The median age was 63 years. According to the ISS staging system, 23.47% of patients were classified as Stage I, 30.99% as Stage II, and 45.54% as Stage III. Among all patients, 50.5% (107/213) developed a ≥ 3 grade infection within 6 months of diagnosis, 34.7% (74/213) within 3 months, and 25.8% (55/213) within 1 month. Among the 107 infected patients, 54 (50.47%) received an IMiD-based regimen, 36 (33.64%) received an IMiD combined with PI regimen, and 17 (15.89%) received a Dara-based regimen. No significant correlation was found between the treatment regimen and early infection occurrence within 6 months of diagnosis.The most common infection sites were the respiratory and pulmonary systems, accounting for 51.4% (55/107). This was followed by gastrointestinal infections (14.9%, 16/107), urinary tract infections (5.6%, 6/107), bloodstream infections (6.5%, 7/107), skin and soft tissue infections (8.4%, 9/107), and infections with unknown sites (13.1%, 14/107). From a microbiological perspective, bacterial infections were the most common, accounting for 21.5% (23/107), followed by viral infections 9.3% (10/107) and fungal infections 6.5% (7/107). Infections due to unknown pathogens had the highest proportion, at 62.6% (67/107). The time distribution of early infections, distribution of infection sites, and pathogen distribution are shown in Figure S2. Compared with non-infected patients, infected patients had significantly lower red blood cell counts (P = 0.008) and significantly higher levels of LDH and β2-microglobulin (P < 0.05). Specific laboratory differences are shown in Table 1.
 |
|
Characteristics of Immunoparesis. Among the 213 NDMM patients, 91.1% (194/213) had immunoparesis. The proportion of early infections in immunoparesis patients was significantly higher than in those without immunoparesis. Regarding the M protein types in immunoparesis patients, 48.5% (94/194) had IgG type, 18.6% (36/194) had IgA type, 17.5% (34/194) had λ type, 11.9% (23/194) had κ type, 2.1% (4/194) had non-secretory type, and 1.6% (3/194) had IgM type.
In the qualitative analysis, 23.0% (49/213) had partial immunoparesis, and 68.1% (145/213) had full immunoparesis. With an increasing number of suppressed immunoglobulin types, red blood cell counts and albumin levels significantly decreased (P < 0.05), as shown in Table 2. In the quantitative analysis, 24.4% (52/213) of patients had an Ig suppression level < 50%, while 66.6% (142/213) had an Ig suppression level ≥ 50%. As the degree of suppression increased, significant declines in red blood cells, white blood cells, platelets, and calcium levels were observed, while no significant differences were observed in genetic high-risk status or ISS stage (Table 3).
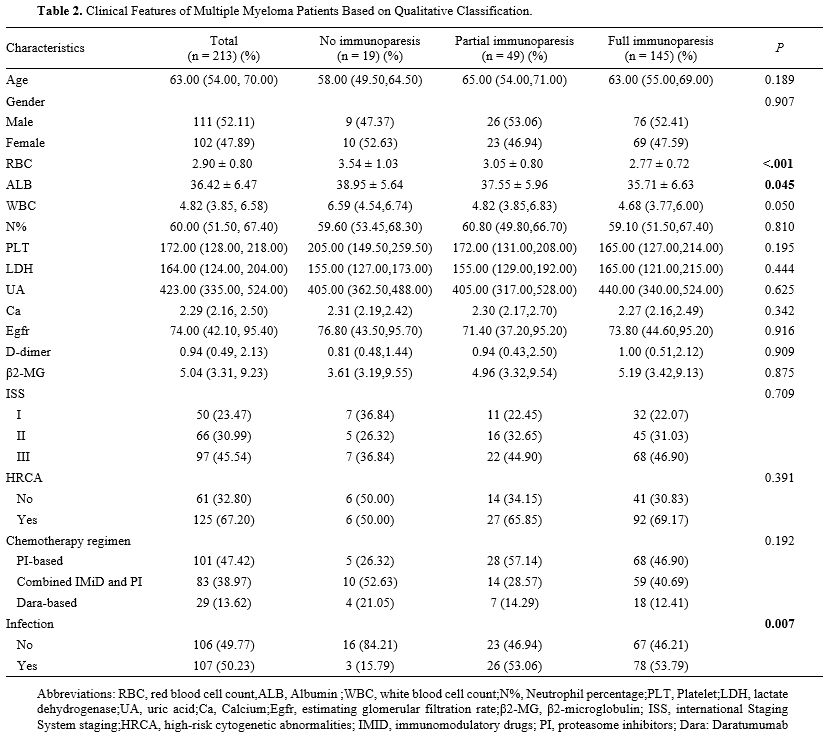 |
Table 2.
