This improvement is not uniform globally. The present manuscript primarily addresses patient populations in high-income settings where longitudinal transfusion programs, iron monitoring, disease-modifying therapies, and multidisciplinary specialty access are feasible. In many low- and middle-income settings, early mortality, limited access to safe transfusion and chelation, infectious complications, and constrained diagnostic infrastructure remain dominant determinants of outcomes, and the clinical priorities and feasible monitoring strategies may differ considerably.[3]
Adults with hemoglobinopathies experience a qualitatively different disease burden, not dominated by acute crises alone, but by cumulative organ damage, polypharmacy, and the convergence of disease-specific complications with age-associated chronic disease. This phenotype, premature multimorbidity combined with a lifelong genetic disease burden, makes hemoglobinopathies a potential model for studying health-span compression in chronic illness.[4]
Gerontology is the scientific study of the processes and problems of aging from biological, clinical, psychological, and social perspectives. In this manuscript, gerontological constructs refer to established conceptual models in gerontology used to explain vulnerability in later life, such as frailty, inflammaging, and loss of physiologic reserve, and a gerontological model refers to a clinical framework that prioritizes function, cognition, disability prevention, and quality of life, integrating disease-specific pathology with age-related vulnerability.[5] This is distinct from normal aging in the general population: the framework does not assume that hemoglobinopathy survivors are simply older, but rather that cumulative disease injury and decades of therapy can produce geriatric syndromes and loss of reserve at younger chronological ages than typically seen in unselected populations.
For this review, beyond midlife is intentionally pragmatic. We focus primarily on patients aged >=50 years, the phase when cumulative organ complications, multimorbidity, and functional vulnerability are increasingly likely to intersect, and when goal-based decision-making becomes essential. However, we also incorporate evidence from cohorts beginning at 40-49 years because older-adult definitions in sickle cell disease literature frequently begin at age 40, reflecting historical survival patterns and earlier accumulation of organ damage. We identify three mechanistic factors contributing to morbidity: disease-related pathology, treatment-related burdens, and biological and functional aging. This triad framework separates mechanisms that require different interventions and clarifies which clinical problems reflect age per se versus cumulative disease and treatment exposure.
Methodological Approach
This manuscript represents an expert opinion narrative review informed by a structured literature search, recognizing that prospective data on aging hemoglobinopathy populations remain limited and that many recommendations are necessarily based on observational cohorts, registries, and guideline extrapolation.We conducted a structured search of PubMed, Scopus, and Web of Science for studies published between 2000 and 2025. Search terms included combinations of thalassemia, sickle cell disease, aging, older adult, frailty, multimorbidity, functional decline, quality of life, and geriatric assessment. Priority was given to cohort studies, clinical guidelines, registry data, and systematic reviews relevant to adult and aging populations. We also reviewed reference lists of key articles to identify additional studies.
Inclusion criteria emphasized studies reporting outcomes or clinical characteristics in adult populations with explicit age stratification, preferably >=50 years and >=40 years when older-adult stratification began at that threshold. Exclusion criteria included pediatric-only studies without adult data, studies without age-stratified outcomes, and reports limited to isolated case descriptions when they did not inform broader clinical patterns.
In total, 52 publications informed the narrative synthesis. Because the literature is heterogeneous and this review was not designed as a formal systematic review, study selection is summarized narratively in the main text. A detailed summary of the search strategy, study selection rationale, study characteristics, and reasons for exclusion at full-text review is provided in the Supplementary File (Supplementary Table S1).
Definitions: Genotypes, Clinical Phenotypes, and Terminology
Throughout the manuscript, thalassemia refers to inherited disorders of reduced globin chain synthesis, including alpha-thalassemia, beta-thalassemia, and delta-beta-thalassemia. Genotype and modifier effects, including co-inheritance of alpha-thalassemia, HbE, or fetal hemoglobin-modulating variants, contribute to a spectrum of severity.[6,7]We use contemporary phenotype-based terminology when possible. Transfusion-dependent thalassemia refers to thalassemia requiring regular lifelong transfusion to survive and maintain adequate hemoglobin levels; non-transfusion-dependent thalassemia refers to thalassemia not requiring regular transfusions for survival but still associated with chronic anemia and significant long-term complications. Traditional terms such as thalassemia major and thalassemia intermedia are sometimes retained in the literature and are broadly aligned with these phenotypes, but do not fully capture clinical variability.[7,8]
Sickle cell disease refers to hemoglobin S-associated genotypes characterized by chronic hemolysis and vaso-occlusion, including HbSS and compound heterozygous forms such as HbSC and HbS/beta-thalassemia.[9] When clinical points apply predominantly to one subgroup, this is stated explicitly to avoid ambiguity (Table 1).
 |
|
Hemoglobinopathy Pathology and Gerontological Constructs
Hemoglobinopathies intersect with several biological pathways widely implicated in aging and age-related disease, including chronic low-grade inflammation, cellular senescence, and vascular aging. In classic gerontology, inflammaging refers to age-associated increases in pro-inflammatory signaling that contribute to organ dysfunction and increased vulnerability.[10]In hemoglobinopathies, chronic hemolysis, recurrent ischemia-reperfusion injury, transfusion exposure, and chronic pain syndromes can sustain inflammatory activation that may resemble inflammaging even at younger chronological ages, plausibly accelerating loss of physiologic reserve.
Similarly, cellular senescence is a hallmark of aging biology and has been proposed as a mechanistic contributor to functional decline.[11] While accelerated aging signatures have begun to be described in sickle cell disease, direct causal pathways linking molecular aging markers to clinical geriatric syndromes in older hemoglobinopathy cohorts remain incompletely established, and mechanistic claims should be interpreted cautiously.[12]
The overlap is clinically useful when used as a framework rather than a deterministic explanation. In thalassemia, long-term transfusion and iron overload can lead to cumulative oxidative stress and direct tissue injury, which may reduce organ reserve in the gerontological sense, lowering tolerance to acute illness, surgery, or medication changes. In sickle cell disease, recurrent vaso-occlusion and hemolysis can cause microvascular injury and endothelial dysfunction that parallels conceptual models of vascular aging, potentially amplifying risk when traditional cardiovascular risk factors emerge in midlife and later life.[13,14]
This section, therefore, supports a functional thesis: regardless of whether hemoglobinopathy injury is labeled accelerated aging, decades of disease activity and therapy exposure can produce phenotypes that resemble geriatric multimorbidity, including frailty, polypharmacy, cognitive vulnerability, and disability, earlier than expected by chronological age alone.
