Immune checkpoint inhibitors (ICIs), such as pembrolizumab, have significantly improved outcomes in rr cHL, but they may also induce specific immune-related adverse events (irAEs).[3,4] Endocrine and cutaneous irAEs are the most frequently, while pulmonary involvement is less common but potentially severe and diagnostically challenging.[5]
Among pulmonary irAEs, sarcoid-like reactions (SLRs) are a rare and underrecognized entity that can closely mimic disease progression on imaging, particularly on FDG PET/CT.[6] In hematologic malignancies, data on SLRs are limited, as most reports originate from solid tumor settings, and these reactions are often categorized non-specifically as immune-mediated pneumonitis.[7]
A young woman with no relevant past medical history presented in early 2024 with left laterocervical lymphadenopathy, fever and night sweats. A lymph node biopsy established the diagnosis of cHL, nodular sclerosis subtype.
Baseline staging with FDG-PET showed multiple hypermetabolic cervical and thoracic lymph nodes, with the largest lesion in the anterior mediastinum (SUVmax 23.1). Whole-body CT revealed a solid parenchymal nodule with spiculated margins (15×11 mm) in the anterior segment of the right upper lobe adjacent to the mediastinal mass, as well as multiple ground-glass opacities, the largest measuring 18×10 mm, consistent with pulmonary involvement. These findings defined stage IV disease.
First-line therapy with brentuximab vedotin (BV) plus AVD (doxorubicin, vinblastine, and dacarbazine), was initiated. The patient, refractory, subsequently received two cycles of second-line BeGEV (bendamustine, gemcitabine, vinorelbine, and prednisone) chemotherapy with peripheral blood stem-cell mobilization, with the intent of autologous stem-cell transplantation (ASCT). However, post- cycle-2 reassessment demonstrated disease progression.
In light of data from the KEYNOTE-204 trial, third-line therapy with pembrolizumab 200 mg every three weeks was initiated.[8] Endocrinologic monitoring before and during treatment revealed no evidence of autoimmune toxicity.
After three cycles, the patient developed mild exertional dyspnea and dry cough. A PET scan was performed earlier than planned, showing complete metabolic response of the lymphoma but revealing new bilateral hilar (SUVmax 5) and subcarinal FDG uptake, along with faint hypermetabolism corresponding to subtle ground-glass opacities in the right upper lobe (SUVmax 2.8) and the middle and left lower lobes. These findings were initially interpreted as inflammatory and, after multidisciplinary discussion with the interventional pulmonology team, pembrolizumab was continued with close radiologic monitoring.
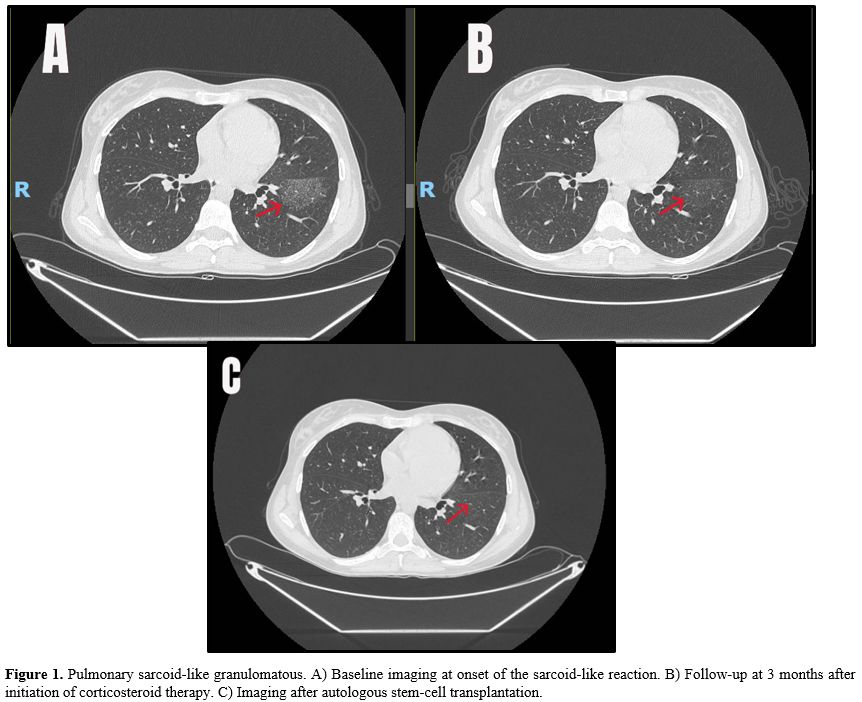
At post-cycle-6 evaluation, PET findings were stable. High-resolution CT (HRCT) demonstrated multiple nodular ground-glass opacities in both lungs, particularly in the apical segment of the right upper lobe (32 × 25 mm), the left lower lobe (48 × 20 mm), and the right lower lobe (30 × 30 mm), associated with centrilobular micronodules (Figure 1, A).