Clinical Features of Multiple Myeloma Patients Based on Qualitative Classification. |
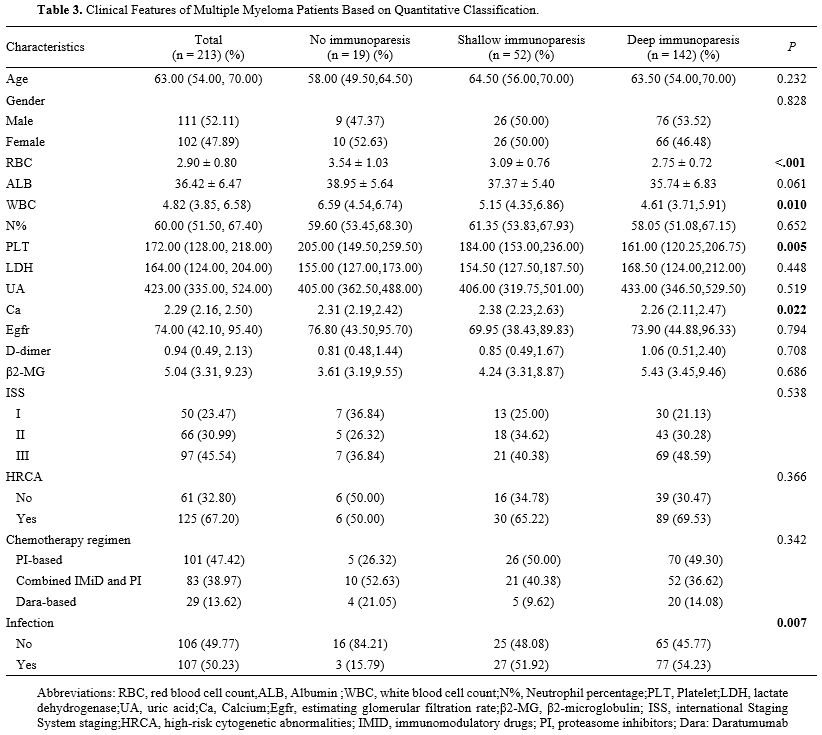 |
Table 3. Clinical Features of Multiple Myeloma Patients Based on Quantitative Classification. |
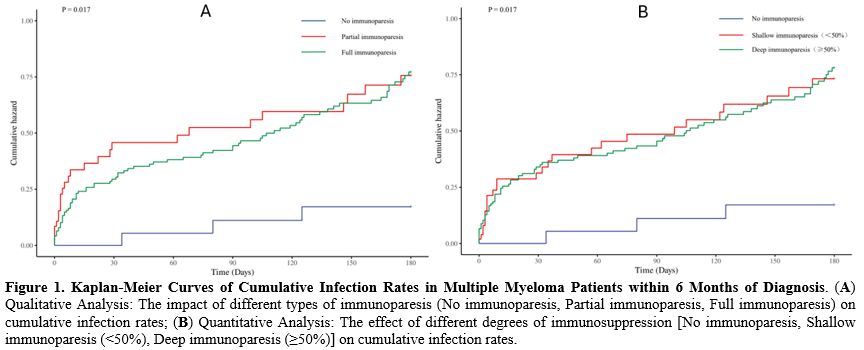
Relationship Between Different States of Immunoparesis and Early Infection. Within six months of diagnosis, the infection rates for the no immunoparesis, partial immunoparesis, and full immunoparesis groups were 3/19 (15.8%), 26/49 (53.1%), and 78/145 (53.8%), respectively. Kaplan-Meier survival curves showed a significant difference in infection rates among the three groups (P = 0.017). Compared to the no immunoparesis group, the infection rates were significantly higher in the partial and full immunoparesis groups. During the first three months after diagnosis, the infection rate in the partial immunoparesis group was significantly higher than in the full immunoparesis group; however, after three months, the infection rate in the full immunoparesis group gradually increased and intersected with that of the partial immunoparesis group. In the quantitative assessment, the infection rates for the no immunoparesis, suppression degree < 50%, and suppression degree ≥ 50% groups were 3/19 (15.8%), 27/52 (51.9%), and 77/142 (54.2%), respectively. Kaplan-Meier survival curves showed a significant difference in infection rates among the three groups (P = 0.017). The infection rates in both shallow and deep immunoparesis groups were significantly higher than in the no immunoparesis group. Although the infection rate slightly increased with greater degrees of immunosuppression, the infection curves of the two groups continued to intersect. The Kaplan-Meier curves for cumulative infection rates within 6 months post-diagnosis, for both qualitative and quantitative assessments, are shown in Figure 1.