Functional Status, Frailty, and Quality of Life: The New Clinical Target
For decades, hemoglobinopathy care pivoted on a single metric: survival. Preventing death from acute chest syndrome, stroke, or cardiac decompensation was and remains essential. But a longer life without functional capacity is clinically hollow.Contemporary aging research demonstrates that functional status, not chronological age, predicts outcomes in chronic illness. Adults aging with hemoglobinopathies may exhibit functional decline, including weakness, slow gait, low activity, exhaustion, and weight loss, that overlaps with frailty syndromes in gerontology. Frailty remains under-recognized in hemoglobinopathy clinics because hematology practice is traditionally oriented toward organ-specific complications and crisis prevention rather than functional trajectories.[15]
Quality of life, cognitive function, employment, and intimate relationships are outcomes that matter profoundly to patients. Older adults with sickle cell disease describe the paradox of longer survival accompanied by persistent pain, fatigue, stigma, and loss of independence. Thalassemia cohorts report a similar tension between improved survival and the burden of endocrine, cardiac, and treatment-related complications that accumulate across decades. Functional and psychosocial endpoints must therefore be systematized in later-life hemoglobinopathy care, not treated as optional adjuncts.
For patients aged >=50 years, and earlier when functional concerns emerge, annual surveillance should include physical function, cognitive screening, depression and anxiety screening, social engagement, and employment or role status. Frailty screening tools should be incorporated, and if weakness is recognized, referral to physical medicine, geriatrics, rehabilitation, or structured exercise programs becomes urgent.[16,17] This conceptual framework is illustrated in Figure 1.
 |
|
Treatment And Follow-Up Evolve With Age: Balancing Benefit, Burden, And Reserve
As patients move beyond midlife, hemoglobinopathy treatment is rarely a simple continuation of pediatric-era targets. What changes is not only the accumulation of complications, but also the balance between treatment benefit and treatment burden in the context of multimorbidity, declining renal clearance, polypharmacy, and shifting patient priorities.In thalassemia, transfusion and chelation remain foundational, but the clinical question increasingly becomes how to sustain function and prevent irreversible decline while minimizing long-term toxicities. Volume tolerance, diastolic dysfunction, arrhythmias, and chronic kidney disease complicate transfusion delivery and may require slower transfusion protocols, individualized diuretic strategies, and closer monitoring of cardiac status. Chelation strategy often needs to evolve as renal impairment, hearing, and vision issues develop, and cumulative adherence fatigue can mandate dose adjustments, agent changes, or deliberate de-intensification when the competing risks and patient goals indicate diminishing marginal benefit.[18,19]
In sickle cell disease, major disease-modifying approaches, including hydroxyurea, transfusion-based strategies, and newer therapies, have been studied predominantly in younger cohorts, and older adults have historically been underrepresented in trials.[12] Beyond midlife, hydroxyurea dose titration may be constrained by renal function, marrow reserve, infection risk, and concomitant medications.[20] Transfusion decisions also increasingly intersect with comorbidity burden, alloimmunization history, and venous access complications.[21] In this setting, proactively defining realistic endpoints, including pain interference, mobility, cognitive stability, work capacity, and time spent outside the hospital, is often more meaningful than escalating therapy intensity by default.
Beyond age 50, the clinical unit of care should shift from reactive specialist visits to a planned annual comprehensive review that integrates organ surveillance with functional and psychosocial assessment. This visit should explicitly revisit goals of care, treatment tolerance, competing risks, and patient priorities, and should end with a written plan shared with primary care and key specialists.
Emerging Morbidities in Aging Hemoglobinopathies: The Disease-Driven and Treatment-Driven Triad
The spectrum of complications in hemoglobinopathy survivors reflects both disease-specific mechanisms and the cumulative effects of chronic treatment exposure. Importantly, many complications discussed below are not exclusive to later life: stroke, pulmonary complications, endocrine dysfunction, and pain can appear across the lifespan. What changes beyond midlife is the cumulative prevalence and severity of organ damage, the rising burden of age-associated comorbidities, and the decline in physiologic reserve that converts apparently stable disease into vulnerability to disability.[22]Major organ system complications in thalassemia and sickle cell disease are summarized in Tables 2 and 3.
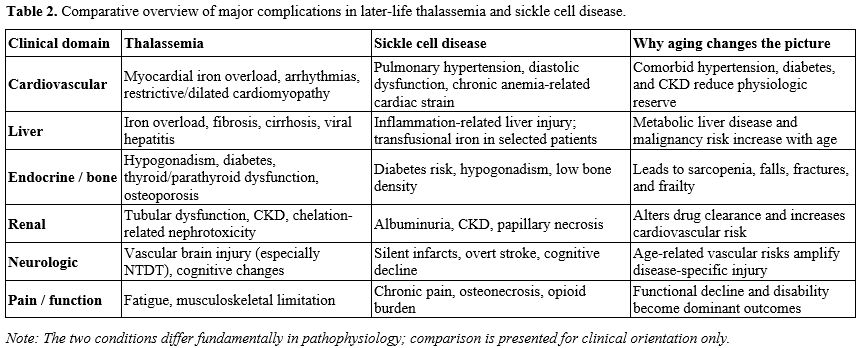 |
Table 2. Comparative overview of major complications in later-life thalassemia and sickle cell disease. |
 |
Table 3. Suggested comprehensive monitoring framework for adults ≥50 years with hemoglobinopathies. |
Cardiovascular complications and the paradox of iron. Cardiopulmonary disease is a major determinant of morbidity and mortality in both thalassemia and sickle cell disease, but the dominant mechanisms differ substantially.
