Case Presentation
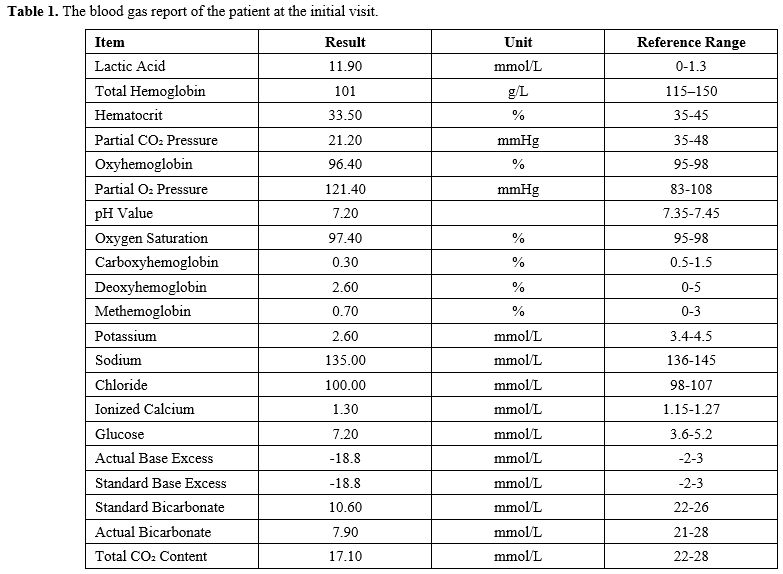
The patient’s clinical course can be divided into two phases.Phase 1 – Initial presentation and glucocorticoid therapy. A 43 year old woman presented with a 50 day history of nausea, weight loss, and progressive fatigue. CT scan revealed no significant hepatosplenomegaly, lymphadenopathy, masses, or renal abnormalities. Initial labs showed mild cytopenias: WBC 2.79×10⁹/L (normal 3.5–9.5×10⁹/L), hemoglobin 101 g/L (normal 115–150 g/L), platelets 161×10⁹/L (normal 125–350×10⁹/L). Creatinine was 1.69 mg/dL (normal 0.5–1.1 mg/dL), along with hypokalemia and severe metabolic acidosis. Arterial blood gas revealed lactic acidosis (lactate 11.9 mmol/L; normal 0–1.3 mmol/L), low bicarbonate (7.9 mmol/L; normal 21–28 mmol/L), and pH 7.20 (normal 7.35–7.45), consistent with a high anion gap metabolic acidosis (Table 1). There was no evidence of sepsis, hypoperfusion, or drug toxicity. The initial differential diagnosis included renal tubular acidosis and acute interstitial nephritis. The patient was started on supportive care plus oral methylprednisolone (24 mg/day). Ten days later, follow up tests showed improvement: lactate fell to 6.90 mmol/L, pH rose to 7.46, and creatinine dropped to 1.20 mg/dL. She was discharged on a tapering steroid regimen. After discharge, her laboratory values continued to fluctuate: creatinine 1.15–2.04 mg/dL, WBC 2.36–5.27×10⁹/L, lactate 5.1–10.9 mmol/L, pH 7.22–7.43, hemoglobin 71–176 g/L, and platelets 102–157×10⁹/L. Glucocorticoid therapy was given for a total of three months.
 |
|
Phase 2 – Diagnostic work up and confirmation of B lymphoblastic leukemia/lymphoma. One week after stopping the drug, the patient experienced worsening nausea, vomiting, palpitations, dyspnea, and lower limb weakness. Upon readmission, tests showed metabolic decompensation: pH 7.31, lactate 14.80 mmol/L, and creatinine 3.39 mg/dL. PET/CT revealed: (1) multifocal hypermetabolic lymphadenopathy (SUVmax 6.9) involving bilateral cervical, supraclavicular, axillary, hilar, mediastinal, and retroperitoneal regions, along with splenomegaly (SUVmax 6.0); (2) bilateral renal enlargement with diffuse hypermetabolism (SUVmax 10.2); (3) diffuse bone marrow hypermetabolism (SUVmax 11.8); and (4) thyroid and uterine abnormalities (SUVmax 3.5 and 4.6, respectively). Guided by these PET/CT findings, bone marrow aspiration was performed. The aspirate showed 24% hematoblasts. In addition, monoblasts and promonocytes accounted for 7.5%, and unclassified cells (large, with loose chromatin and gray blue cytoplasm containing many vacuoles) made up 22%. Flow cytometry identified an abnormal population comprising 74.59% of nucleated cells, expressing CD34, CD38, CD33, CD123, CD19, CD56, CD22, cCD79a, TdT, and HLA DR, with partial CD9 and weak CD11b expression. Karyotype analysis revealed complex abnormalities: 46,X,t(X;9)(q21;p21), +1; der(1;16)(q10;p10), t(2;14)(p10;p10) [16]/47,idem,+8[1]/46,idem,+11,der(11;17)(q10;q10)[1]/46XX[2]. PCR for 43 leukemia associated fusion genes and a 29 gene Ph like acute lymphoblastic leukemia (ALL) panel was negative. Targeted next generation sequencing identified ETV6 p.K302Gfs25 and three KMT2D mutations: p.G5001Rfs6, p.R4198X, and p.F1538Lfs*26. These findings confirmed the diagnosis of B lymphoblastic leukemia/lymphoma. The patient left the hospital voluntarily and died suddenly one week later.