 |
|
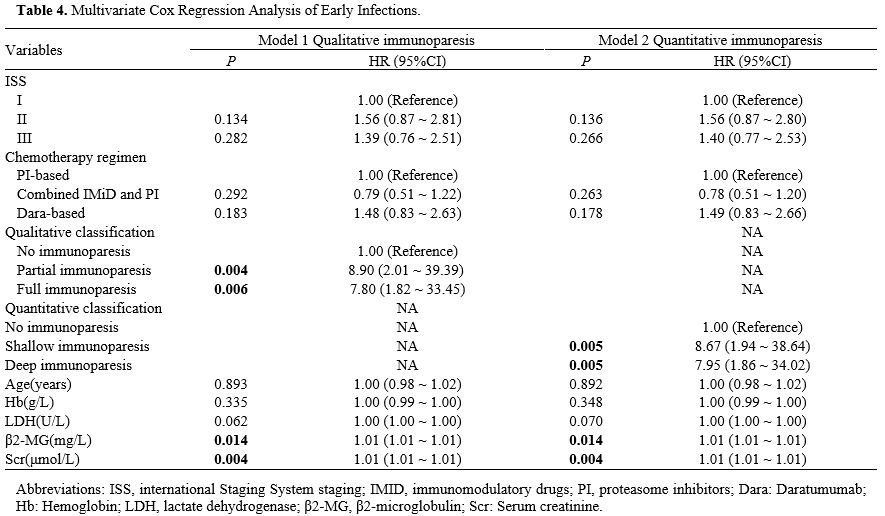
To assess the independent effects of qualitative and quantitative immunoparesis on infection timing, we constructed multivariate Cox proportional hazard models, adjusting for clinical factors such as age, ISS stage, hemoglobin, creatinine, β2-microglobulin, LDH, and treatment regimen, based on relevant studies of infection risk in MM. The results showed that, in the qualitative analysis model (Table 4), compared to the no immunoparesis group, the infection risk in the partial immunoparesis group was significantly higher (HR = 8.9, P = 0.004), and in the full immunoparesis group, it was 7.8 times higher (HR = 7.8, P = 0.006). In the quantitative analysis model, compared to the no immune suppression group, the early infection risk in the < 50% suppression group increased by 8.67 times (HR = 8.67, P = 0.005), and in the ≥ 50% suppression group, it increased by 7.95 times (HR = 7.95, P = 0.005). These findings confirm that immunoparesis significantly increases the risk of early infection. However, within this cohort, we did not observe a statistically significant risk gradient associated with either the breadth (partial vs. full) or the depth (< 50% vs. ≥ 50%) of immunoglobulin suppression.
 |
|
In the multivariate analysis, creatinine and β2-microglobulin levels were independent predictors of early infection (P < 0.05), whereas age, ISS stage, hemoglobin, and LDH levels did not show significant effects (P > 0.05). Additionally, the impact of different treatment regimens on infection risk was analyzed, revealing no significant differences (P > 0.05).