In thalassemia, myocardial iron overload accumulates quietly, driven by transfusion burden and chelation adequacy. Iron-laden cardiomyocytes develop restrictive or dilated phenotypes; arrhythmias emerge as late, sometimes fatal complications. Cardiac MRI T2* remains central to monitoring and should not be replaced by ferritin alone.[23,24]
In sickle cell disease, cardiac strain more often reflects chronic anemia and hemolysis physiology, microvascular dysfunction, and cardiopulmonary disease, including pulmonary hypertension, rather than transfusional iron alone, except in those receiving long-term transfusions. Diastolic dysfunction is common, and the clinical impact is amplified when hypertension, diabetes, and kidney disease emerge beyond midlife.[25,26]
Elevated tricuspid regurgitant jet velocity on echocardiography is common in both conditions, but screening echocardiographic markers must be distinguished from hemodynamically confirmed pulmonary hypertension. In sickle cell disease, pulmonary hypertension is strongly associated with mortality risk. In thalassemia cohorts, elevated tricuspid regurgitant jet velocity has also been reported and may reflect complex cardiopulmonary physiology.
Clinical overview. Echocardiography remains a reasonable periodic screening tool in adults and should be interpreted in the context of age, symptoms, and comorbidities. In patients beyond midlife, escalation of monitoring frequency is most defensible when new symptoms, abnormal diastolic parameters, elevated tricuspid regurgitant velocity, or cardiovascular risk factors emerge. For thalassemia, cardiac MRI T2* should remain central in patients with significant transfusion burden or prior abnormal results. When pulmonary hypertension is suspected, right heart catheterization is required to define the mechanism and guide therapy.[27,28]
Complex combined pathology: hepatic fibrosis, iron overload, and metabolic liver disease. Liver iron concentration predicts morbidity and interacts with long-term outcomes. Yet in aging patients, at least two distinct pathologies may coexist: iron-driven fibrosis or cirrhosis and metabolic fatty liver disease.[29]
Iron overload and hepatic fibrosis are common in heavily transfused patients. Duration of iron overload, not just peak levels, appears clinically relevant. MRI-based liver iron quantification is generally preferred when available, particularly because inflammation and vascular congestion may complicate elastography interpretation.[30,31]
Metabolic-associated fatty liver disease is increasingly recognized among older patients with hemoglobinopathies and can coexist with iron overload. Distinguishing iron-driven from metabolic disease is clinically critical: iron disease demands chelation optimization; metabolic disease benefits from weight management, exercise, and metabolic control. Both can increase hepatocellular carcinoma risk. In cohorts transfused before modern viral screening, hepatitis C exposure remains common.[33,34,32]
Clinical overview. Liver surveillance should remain disease-specific, but beyond midlife, the stakes of cumulative fibrosis and malignancy risk become more consequential. Hepatitis B and C status should be assessed; a hepatology referral should follow evidence of advanced fibrosis; and hepatocellular carcinoma surveillance should be maintained when cirrhosis is present.
Diabetes, hypogonadism, sarcopenia, and bone loss. Endocrine dysfunction is common in older thalassemia patients, often reflecting decades of iron exposure, and also occurs in sickle cell disease. Iron deposition in pancreatic beta cells impairs insulin secretion, while hepatic iron and systemic inflammation amplify insulin resistance.[35]
Hypogonadotropic hypogonadism is a frequent endocrinopathy in thalassemia and contributes to sexual dysfunction, infertility, bone loss, and frailty.[36,37] Hypogonadism in sickle cell disease is less systematically documented and may be underrecognized. Thyroid and parathyroid disease are also common.[38]
Osteoporosis and sarcopenia are especially important beyond midlife because they convert chronic disease burden into falls, fractures, and loss of independence. The key issue in older adults is not simply detecting endocrinopathies but preventing functional consequences.[39]
Clinical overview. Screening for diabetes, thyroid dysfunction, gonadal dysfunction, calcium and vitamin D status, and bone density should be individualized by phenotype, transfusion exposure, symptoms, and age. Beyond age 50, the emphasis should shift from endocrine diagnosis alone to preservation of mobility, fracture prevention, and rehabilitation.
Renal impairment: drug clearance, imaging, and cardiovascular protection. Chronic kidney disease is an important emerging morbidity in aging hemoglobinopathy populations. Mechanisms differ by condition: vaso-occlusive injury and papillary necrosis in sickle cell disease; iron-related and anemia-related tubular dysfunction in thalassemia; and chronic hemolysis-associated tubular injury in both. Albuminuria is common and clinically meaningful.[40,41]
Renal impairment alters drug clearance and toxicity risk. A chelation strategy may need adjustment, imaging choices may be constrained, and hypertension and diabetes management become more urgent, as these risks compound hemoglobinopathy-related renal vulnerability.[42,43,44]
Clinical overview. Annual screening for albuminuria and glomerular filtration rate is reasonable in adulthood and becomes more consequential beyond midlife. Nephrology referral is appropriate for persistent albuminuria or reduced glomerular filtration rate, particularly when therapy adjustments are required.
Brain decline: stroke, silent infarction, and processing-speed loss. Cerebrovascular disease is a hallmark of sickle cell disease but can be under-recognized in adult practice. Overt stroke and silent cerebral infarction accumulate with age and interact with traditional vascular risk factors. Cognitive impairment is prevalent but often missed unless specifically assessed.[45,46,47]
In thalassemia, overt stroke is less typical, but vascular brain injury has increasingly been described, particularly in non-transfusion-dependent disease. Cognitive effects in thalassemia remain less well studied and probably heterogeneous.[48]
Clinical overview. Beyond midlife, cognitive screening becomes more clinically actionable because cognitive vulnerability interacts strongly with adherence, employment, driving safety, medication burden, and independent living. In adults with sickle cell disease, especially those with prior neurologic symptoms, hypertension, or functional decline, brain imaging may inform risk stratification, although evidence for universal adult MRI screening remains limited, and practice varies by setting.
