Case Presentation
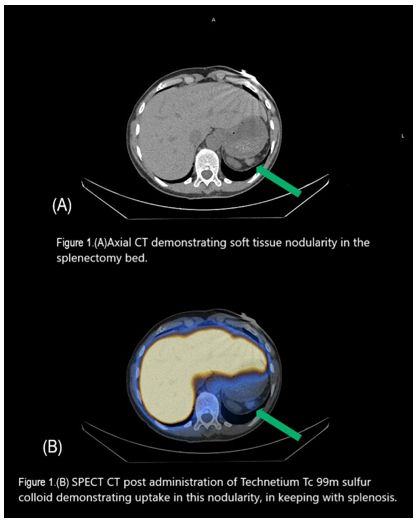
A 65-year-old female patient was referred to the Haematology Department at Mater Private Hospital, Dublin, by her general practitioner (GP) for investigation of asymptomatic macrocytic anaemia and thrombocytosis. She had undergone splenectomy at the age of 17 following abdominal trauma sustained in a road traffic accident. She denied weight loss, night sweats, abdominal pain or other constitutional symptoms. Her regular medications included amitriptyline 10 mg, phenoxymethylpenicillin 333 mg and denosumab 60 mg once daily. On clinical examination, there was no lymphadenopathy or organomegaly. Initial laboratory investigations showed haemoglobin (Hb) of 11.6 g/dL with mean corpuscular volume (MCV) of 102 fL, white blood cell count of 6.9 ×10⁹/L, neutrophils 4.2 ×10⁹/L and platelet count of 423 ×10⁹/L. Vitamin B12, folate and ferritin levels were normal. Viral serology and myeloma screening were negative. There was no evidence suggestive of myelodysplastic syndrome or a myeloproliferative neoplasm. CT scan of the thorax, abdomen and pelvis demonstrated multiple well-circumscribed soft tissue nodules within the anterior peritoneum, anterior diaphragmatic fat and left pelvic sidewall measuring up to 1.4 cm.The radiological appearance raised suspicion of peritoneal carcinomatosis, representing a significant diagnostic concern. However, the remote history of splenectomy prompted consideration of splenosis as an alternative explanation for the imaging findings.
For further evaluation, nuclear medicine imaging with Tc-99m sulfur colloid SPECT was performed, which confirmed the diagnosis of splenosis.
 |
|
Discussion
There are two main hypotheses explaining the pathogenesis of ectopic splenic tissue throughout the abdomen: direct implantation of splenic fragments (splenic seeding) following trauma or splenectomy, and haematogenous dissemination.[1-4] Clinically and radiologically, splenosis represents an important diagnostic pitfall because it may closely mimic malignant peritoneal disease. Patients with omental splenosis may present with nonspecific abdominal symptoms and may be referred to gastroenterology or surgical services. As a result, the condition has been misdiagnosed as irritable bowel syndrome, inflammatory bowel disease, bowel obstruction, pseudomyxoma peritonei, peritoneal lymphomatosis, tuberculosis, peritoneal mesothelioma, diffuse peritoneal leiomyomatosis and even primary gastrointestinal malignancy.[2-6] The average interval between splenectomy and diagnosis of splenosis is approximately 10 years, although reported cases range from a few months to 40 years. Thrombocytosis after splenectomy is a common finding, and platelet counts may become markedly elevated (>900 ×10⁹/L) in the early postoperative period. Over time, platelet values generally decrease but may remain mildly elevated (>450 ×10⁹/L). Platelet counts in patients with splenosis have occasionally been reported; however, in most cases they remain mildly elevated, suggesting that splenosis alone does not fully restore the hemocatheretic function of the spleen.[7] An open question remains whether patients with previous splenectomy and residual splenosis should also receive antimicrobial prophylaxis and scheduled vaccinations against encapsulated microorganisms, including Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis. Previous reports suggest that splenosis alone is insufficient to provide adequate protection against these pathogens. Furthermore, clinicians should be aware that splenosis may also be associated with complications such as bleeding, including gastrointestinal hemorrhage6.In the present case, the 48-year interval between splenectomy and diagnosis highlights the possibility of extremely delayed presentation.Most importantly, this case illustrates how splenosis can mimic peritoneal carcinomatosis on CT imaging. Recognition of this entity and careful review of past surgical history are therefore essential to avoid unnecessary invasive investigations or even unnecessary oncological treatment. When splenosis is suspected, nuclear medicine studies such as Tc-99m sulfur colloid or heat-damaged red blood cell scintigraphy are reliable, noninvasive diagnostic tools that can help clinicians diagnose splenosis.
References
- Pei B, Hu Z, Pan F. Thoracic splenosis
initially misdiagnosed as lung neoplasms: An unusual case and
literature review. Medicine (Baltimore). 2026 Jan 2;105(1):e47056. https://doi.org/10.1097/MD.0000000000047056 PMid:41496102 PMCid:PMC12778126
- Hussain
M, Malkova K, Romanov A, Rawas F, Botiralieva GK, Pak N, Chernov YN,
Lyapichev KA. Splenosis involved by in situ follicular B-cell neoplasm.
Virchows Arch. 2025 Nov 24. https://doi.org/10.1007/s00428-025-04322-z
- Peng
Y, Liang R, Zhang C, Sun L, Zhao J. Abdominopelvic Splenosis Resembling
an Ovarian Malignancy: A Case Report. Int J Womens Health. 2025 Oct
30;17:4011-4018. https://doi.org/10.2147/IJWH.S556829 PMid:41190252 PMCid:PMC12581867
- Hussain
M, Malkova K, Romanov A, Rawas F, Botiralieva GK, Pak N, Chernov YN,
Lyapichev KA. Splenosis involved by in situ follicular B-cell neoplasm.
Virchows Arch. 2025 Nov 24. https://doi.org/10.1007/s00428-025-04322-z
- Hanifa
H, Alhussein H, Mahmandar L, Kadi S, Najjar M, Alhaj A. Unveiling three
accessory spleens in one patient: a rare case report and literature
review. Int J Emerg Med. 2024 Nov 12;17(1):175. https://doi.org/10.1186/s12245-024-00758-3 PMid:39533206 PMCid:PMC11555858
- Rodríguez
PF, Martínez Fernández R, Aldama ER. Abdominal splenosis as a rare and
serious cause of upper gastrointestinal bleeding. Med Clin (Barc). 2026
Feb;166(2):107271. https://doi.org/10.1016/j.medcle.2026.107271
- Khan PN, Nair RJ, Olivares J, et al.Postsplenectomy reactive thrombocytosis. Proc (Bayl Univ Med Cent). 2009;22(1):9-12. https://doi.org/10.1080/08998280.2009.11928458 PMid:19169391 PMCid:PMC2626351