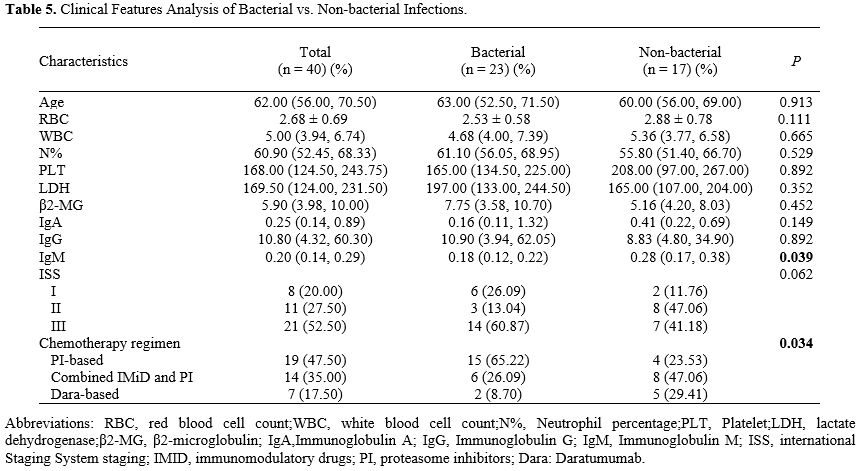
Exploratory Analysis of Pathogen Distribution and Clinical Correlates. Among the 107 infected patients, specific pathogens were identified in 40 cases (37.4%), including 23 bacterial and 17 non-bacterial infections. Given this limited microbiological confirmation rate, the following analyses are considered exploratory and hypothesis-generating. We compared clinical characteristics between these two subgroups. Preliminary observations indicated that IgM levels were lower in the bacterial infection group than in the non-bacterial group (P = 0.039), whereas no such trend was observed for IgA or IgG (Table 5).
Additionally, treatment regimens appeared to be associated with certain infection types in this subgroup. However, no statistically significant differences were observed in the number or degree of immunoparesis between the groups.
 |
|
Discussion
Early infections remain one of the leading causes of early mortality in MM patients.[4,13] Our study indicates that immunoparesis significantly increases the risk of early infections in MM patients. However, our analysis did not identify a statistically significant progressive increase in infection risk corresponding to the number of suppressed immunoglobulin types or the severity of immunosuppression.In our study, 50.5% of patients developed infections of grade ≥ 3 within six months of diagnosis, with the most common infection site being the lungs, and the most common pathogen being bacteria. These findings align with studies by Blimark, Sørrig, and others.[4,14]
The association between immunoparesis and increased early infection risk observed in our cohort aligns with established evidence that immune suppression is a significant predictor of poor prognosis in MM.[8,11,15] Mechanistically, immunoparesis reflects impaired humoral immunity through suppressed polyclonal immunoglobulin synthesis, increasing susceptibility to pathogens, particularly during the initiation of immunosuppressive therapy.[6,16,17] While previous studies have suggested that more severe immunoparesis correlates with poorer survival outcomes,[12,18] our study did not observe a significant risk gradient with respect to the breadth or depth of suppression. Specifically, infection rates were comparable between partial and full immunoparesis, with no marked increase in risk observed when comparing immunoglobulin reductions of <50% versus ≥50%.