Disability, opioid management, and chronic pain: a functional endpoint. In older adults, the approach to pain management should focus on functional outcomes rather than just pain scores.[49,50] Unlike acute vaso-occlusive crises, chronic baseline pain does not respond reliably to transfusions or hydroxyurea and often reflects mixed nociceptive, neuropathic, and centrally amplified mechanisms.[51] Osteonecrosis may become a dominant cause of reduced mobility.
Quality of life and functional status correlate strongly with pain interference and depression. These outcomes must be addressed directly, rather than inferred from hemoglobin values or hospital utilization alone.[52]
Clinical overview. Pain management in later life should be defined by functional endpoints rather than pain scores alone. Multimodal pain management, including non-opioid strategies, physical therapy, psychological interventions, and palliative-informed approaches, should be prioritized. In patients with progressive disability or severe symptom burden, palliative care consultation is appropriate even years from the end of life.
Remaining complications: pulmonary, thrombotic, infectious, and mental health. Pulmonary complications are a leading cause of morbidity and mortality in sickle cell disease and thalassemia patients, and cardiac iron overload or pulmonary hypertension are also risks. Chronic lung disease and obstructive sleep apnea are increasingly recognized but under-screened.[53,54,55,56] Venous thromboembolism risk is elevated, particularly in splenectomized patients or those with advanced kidney disease.[57,58] Infection risk and transfusion-related alloimmunization remain ongoing concerns.[59]
Depression and anxiety are highly prevalent. Stigma, discrimination, and social isolation compound psychological burden, particularly in older populations. Routine screening for depression and anxiety should be incorporated into later-life hemoglobinopathy care.[60]
Preventive Care and Shared Decision-Making in Older Age
Adults with hemoglobinopathies often receive inconsistent routine preventive care despite increasing survival into late adulthood in high-income settings. Barriers include crowded hematology schedules, lack of coordination between specialties, and assumptions that hemoglobinopathy-related risk dominates all other health priorities.Beyond age 50, clinicians should explicitly discuss preventive care goals and align them with life expectancy, functional status, and patient values. Preventive care decisions should be integrated into shared decision-making rather than occurring by default or omission. Hematology visits should not replace primary care but should reinforce coordination with primary care for cancer screening, cardiovascular risk management, vaccinations, bone health, and routine preventive services.[61]
Organizing Multidisciplinary Care: Principles For Complex Chronic Illness
Ideal multidisciplinary care involves hematologists, cardiologists, endocrinologists, hepatologists, nephrologists, neurologists, pulmonologists, pain specialists, psychologists, physical and occupational therapists, social workers, and pharmacists. Nevertheless, few centers can sustain all specialties on-site.[62]A pragmatic gerontology-informed model designates a hematology nurse coordinator or case manager as the hub: this person knows each patient, coordinates referrals, follows up on test results, and serves as the point of contact for patient questions. This is consistent with chronic care models and published standards emphasizing shared care arrangements among specialist centers, local hospitals, and primary or community care teams.
Specialized hemoglobinopathy centers should not function as the patient's de facto primary care provider. The most sustainable model in high-income settings is shared care: the specialist center serves as the disease-specific hub, responsible for hemoglobinopathy-directed management and coordinating multidisciplinary input, while primary care delivers routine preventive care and general chronic disease management, with clear communication and rapid re-access pathways to specialist expertise.[63]
The comprehensive annual review beyond midlife should integrate functional and psychosocial assessment, treatment tolerability review, medication review, and organ monitoring tailored to age, phenotype, and medical history. Shared decision-making should include explicit discussion of care goals, competing risks, the expected benefits versus burdens of interventions, and treatment acceptability.
Integrating Palliative Principles: A Shift in Clinical Mindset
Palliative care should not be confused with end-of-life care. This approach improves quality of life and functional status by addressing symptom burden, clarifying goals, and aligning medical interventions with patient values throughout all stages of disease.In older patients with hemoglobinopathy, this shift is particularly important because the dominant clinical threats often become pain interference, fatigue, disability, mood disorders, and caregiver burden, even when organ metrics appear stable. Standard hematology protocols may provide limited benefit if they do not address pain, mood, sleep, and social functioning.
Early palliative consultation, not triggered by crisis, provides patients and families with structured discussions regarding priorities, realistic expectations, and decision-making under competing risks. Palliative principles, including shared decision-making, goal clarification, symptom optimization, and psychosocial support, should be embedded in routine hemoglobinopathy care rather than reserved for late-stage scenarios.[63,64]
Research Priorities and Future Directions
Three critical gaps must be addressed.Prospective aging cohorts. Long-term studies of adults beyond midlife with thalassemia and sickle cell disease, incorporating standardized measures of frailty, cognition, disability, quality of life, and functional decline, are essential.
Interventional trials. Evidence-based trials of frailty reduction, sarcopenia management, cognitive rehabilitation, structured pain interventions, and psychosocial support remain limited. Trials should prioritize patient-reported outcomes and disability prevention alongside organ metrics and mortality.
Shared decision-making tools and care-delivery research. Monitoring strategies that integrate organ surveillance with functional assessment need evaluation, including comparative effectiveness of shared-care models, nurse navigation, telemedicine-supported specialty access, and multidisciplinary clinic structures across diverse health systems.
Conclusions
Three changes in clinical perspective are necessary as hemoglobinopathy patients move beyond midlife, particularly in high-income settings where survival into the 50s and beyond is increasingly common.Monitoring must evolve. The goal is not only to record cumulative damage but to detect treatable complications early and identify modifiable functional impairment. Beyond age 50, and earlier when clinical vulnerability emerges, routine assessments should include gait speed, grip strength, cognitive screening, depression screening, frailty screening, and social functioning.
Therapeutic decisions must weigh complexity. Blind adherence to pediatric-era protocols becomes ineffective in aging patients with polypharmacy, multiple organ involvement, and limited reserve. Shared decision-making should incorporate comorbidity burden, treatment acceptance, organ reserve, realistic benefit, and patient goals.