 |
|
Bronchoscopy with transbronchial biopsy, revealed chronic granulomatous inflammation with Langherans-type giant cells, without evidence of lymphoma. Microbiological investigations were negative. These findings supported a diagnosis of immune-mediated pneumonitis with SLRs related to pembrolizumab.
Pembrolizumab was permanently discontinued, and prednisone 0.5 mg/kg/day was administered for 21 days, followed by radiologic reassessment. Follow-up HRCT demonstrated radiologic stability with partial resolution of ground-glass opacities (Figure 1, B). Pulmonary function tests were normal, and pulmonology consultation found no contraindication to proceeding with ASCT. Therefore, a steroid tapering over three months was performed.
The patient subsequently underwent ASCT with BEAM (carmustine, etoposide, cytarabine, and melphalan) conditioning without pulmonary or other transplant-related complications. Post-transplant chest CT showed further resolution of pulmonary findings (Figure 1, C). PET imaging performed three months after transplantation confirmed complete remission. Patient gave consent to publish her data and images.
Pembrolizumab is widely used in rrHL and has demonstrated durable clinical responses;[6,8] immune checkpoint inhibition can result in irAEs due to dysregulated immune activation. Among these, SLRs are rare granulomatous inflammatory manifestations that remain poorly characterized in the hematologic setting.[6] Their pathogenesis is not fully established, but PD-1 inhibition is thought to promote an exaggerated T-helper 1 immune response, leading to increased cytokine production, including tumor necrosis factor-α, which favors granuloma formation.[6,9]
Pulmonary SLRs typically develop after several cycles of ICI, most commonly between the third and sixth infusion and may present with bilateral hilar or mediastinal lymphadenopathy, diffuse micronodules, and ground-glass opacities with a perilymphatic distribution. Becausethese lesions are often FDG-avid, they may be mistaken for lymphoma persistence or progression, representing a particularly relevant pitfall in cHL, where PET/CT is central to response assessment.[6,10]
Accurate diagnosis requires careful correlation of clinical, radiological, and histological (non-caseating granulomas) data.[9]
According to current guidelines for irAEs, management depends on severity: asymptomatic or mildly symptomatic patients may benefit from a temporary treatment interruption and close monitoring, whereas symptomatic patients generally require corticosteroid therapy, typically prednisone at 0.5–1 mg/kg/day with gradual tapering over 4–6 weeks.[11,12]
In the present case, early recognition of the SLR, avoided misclassification as refractory lymphoma and allowed appropriate steroid treatment, preservation of the transplant strategy, and successful completion of ASCT without pulmonary complications.
In conclusion, pulmonary SLR is a rare but clinically relevant irAE associated with pembrolizumab in HL. Its radiologic features may closely resemble disease progression, potentially leading to inappropriate therapeutic decisions. Increased awareness, multidisciplinary evaluation, and histologic confirmation are essential for correct diagnosis and management, allowing continuation of optimal treatment strategies when appropriate.
References
- Ansell SM. Hodgkin lymphoma: 2025 update on
diagnosis, risk-stratification, and management. Am J Hematol. 2024
Dec;99(12):2367-2378. https://doi.org/10.1002/ajh.27470 PMid:39239794 PMCid:PMC12083808
- Dalton
M Craven, Meagan J Harrington, Griffin M Sansbury, Tarsizious
Chikaonda, Marriam Mponda, Claire T Pedersen, Karen S Grigg, Hannah
Burrows, Matthew S Painschab. Hodgkin lymphoma treatment patterns and
outcome disparities in low- and middle-income countries: A systematic
review. Blood Global Hematology, 2025. 100021, ISSN 3050-5658. https://doi.org/10.1016/j.bglo.2025.100021 PMCid:PMC13274657
- Boucheron
T, Chiche L, Penaranda G, Souquet M, Pegliasco H, Deturmeny J, Brunel
V, Barrière N, Arbault-Bitton C, Coquet E, Diaz L, Escoda T. Risk of
Serious Immune-Related Adverse Events with Various PD1 and PD-L1
Inhibitors: A Single-Institution, Real-Life, Comparative Study. Ther
Clin Risk Manag. 2025 Mar 5;21:273-282. https://doi.org/10.2147/TCRM.S479686 PMid:40060169 PMCid:PMC11890422
- Argnani
L, Stefoni V, Casadei B, Pelusi C, Preiato VL, Pagotto U, Buganè A,
Pellegrini C, Broccoli A, Zinzani PL. Immune-related adverse events in
the treatment of Hodgkin lymphoma with immune checkpoint inhibitors. Br
J Haematol. 2026 Feb 26. https://doi.org/10.1111/bjh.70402 PMid:41744197 PMCid:PMC13176520
- Furrer-Matcau
C, Sieber C, Lehnick D, Brand CU, Hug B. Cutaneous adverse events due
to checkpoint inhibitors - a retrospective analysis at a tertiary
referral hospital in Switzerland 2019-2022. Front Oncol. 2024 Dec
5;14:1485594. https://doi.org/10.3389/fonc.2024.1485594 PMid:39703836 PMCid:PMC11655322
- Gkiozos
I, Kopitopoulou A, Kalkanis A, Vamvakaris IN, Judson MA, Syrigos KN.