These observations may be influenced by several factors. The high prevalence of immunoparesis in NDMM naturally led to a small reference group and a skewed distribution across subgroups, which, as reflected in the wider confidence intervals, may have limited the statistical power to detect subtle risk gradients. Additionally, this finding is consistent with the perspective that, while the depth of immunoparesis relates to overall prognosis, its impact on infection risk may not follow a strictly linear progression.[1,8] It is possible that the primary infection risk arises from the initial disruption of humoral homeostasis. However, as this retrospective cohort lacked longitudinal immunophenotyping, cellular immune assays, or cytokine profiling, the biological basis for the absence of a risk gradient cannot be definitively characterized. Future prospective studies incorporating comprehensive immunological assessments are required to further elucidate the relationship between the severity of immunoparesis and infection risk.
In the subgroup of patients with microbiologically identified pathogens (n=40), several preliminary trends were observed. Within this restricted sample, lower IgM levels appeared preferentially associated with bacterial infections compared to IgA or IgG suppression, a finding that conceptually aligns with the established role of IgM in humoral immune surveillance.[13,15] Additionally, exploratory data suggested potential variations in pathogen distribution across treatment regimens. Specifically, bacterial infections predominated in patients receiving proteasome inhibitors, while viral and fungal pathogens were more frequently recorded in those on Dara-based regimens.[19] However, since 62.6% of infection events remained microbiologically undocumented, these observations derived from a limited absolute sample size must be strictly regarded as exploratory and hypothesis-generating rather than definitive clinical patterns. The low microbiological confirmation rate in this study reflects the inherent diagnostic complexities of NDMM in a real-world setting. This phenomenon stems primarily from the clinical imperative to initiate empirical antimicrobial therapy before specimen collection to mitigate early mortality risks, alongside the logistical challenges of obtaining specimens in a retrospective setting. Consequently, these findings regarding IgM and treatment regimens represent only preliminary tendencies within our specific cohort. Their biological significance and therapeutic implications warrant further investigation in larger prospective studies utilizing standardized microbiological screening protocols.
Our analysis also revealed that β2-microglobulin and creatinine levels are independent predictors of early infections, consistent with the findings of Charles et al.[20,21] Elevated β2-microglobulin levels indicate higher tumor burden, while elevated creatinine levels suggest renal dysfunction, both of which are risk factors for infections.
Several limitations of this study warrant consideration. While the analysis focused on established prognostic markers, certain granular clinical factors, including cumulative steroid exposure, performance status, and specific prophylaxis strategies, were not incorporated into the multivariate models. Although proxy indicators such as ISS stage and continuous creatinine levels were used to reflect disease burden, the independent prognostic value of immunoparesis remains suggestive. Additionally, the high prevalence of immunoparesis (91.1%) in this cohort naturally limited the size of the reference group to nineteen patients. This numerical imbalance led to wider confidence intervals in the Cox models, warranting cautious interpretation of the precise hazard ratio magnitudes. Notably, our data did not demonstrate a statistically significant risk gradient across varying breadths or depths of suppression. This observation may suggest that any degree of immunoglobulin reduction constitutes a critical threshold for elevated infection risk in this population. However, we also recognize that the study might be underpowered to discern more subtle differences. Therefore, these findings should be interpreted as a lack of demonstrated difference within this specific cohort rather than proof of biological equivalence. Future prospective studies with larger, more balanced cohorts are necessary to further refine these risk estimates. Finally, as detailed in the previous section, the pathogen-specific analysis is constrained by the high rate of undocumented infections and the limited number of confirmed samples. These exploratory findings are hypothesis-generating and should not be interpreted as definitive proof of risk equivalence between suppression states. Future prospective studies with larger, more balanced cohorts are required to further refine these risk estimations.