Care systems must integrate palliative principles and multidisciplinary coordination. Shared-care models in which specialist hemoglobinopathy centers function as disease-specific hubs, coordinating with primary care and local services, are more defensible than expecting specialist centers to replace primary care.
Hemoglobinopathies, as models of cumulative multimorbidity in lifelong genetic disease, offer gerontology both a clinical challenge and an opportunity. The survivors of these disorders demand that we move beyond pediatric emergency medicine and hematological metrics, and embrace the gerontological imperative: optimize function, prevent disability, clarify goals, alleviate suffering, and support the lived experience of growing old with chronic, complex, systemic disease.
Author Contributions
Sophia Delicou conceived the review concept, coordinated the multidisciplinary team, and drafted the manuscript. Constantina Aggeli and Elena Papatheodorou contributed to the cardiovascular sections and critical revision of the manuscript. Iliana Mani contributed to internal medicine perspectives and manuscript revision. Christos Savvidis and Ioannis Ilias contributed to the endocrinology sections. Panagiota Giannou and Athanasia Kapota contributed to the nephrology sections. Myrto Palkopoulou contributed to the neurology and cognitive impairment sections. Theodoros Aforozis contributed to the psychiatric and mental health sections. Irene Kouroukli contributed to the pain management sections. Alexandra Mika contributed to the imaging and radiological aspects of monitoring. Aikaterini Xydaki and Maria Moraki contributed to the sections on hemoglobinopathy clinical management. John Koskinas contributed to the conceptual framework and critical revision of the manuscript.All authors reviewed and approved the final version of the manuscript.
Acknowledgments
The authors acknowledge the multidisciplinary team of the Expertise Center of Hemoglobinopathies and their Complications at the General Hospital of Athens Hippokrateio for their clinical collaboration and ongoing commitment to the care of patients with hemoglobinopathies.References
- Borgna‐Pignatti C, Cappellini MD, De Stefano
P, Del Vecchio GC, Forni GL, Gamberini MR, Ghilardi R, Origa R, Piga A,
Romeo MA, Zhao H. Survival and complications in thalassemia. Annals of
the New York Academy of Sciences. 2005 Nov;1054(1):40-7. https://doi.org/10.1196/annals.1345.006 PMid:16339650
- Vichinsky EP. Changing patterns of thalassemia worldwide. Annals of the New York Academy of Sciences. 2005 Nov;1054(1):18-24. https://doi.org/10.1196/annals.1345.003 PMid:16339647
- Piel FB, Steinberg MH, Rees DC. Sickle cell disease. New England Journal of Medicine. 2017 Apr 20;376(16):1561-73. https://doi.org/10.1056/NEJMra1510865 PMid:28423290 PMCid:PMC11664321
- Kato
GJ, Piel FB, Reid CD, Gaston MH, Ohene-Frempong K, Krishnamurti L,
Smith WR, Panepinto JA, Weatherall DJ, Costa FF, Vichinsky EP. Sickle
cell disease. Nature reviews Disease primers. 2018 Mar 15;4(1):18010. https://doi.org/10.1038/nrdp.2018.10 PMid:29542687 PMCid:PMC11664321
- Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. The Lancet. 2013 Mar 2;381(9868):752-62. https://doi.org/10.1016/S0140-6736(12)62167-9 PMid:23395245 PMCid:PMC4098658
- Danjou F, Anni F, Galanello R. Beta-thalassemia: from genotype to phenotype. haematologica. 2011 Nov;96(11):1573. https://doi.org/10.3324/haematol.2011.055962 PMid:22058279 PMCid:PMC3208672
- Thein
SL, Wood WG. The Molecular Basis of ẞ Thalassemia, δβ Thalassemia, and
Hereditary Persistence of Fetal Hemoglobin. Disorders of hemoglobin:
genetics, pathophysiology, and clinical management. 2009 Aug 17:323. https://doi.org/10.1017/CBO9780511596582.023
- Diamantidis
MD, Ikonomou G, Argyrakouli I, Pantelidou D, Delicou S. Genetic
modifiers of hemoglobin expression from a clinical perspective in
hemoglobinopathy patients with beta thalassemia and sickle cell
disease. International Journal of Molecular Sciences. 2024 Nov
5;25(22):11886. https://doi.org/10.3390/ijms252211886 PMid:39595957 PMCid:PMC11593634
- Ballas
SK, Lieff S, Benjamin LJ, Dampier CD, Heeney MM, Hoppe C, Johnson CS,
Rogers ZR, Smith‐Whitley K, Wang WC, Telen MJ. Definitions of the
phenotypic manifestations of sickle cell disease. American journal of
hematology. 2010 Jan;85(1):6-13. https://doi.org/10.1002/ajh.21550 PMid:19902523 PMCid:PMC5046828
- Franceschi
C, Garagnani P, Parini P, Giuliani C, Santoro A. Inflammaging: a new
immune-metabolic viewpoint for age-related diseases. Nature Reviews
Endocrinology. 2018 Oct;14(10):576-90. https://doi.org/10.1038/s41574-018-0059-4 PMid:30046148
- López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The hallmarks of aging. Cell. 2013 Jun 6;153(6):1194-217. https://doi.org/10.1016/j.cell.2013.05.039 PMid:23746838 PMCid:PMC3836174