Sarcoidosis-Like Reactions Induced by Checkpoint Inhibitors. J Thorac
Oncol. 2018 Aug;13(8):1076-1082. doi: 10.1016/j.jtho.2018.04.031. Epub
2018 May 12. https://doi.org/10.1016/j.jtho.2018.04.031 PMid:29763666
- Sacks
EL, Donaldson SS, Gordon J, Dorfman RF. Epithelioid granulomas
associated with Hodgkin's disease: clinical correlations in 55
previously untreated patients. Cancer. 1978 Feb;41(2):562-7.
https://doi.org/10.1002/1097-0142(197802)41:2<562::AID-CNCR2820410224>3.0.CO;2-X PMid:630538
- Kuruvilla
J, Ramchandren R, Santoro A, Paszkiewicz-Kozik E, Gasiorowski R,
Johnson NA, Fogliatto LM, Goncalves I, de Oliveira JSR, Buccheri V,
Perini GF, Goldschmidt N, Kriachok I, Dickinson M, Komarnicki M,
McDonald A, Ozcan M, Sekiguchi N, Zhu Y, Nahar A, Marinello P, Zinzani
PL; KEYNOTE-204 investigators. Pembrolizumab versus brentuximab vedotin
in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): an
interim analysis of a multicentre, randomised, open-label, phase 3
study. Lancet Oncol. 2021 Apr;22(4):512-524. doi:
10.1016/S1470-2045(21)00005-X. Epub 2021 Mar 12. Erratum in: Lancet
Oncol. 2021 May;22(5):e184. https://doi.org/10.1016/S1470-2045(21)00005-X PMid:33721562
- Yousuf
H, Mekki R, Khan K, Hussain A. Pembrolizumab-Induced Sarcoid-Like
Reaction in a Patient With Lung Cancer. Cureus. 2020 Dec
31;12(12):e12395. https://doi.org/10.7759/cureus.12395
- Li
Y, Flavell RR, Juarez R, Chow M, Wu C, Tsai K, Daud A, Behr SC.
Retrospective study of the incidence of sarcoidosis-like reaction in
patients treated with immunotherapy. Clin Radiol. 2023
Feb;78(2):e131-e136. https://doi.org/10.1016/j.crad.2022.09.127 PMid:36344282
- Schneider
BJ, Naidoo J, Santomasso BD, Lacchetti C, Adkins S, Anadkat M, Atkins
MB, Brassil KJ, Caterino JM, Chau I, Davies MJ, Ernstoff MS, Fecher L,
Ghosh M, Jaiyesimi I, Mammen JS, Naing A, Nastoupil LJ, Phillips T,
Porter LD, Reichner CA, Seigel C, Song JM, Spira A, Suarez-Almazor M,
Swami U, Thompson JA, Vikas P, Wang Y, Weber JS, Funchain P, Bollin K.
Management of Immune-Related Adverse Events in Patients Treated With
Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J Clin
Oncol. 2021 Dec 20;39(36):4073-4126. https://doi.org/10.1200/JCO.21.01440 PMid:34724392
- Haanen J, Obeid M, Spain L, Carbonnel F, Wang Y, Robert C, Lyon AR, Wick W, Kostine M, Peters S, Jordan K, Larkin J; ESMO Guidelines Committee. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022 Dec;33(12):1217-1238. https://doi.org/10.1016/j.annonc.2022.10.001 PMid:36270461