Conclusion
In conclusion, immunoparesis is a significant and independent predictor of early infection risk in patients with NDMM. While our data do not demonstrate a risk gradient based on the specific breadth or depth of immunoglobulin suppression, the high incidence of severe infection across all suppression states is clinically noteworthy. These findings underscore that immunoparesis, regardless of severity, is a critical indicator for identifying high-risk patients. Clinicians should prioritize assessing immunoparesis at diagnosis to support vigilant monitoring and the implementation of timely infection prevention strategies.Author contributions
Hongfeng Wang: Writing – review & editing, Writing – original draft, Visualization, Formal analysis, Data curation, Conceptualization; Jianbin Chen: Writing – review & editing, Visualization, Validation, Supervision, Resources, Project administration, Methodology, Funding acquisition, Formal analysis, Data curation. All authors approved the final version.Data Availability Statement
Data may be available from the corresponding author upon reasonable request.Acknowledgments
We are grateful to The First Affiliated Hospital of Chongqing Medical University.References
- Heaney JLJ, Campbell JP, Iqbal G, Cairns D, Richter
A, Child JA, Gregory W, Jackson G, Kaiser M, Owen R, Davies F, Morgan
G, Dunn J, Drayson MT. Characterisation of immunoparesis in newly
diagnosed myeloma and its impact on progression-free and overall
survival in both old and recent myeloma trials. Leukemia.
2018;32:1727-38. https://doi.org/10.1038/s41375-018-0163-4 PMid:29925902 PMCid:PMC6087716
- Kyle
RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A, Fonseca R,
Rajkumar SV, Offord JR, Larson DR, Plevak ME, Therneau TM, Greipp PR.
Review of 1027 Patients With Newly Diagnosed Multiple Myeloma. Mayo
Clin Proc. 2003;78:21-33. https://doi.org/10.4065/78.1.21 PMid:12528874
- Malard
F, Neri P, Bahlis NJ, Terpos E, Moukalled N, Hungria VTM, Manier S,
Mohty M. Multiple myeloma. Nat Rev Dis Primers. 2024;10:45. https://doi.org/10.1038/s41572-024-00529-7 PMid:38937492
- Blimark
C, Holmberg E, Mellqvist UH, Landgren O, Björkholm M, Hultcrantz M,
Kjellander C, Turesson I, Kristinsson SY. Multiple myeloma and
infections: a population-based study on 9253 multiple myeloma patients.
Haematologica. 2015;100:107-13. https://doi.org/10.3324/haematol.2014.107714 PMid:25344526 PMCid:PMC4281323
- Wangel A. Multiple myeloma and polyclonal hypogammaglobulinaemia. Acta Med Scand. 1987;221:421-5. https://doi.org/10.1111/j.0954-6820.1987.tb01275.x PMid:3300176
- Wang H, Chen J. Immunoparesis in multiple myeloma: a current overview. Front Oncol. 2025;15:1628144. https://doi.org/10.3389/fonc.2025.1628144 PMid:41064084 PMCid:PMC12501984
- Pruzanski
W, Gidon MS, Roy A. Suppression of polyclonal immunoglobulins in
multiple myeloma: relationship to the staging and other manifestations
at diagnosis. Clin Immunol Immunopathol. 1980;17:280-6. https://doi.org/10.1016/0090-1229(80)90097-5 PMid:7408241
- Kastritis
E, Zagouri F, Symeonidis A, Roussou M, Sioni A, Pouli A, Delimpasi S,
Katodritou E, Michalis E, Michael M, Hatzimichael E, Vassou A, Repousis
P, Christophoridou A, Kartasis Z, Stefanoudaki E, Megalakaki C,
Giannouli S, Kyrtsonis MC, Konstantopoulos K, Spyroupoulou-Vlachou M,
Terpos E, Dimopoulos MA, Greek Myeloma Study Group. Preserved levels of
uninvolved immunoglobulins are independently associated with favorable
outcome in patients with symptomatic multiple myeloma. Leukemia.
2014;28:2075-9. https://doi.org/10.1038/leu.2014.110 PMid:24637336
- Chahin
M, Branham Z, Fox A, Leurinda C, Keruakous AR. Clinical considerations
for immunoparesis in multiple myeloma. Cancers. 2022;14:2278. https://doi.org/10.3390/cancers14092278 PMid:35565407 PMCid:PMC9104750
- Harutyunyan
NM, Vardanyan S, Ghermezi M, Gottlieb J, Berenson A, Andreu-Vieyra C,
Berenson JR. Levels of uninvolved immunoglobulins predict clinical
status and progression-free survival for multiple myeloma patients. Br
J Haematol. 2016;174:81-7. https://doi.org/10.1111/bjh.14026 PMid:27017948
- Zhang
M, Cheng Q, Zhao F, Xu A, Li Q, Hu Y, Sun C. Development of a nomogram
prognostic model for early grade ≥ 3 infection in newly diagnosed
multiple myeloma based on immunoparesis. Int Immunopharmacol.