- Oyedeji
CI, Hodulik KL, Telen MJ, Strouse JJ. Management of Older Adults with
Sickle Cell Disease: Considerations for Current and Emerging Therapies:
CI Oyedeji et al. Drugs & aging. 2023 Apr;40(4):317-34. https://doi.org/10.1007/s40266-023-01014-8 PMid:36853587 PMCid:PMC10979738
- Fibach E, Dana M. Oxidative stress in β-thalassemia. Molecular diagnosis & therapy. 2019 Apr 1;23(2):245-61. https://doi.org/10.1007/s40291-018-0373-5 PMid:30484264
- Conran
N, Embury SH. Sickle cell vaso-occlusion: The dialectic between red
cells and white cells. Experimental Biology and Medicine. 2021
Jun;246(12):1458-72. https://doi.org/10.1177/15353702211005392 PMid:33794696 PMCid:PMC8243211
- Oyedeji
CI, Hall K, Luciano A, Morey MC, Strouse JJ. The sickle cell disease
functional assessment (SCD-FA) tool: a feasibility pilot study. Pilot
and feasibility studies. 2022 Mar 4;8(1):53. https://doi.org/10.1186/s40814-022-01005-3 PMid:35246265 PMCid:PMC8895638
- Di
Stefano V, Gianesin B, Bertini M, Culcasi M, Denotti AR, Derchi G,
Giuditta M, Longo F, Manca MR, Martinoli MC, Orecchia V. Atrial
fibrillation prevalence and its management in transfusion-dependent
thalassemias: the FATHAL study. Blood. 2023 Nov 2;142:2472. https://doi.org/10.1182/blood-2023-182773
- Morley
JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL)
predicts outcomes in middle-aged African Americans. The journal of
nutrition, health & aging. 2012 Aug;16(7):601-8. https://doi.org/10.1007/s12603-012-0084-2 PMid:22836700 PMCid:PMC4515112
- Taher AT, Musallam KM, Cappellini MD. β-Thalassemias. New England Journal of Medicine. 2021 Feb 25;384(8):727-43. https://doi.org/10.1056/NEJMra2021838 PMid:33626255
- Cappellini
MD, Motta I. New therapeutic targets in transfusion-dependent and
-independent thalassemia. Hematology 2014, the American Society of
Hematology Education Program Book. 2017 Dec 8;2017(1):278-83. https://doi.org/10.1182/asheducation-2017.1.278 PMid:29222267 PMCid:PMC6142569
- Di
Grazia D, Mirabella C, Chiara F, Caudana M, Shelton Agar FM, Zanatta M,
Allegra S, Bertello J, Voi V, Ferrero GB, Abbadessa G. Hydroxyurea
pharmacokinetic evaluation in patients with sickle cell disease.
Pharmaceuticals. 2024 Oct 17;17(10):1386. https://doi.org/10.3390/ph17101386 PMid:39459025 PMCid:PMC11510670
- Pirenne
F, Floch A, Diop S. Alloimmunisation against red blood cells in sickle
cell disease: transfusion challenges in high-income and low-income
countries. The Lancet Haematology. 2023 Jun 1;10(6):e468-76. https://doi.org/10.1016/S2352-3026(23)00066-2 PMid:37060916
- Delicou
S, Manganas K, Diamantidis MD, Venou TM, Delaporta P, Pantelidou D,
Spachiou E, Tsagia S, Pappi V, Petropoulou F, Kapsali E. Comparative
analysis of mortality patterns and treatment strategies in thalassaemia
and sickle cell disease patients: A 12‐year study. British Journal of
Haematology. 2025 May;206(5):1466-78. https://doi.org/10.1111/bjh.20043 PMid:40090899
- Di
Stefano V, Gianesin B, Orecchia V, Longo F, Susanna B, Barone A,
Culcasi M, Denotti AR, Costantini S, Ferrara F, Foggetti I. Atrial
fibrillation prevalence and its management in aging
transfusion-dependent thalassemia patients: the FATHAL study. Blood
Advances. 2026 Jan 22:bloodadvances-2025017577. https://doi.org/10.1182/bloodadvances.2025017577 PMid:41569798
- Pennell
DJ. T2* magnetic resonance and myocardial iron in thalassemia. Annals
of the New York Academy of Sciences. 2005 Nov;1054(1):373-8. https://doi.org/10.1196/annals.1345.045 PMid:16339685
- Gladwin
MT, Sachdev V, Jison ML, Shizukuda Y, Plehn JF, Minter K, Brown B,
Coles WA, Nichols JS, Ernst I, Hunter LA. Pulmonary hypertension as a
risk factor for death in patients with sickle cell disease. New England
Journal of Medicine. 2004 Feb 26;350(9):886-95. https://doi.org/10.1056/NEJMoa035477 PMid:14985486
- Gordeuk
VR, Castro OL, Machado RF. Pathophysiology and treatment of pulmonary
hypertension in sickle cell disease. Blood, The Journal of the American
Society of Hematology. 2016 Feb 18;127(7):820-8. https://doi.org/10.1182/blood-2015-08-618561 PMid:26758918 PMCid:PMC4760088
- Morris
CR, Kim HY, Trachtenberg F, Wood J, Quinn CT, Sweeters N, Kwiatkowski
JL, Thompson AA, Giardina PJ, Boudreaux J, Olivieri NF. Risk factors
and mortality associated with an elevated tricuspid regurgitant jet
velocity measured by Doppler-echocardiography in thalassemia: a
Thalassemia Clinical Research Network report. Blood, The Journal of the
American Society of Hematology. 2011 Oct 6;118(14):3794-802. https://doi.org/10.1182/blood-2010-11-319152 PMid:21772051 PMCid:PMC3193260
- Musallam
KM, Cappellini MD, Porter JB, Farmakis D, Taher AT. TIF guidelines for
the management of transfusion-dependent β-thalassemia. HemaSphere.
2025;9(3):e70095 https://doi.org/10.1002/hem3.70095 PMid:40045934 PMCid:PMC11880825
- Fragkou
N, Vlachaki E, Goulis I, Sinakos E. Liver disease in patients with
transfusion-dependent β-thalassemia: The emerging role of metabolism
dysfunction-associated steatotic liver disease. World Journal of
Hepatology. 2024 May 27;16(5):671. https://doi.org/10.4254/wjh.v16.i5.671 PMid:38818299 PMCid:PMC11135276
- Shah
FT, Porter JB, Sadasivam N, Kaya B, Moon JC, Velangi M, Ako E, Pancham
S. Guidelines for the monitoring and management of iron overload in
patients with haemoglobinopathies and rare anaemias. British Journal of
Haematology. 2022 Jan;196(2):336-50. https://doi.org/10.1111/bjh.17839 PMid:34617272 PMCid:PMC11969382
- Sarigianni
M, Liakos A, Vlachaki E, Paschos P, Athanasiadou E, Montori VM, Murad
MH, Tsapas A. Accuracy of magnetic resonance imaging in diagnosis of
liver iron overload: a systematic review and meta-analysis. Clinical
gastroenterology and hepatology. 2015 Jan 1;13(1):55-63. https://doi.org/10.1016/j.cgh.2014.05.027 PMid:24993364
- Delicou
S, Maragkos K, Tambaki M, Kountouras D, Koskinas J. Transient
elastography (TE) is a useful tool for assessing the response of liver
iron chelation in sickle cell disease patients. Mediterranean journal
of hematology and infectious diseases. 2018 Sep 1;10(1):e2018049. https://doi.org/10.4084/mjhid.2018.049 PMid:30210742 PMCid:PMC6131104
- Fragkou
N, Vlachaki E, Goulis I, Sinakos E. Liver disease in patients with
transfusion-dependent β-thalassemia: The emerging role of metabolism
dysfunction-associated steatotic liver disease. World Journal of
Hepatology. 2024 May 27;16(5):671. https://doi.org/10.4254/wjh.v16.i5.671 PMid:38818299 PMCid:PMC11135276
- Padeniya
P, Ediriweera D, De Silva AP, Niriella M, Premawardhena A. The
association between steatosis and liver damage in transfusion‐dependent
beta thalassaemia patients. British Journal of Haematology. 2023
Feb;200(4):517-23. https://doi.org/10.1111/bjh.18492 PMid:36194160
- Evangelidis
P, Venou TM, Fani B, Vlachaki E, Gavriilaki E. Endocrinopathies in
hemoglobinopathies: what is the role of iron?. International Journal of
Molecular Sciences. 2023 Nov 13;24(22):16263. https://doi.org/10.3390/ijms242216263 PMid:38003451 PMCid:PMC10671246
- Mahwi
TO, Rashid ZG, Ahmed SF. Hypogonadism among patients with
transfusion-dependent thalassemia: a cross-sectional study. Annals of
Medicine and Surgery. 2023 Jul 1;85(7):3418-22. https://doi.org/10.1097/MS9.0000000000000947 PMid:37427192 PMCid:PMC10328634
- De
Sanctis V, Soliman AT, Elsedfy H, Di Maio S, Canatan D, Soliman N,
Karimi M, Kattamis C. Gonadal dysfunction in adult male patients with
thalassemia major: an update for clinicians caring for thalassemia.
Expert review of hematology. 2017 Dec 2;10(12):1095-106. https://doi.org/10.1080/17474086.2017.1398080 PMid:29072100
- PARIZAD
N, AZAMI M, SAYEHMIRI K. Prevalence of Hypothyroidism,
Hypoparathyroidism and the Frequency of Regular Chelation Therapy in
Patients with Thalassemia Major in Iran: A Systematic Review and
Meta-analysis study.
- Thavonlun
S, Houngngam N, Kingpetch K, Numkarunarunrote N, Santisitthanon P,
Buranasupkajorn P, Pongchaiyakul C, Sutcharitchan P, Wattanachanya L.
Association of osteoporosis and sarcopenia with fracture risk in
transfusion-dependent thalassemia. Scientific Reports. 2023 Sep
29;13(1):16413. https://doi.org/10.1038/s41598-023-43633-6 PMid:37775530 PMCid:PMC10541420
- Abbasi
M, Srivastava A, Saraf SL. Management of kidney disease with sickle
cell disease. Journal of the American Society of Nephrology. 2024 Feb
6:10-681. https://doi.org/10.1681/ASN.0000000804 PMid:40569673 PMCid:PMC12499626
- Thongsaen
P, Tonsawan P, Wanitpongpun C, et al. Clinical features and risk
factors of renal dysfunction in thalassemia patients. Int Urol Nephrol.
2023;55(7):1779-1785. https://doi.org/10.1007/s11255-023-03506-3 PMid:36749473
- Romadhon
PZ, Ashariati A, Bintoro SU, Thaha M, Suryantoro SD, Windradi C, Mahdi
BA, Novendrianto D, Widiyastuti KN, Martani OS, Widiasi ED. Markers of
renal complications in beta thalassemia patients with iron overload
receiving chelation agent therapy: A systematic review. Journal of
Blood Medicine. 2022 Jan 1:725-38. https://doi.org/10.2147/JBM.S387416 PMid:36467279 PMCid:PMC9717586
- Capolongo
G, Zacchia M, Beneduci A, Costantini S, Cinque P, Spasiano A, De Luca
G, Di Pietro ME, Ricchi P, Trepiccione F, Capasso G. Urinary metabolic
profile of patients with transfusion-dependent β-thalassemia major
undergoing deferasirox therapy. Kidney and Blood Pressure Research.
2020 May 20;45(3):455-66. https://doi.org/10.1159/000507369 PMid:32434200
- Santos
S, Lousa I, Carvalho M, Sameiro-Faria M, Santos-Silva A, Belo L. Anemia
in elderly patients: contribution of renal aging and chronic kidney
disease. Geriatrics. 2025 Mar 14;10(2):43. https://doi.org/10.3390/geriatrics10020043 PMid:40126293 PMCid:PMC11932280
- Alakbarzade
V, Maduakor C, Khan U, Khandanpour N, Rhodes E, Pereira AC.
Cerebrovascular disease in sickle cell disease. Practical Neurology.