2024;126:111277. https://doi.org/10.1016/j.intimp.2023.111277 PMid:38061120
- Chakraborty
R, Rybicki L, Nakashima MO, Dean RM, Faiman BM, Samaras CJ, Rosko N,
Dysert H, Valent J, Anwer F. Characterisation and prognostic impact of
immunoparesis in relapsed multiple myeloma. Br J Haematol.
2020;189:1074-82. https://doi.org/10.1111/bjh.16488 PMid:32108328 PMCid:PMC9292652
- Holmström
MO, Gimsing P, Abildgaard N, Andersen NF, Helleberg C, Clausen NAT,
Klausen TW, Frederiksen M, Kristensen DL, Larsen H, Pedersen PT,
Andersen KT, Pedersen RS, Jensen BA, Gregersen H, Vangsted AJ. Causes
of early death in multiple myeloma patients who are ineligible for
high-dose therapy with hematopoietic stem cell support: a study based
on the nationwide danish myeloma database. Am J Hematol.
2015;90:E73-74. https://doi.org/10.1002/ajh.23932 PMid:25561348
- Sørrig
R, Klausen TW, Salomo M, Vangsted A, Gimsing P. Risk factors for
infections in newly diagnosed multiple myeloma patients: a danish
retrospective nationwide cohort study. Eur J Haematol. 2019;102:182-90.
https://doi.org/10.1111/ejh.13190 PMid:30485563
- Sørrig
R, Klausen TW, Salomo M, Vangsted AJ, Frølund UC, Andersen KT,
Klostergaard A, Helleberg C, Pedersen RS, Pedersen PT, Helm-Petersen S,
Teodorescu EM, Preiss B, Abildgaard N, Gimsing P. Immunoparesis in
newly diagnosed multiple myeloma patients: effects on overall survival
and progression free survival in the danish population. PLoS One.
2017;12:e0188988. https://doi.org/10.1371/journal.pone.0188988 PMid:29216227 PMCid:PMC5720701
- Pratt G, Goodyear O, Moss P. Immunodeficiency and immunotherapy in multiple myeloma. Br J Haematol. 2007;138:563-79. https://doi.org/10.1111/j.1365-2141.2007.06705.x PMid:17686051
- Rennert
P, Schneider P, Cachero TG, Thompson J, Trabach L, Hertig S, Holler N,
Qian F, Mullen C, Strauch K, Browning JL, Ambrose C, Tschopp J. A
soluble form of B cell maturation antigen, a receptor for the tumor
necrosis factor family member april, inhibits tumor cell growth. J Exp
Med. 2000;192:1677-84. https://doi.org/10.1084/jem.192.11.1677 PMid:11104810 PMCid:PMC2193103
- Geng
C, Yang G, Wang H, Wu Y, Leng Y, Zhou H, Zhang Z, Jian Y, Chen W. Deep
and partial immunoparesis is a poor prognostic factor for newly
diagnosed multiple myeloma patients. Leuk Lymphoma. 2021;62:883-90. https://doi.org/10.1080/10428194.2020.1855345 PMid:33275060
- Mateos
MV, Dimopoulos MA, Cavo M, Suzuki K, Jakubowiak A, Knop S, Doyen C,
Lucio P, Nagy Z, Kaplan P, Pour L, Cook M, Grosicki S, Crepaldi A,
Liberati AM, Campbell P, Shelekhova T, Yoon SS, Iosava G, Fujisaki T,
Garg M, Chiu C, Wang J, Carson R, Crist W, Deraedt W, Nguyen H, Qi M,
San-Miguel J, ALCYONE Trial Investigators. Daratumumab plus bortezomib,
melphalan, and prednisone for untreated myeloma. N Engl J Med.
2018;378:518-28. https://doi.org/10.1056/NEJMoa1714678 PMid:29231133
- Shang
Y, Wang W, Liang Y, Kaweme NM, Wang Q, Liu M, Chen X, Xia Z, Zhou F.
Development of a risk assessment model for early grade ≥ 3 infection
during the first 3 months in patients newly diagnosed with multiple
myeloma based on a multicenter, real-world analysis in China. Front
Oncol. 2022;12:772015. https://doi.org/10.3389/fonc.2022.772015 PMid:35372017 PMCid:PMC8967980
- Dumontet C, Hulin C, Dimopoulos MA, Belch A, Dispenzieri A, Ludwig H, Rodon P, Van Droogenbroeck J, Qiu L, Cavo M, Van De Velde A, Lahuerta JJ, Allangba O, Lee JH, Boyle E, Perrot A, Moreau P, Manier S, Attal M, Roussel M, Mohty M, Mary JY, Civet A, Costa B, Tinel A, Gaston-Mathé Y, Facon T. A predictive model for risk of early grade ≥ 3 infection in patients with multiple myeloma not eligible for transplant: analysis of the FIRST trial. Leukemia. 2018;32:1404-13. https://doi.org/10.1038/s41375-018-0133-x PMid:29784907 PMCid:PMC5990520
Supplementary Material
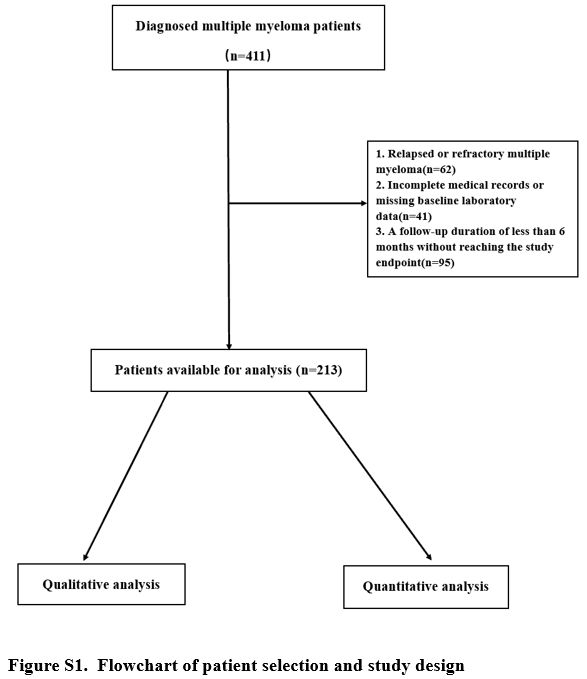 |
Figure S1. Flowchart of patient selection and study design. |
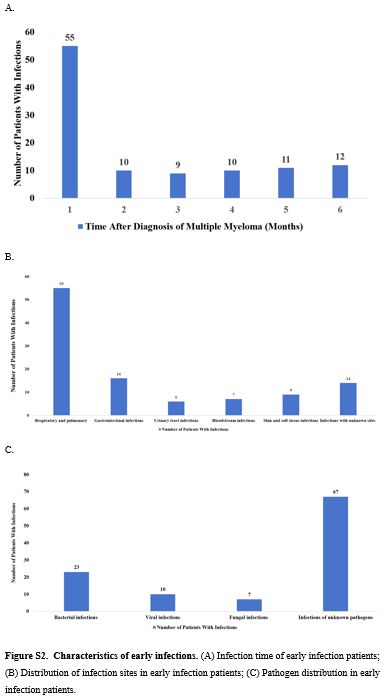 |
Figure S2. Characteristics of early infections. (A)
Infection time of early infection patients; (B) Distribution of
infection sites in early infection patients; (C) Pathogen distribution
in early infection patients. |