2023 Apr 1;23(2):131-8. https://doi.org/10.1136/pn-2022-003440 PMid:36123118
- Houwing
ME, Grohssteiner RL, Dremmen MH, Atiq F, Bramer WM, de Pagter AP, Zwaan
CM, White TJ, Vernooij MW, Cnossen MH. Silent cerebral infarcts in
patients with sickle cell disease: a systematic review and
meta-analysis. BMC Medicine. 2020 Dec 22;18(1):393. https://doi.org/10.1186/s12916-020-01864-8 PMid:33349253 PMCid:PMC7754589
- Charles
C, Bereznyakova O, Jacquin G, Bergeron J, Hafsaoui AY, Fraile V, Van
Synghel N, Arethuse AE, Kazadi C, St-Onge J, Desforges SM. Baseline
Neurological Morbidity Assessment in Adult Patients with Sickle Cell
Disease: The Montreal Brain-SCD Cohort. Blood. 2024 Nov 5;144:521. https://doi.org/10.1182/blood-2024-203020
- Hashemieh
M, Jafari N. Vascular brain damage in thalassemia syndrome: an emerging
challenge. Iranian Journal of Child Neurology. 2022 Jan 1;16(1):19.
- Glaros
A, Brandow AM. Neuropathic pain in sickle cell disease: measurement and
management. Hematology 2014, the American Society of Hematology
Education Program Book. 2020 Dec 4;2020(1):553-61.
- Karafin
MS, Simpson P, Field JJ. Chronic pain does not impact baseline
circulating cytokine levels in adults with sickle cell disease. Acta
Haematologica. 2021 Jan 25;144(1):111-6. https://doi.org/10.1159/000507563 PMid:32403100
- Demiray
DY, Oktay G. Association of depression and hydroxyurea use with
neuropathic pain in hemoglobinopathies. Scientific Reports. 2025 Oct
13;15(1):35750. https://doi.org/10.1038/s41598-025-20590-w PMid:41083566 PMCid:PMC12518568
- Yaya
I, Pourageaud A, Derbez B, Odièvre MH, Oudin Doglioni D, Podevin M,
Thomas G, Yombo-Kokule L, Godart C, Lepetit M, Cassubie-Mercier T.
Predictors of health-related quality of life in a large cohort of adult
patients living with sickle cell disease in France: the DREPAtient
study. Frontiers in Public Health. 2024 May 20;12:1374805. https://doi.org/10.3389/fpubh.2024.1374805 PMid:38832226 PMCid:PMC11144927
- Pervaiz
A, El-Baba F, Dhillon K, Daoud A, Soubani A. Pulmonary complications of
sickle cell disease: a narrative clinical review. Advances in
Respiratory Medicine. 2021 Apr 21;89(2):173-87. https://doi.org/10.5603/ARM.a2021.0011 PMid:33881157
- Vij R, Machado RF. Pulmonary complications of hemoglobinopathies. Chest. 2010 Oct 1;138(4):973-83. https://doi.org/10.1378/chest.10-0317 PMid:20923801
- Aessopos
A, Farmakis D. Pulmonary hypertension in β‐thalassemia. Annals of the
New York Academy of Sciences. 2005 Nov;1054(1):342-9. https://doi.org/10.1196/annals.1345.041 PMid:16339682
- Koelbel
M, Kirkham FJ. Sleep Behaviour in Sickle Cell Disease: A Systematic
Review and Meta-Analysis. Children. 2024 Dec 26;12(1):21. https://doi.org/10.3390/children12010021 PMid:39857852 PMCid:PMC11763464
- Babu K, Wun T. Sickle cell disease: managing thromboembolism. Hematology. 2025 Dec 5;2025(1):279-84. https://doi.org/10.1182/hematology.2025000715C PMid:41347992 PMCid:PMC12897942
- Danilatou
V, Papadakis E, Kyriakou E, Nomikou E, Delicou S, Girtovitis F.
Transfusion-Dependent Thalassemia and Venous Thromboembolism
Management: Position Statement from the Steering Committees of
Hemostasis and Erythrocyte and Hemoglobinopathies Study Groups-Hellenic
Society of Haematology. Seminars in Thrombosis and Hemostasis 2025 Aug
22. Thieme Medical Publishers, Inc. https://doi.org/10.1055/a-2669-7739 PMid:40730350
- Ladhani
SN, Fernandes S, Garg M, Borrow R, de Lusignan S, Bolton‐Maggs PH, BSH
Guidelines Committee. Prevention and treatment of infection in patients
with an absent or hypofunctional spleen: a British Society for
Haematology guideline. British Journal of Haematology. 2024
May;204(5):1672-86. https://doi.org/10.1111/bjh.19361 PMid:38600782
- Munung
NS, Treadwell M, Kamga KK, Dennis-Antwi J, Anie K, Bukini D, Makani J,
Wonkam A. Caught between pity, explicit bias, and discrimination: a
qualitative study on the impact of stigma on the quality of life of
persons living with sickle cell disease in three African countries.
Quality of Life Research. 2024 Feb;33(2):423-32. https://doi.org/10.1007/s11136-023-03533-8 PMid:37889387 PMCid:PMC10850006
- Oyedeji
CI, Hodulik KL, Telen MJ, Strouse JJ. Management of Older Adults with
Sickle Cell Disease: Considerations for Current and Emerging Therapies:
CI Oyedeji et al. Drugs & aging. 2023 Apr;40(4):317-34. https://doi.org/10.1007/s40266-023-01014-8 PMid:36853587 PMCid:PMC10979738
- Elwyn
G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P,
Cording E, Tomson D, Dodd C, Rollnick S, Edwards A. Shared decision
making: a model for clinical practice. Journal of general internal
medicine. 2012 Oct;27(10):1361-7. https://doi.org/10.1007/s11606-012-2077-6 PMid:22618581 PMCid:PMC3445676
- Légaré
F, Witteman HO. Shared decision making: examining key elements and
barriers to adoption into routine clinical practice. Health affairs.
2013 Feb 1;32(2):276-84. https://doi.org/10.1377/hlthaff.2012.1078 PMid:23381520
- Hargraves
I, LeBlanc A, Shah ND, Montori VM. Shared decision making: the need for
patient-clinician conversation, not just information. Health affairs.
2016 Apr 1;35(4):627-9. https://doi.org/10.1377/hlthaff.2015.1354 PMid:27044962
Supplementary Material
.

- Table 1. Literature Search Strategy and Study Selection Process
|
|