Discussion
According to the 5th edition of the WHO classification of haematolymphoid tumors, a bone marrow blast count of 25% or more is one of the diagnostic criteria for ALL.[1] In our patient, the bone marrow smear showed not only 24% lymphoblasts, but also 7.5% monoblasts and promonocytes, and 22% unclassified cells. Flow cytometry identified a lymphoblastic cell population accounting for 74.59%. Taken together, we consider that all three cell types belong to the same neoplastic clone. Therefore, this case is best classified as B lymphoblastic leukemia/lymphoma. It is worth noting that most published cases of lactic acidosis associated with lymphoblastic neoplasms involved T cell lymphoblastic lymphoma.[2]This case illustrates several important diagnostic considerations.
First, Type B lactic acidosis is a well-recognized but uncommon complication of hematologic malignancies. It results from increased lactate production via aerobic glycolysis (Warburg effect) combined with impaired clearance.[3,4] In our patient, the absence of hypoperfusion suggests that a non hypoxic mechanism – most likely the Warburg effect – was involved. Additionally, PET CT showed bilateral renal and hepatic hypermetabolism, raising the possibility of neoplastic infiltration. If present, such infiltration might have further impaired lactate elimination.[5] However, because no renal or liver biopsy was performed, direct evidence for this mechanism was insufficient, and these explanations remain plausible hypotheses.
Second, AKI in leukemia is multifactorial, including prerenal, intrinsic, and postrenal causes.[6–8] In this case, PET/CT showed bilateral renal hypermetabolism, raising the possibility of neoplastic infiltration, which might have contributed to both renal dysfunction and impaired lactate clearance, though lacking pathological confirmation. Retrospective analysis revealed no evidence of prerenal or postrenal contributors, pointing to intrinsic renal AKI attributable to tubulointerstitial disease. Notably, approximately 50% of such cases involve multifactorial mechanisms.[8]
Third, the aleukemic presentation with only mild cytopenias represents a major diagnostic challenge. The absence of circulating blasts delayed hematologic evaluation despite persistent metabolic abnormalities. Peripheral blood counts fluctuated within a narrow range without overt blasts — a well-recognized but easily overlooked presentation of acute leukemia.[9,10] In such atypical cases, even subtle cytopenias should lower the threshold for bone marrow examination.
Finally, the transient improvement with glucocorticoids likely reflects partial cytoreduction, further masking the underlying disease and contributing to diagnostic delay.[4,5] This partial response should not be misinterpreted as resolution of the underlying condition.
Key Diagnostic Triggers
• Type B lactic acidosis without hypoperfusion suggests occult malignancy.• Unexplained AKI with systemic symptoms needs a hematologic workup.
• Mild or fluctuating cytopenias in atypical cases warrant early bone marrow exam.
• Temporary steroid response can mask underlying leukemia/lymphoma.
Conclusions
Unexplained metabolic acidosis and AKI may represent early manifestations of lymphoblastic leukemia/lymphoma, even in the absence of peripheral blasts. Early consideration of hematologic malignancy and prompt bone marrow evaluation are essential to avoid diagnostic delay. This case underscores the importance of integrating metabolic, renal, and hematologic findings in patients with atypical presentations.Ethics approval
The study protocol was approved by the Medical Ethics Committee of the affiliated hospital of Qingdao University (QDFY+X2021045). The study was in accordance with the Declaration of Helsinki.Patient consent for publication
Written informed consent was obtained from the patient.Author contributions
Zhan Su and Yan Jiang designed the study and wrote the manuscript. Qingyun Fan collected the clinical information. All authors read and approved the final manuscript.References
- WHO Classification of Tumors Editorial Board. WHO
classification of tumors series: Haematolymphoid tumors., 5th ed. Lyon
(France): International Agency for Research on Cancer; 2024; pp
330-5.
- Özdemir
ZÖ, Özdemir E, Halaçlı B, Güven G, Topeli A. A rare clinical
manifestation of lactate elevation explained by the Warburg effect:
report of two lymphoma cases and literature review. Turk J Intensive
Care. 2025 Dec;23(4):326-34. https://doi.org/10.63729/TJIC.2025.677
- Liberti MV, Locasale JW. The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem Sci. 2016 Mar;41(3):211-8. https://doi.org/10.1016/j.tibs.2015.12.001 PMid:26778478 PMCid:PMC4783224
- Padda J, Khalid K, Kakani V, Cooper AC, Jean-Charles G. Metabolic Acidosis in Leukemia. Cureus. 2021 Sep;13(9):e17732. https://doi.org/10.7759/cureus.17732
- De
Keulenaer B, Van Outryve S, De Backer A, Van Overbeke L, Daelemans R,
Van Marck E, Schepens D, Stephens D. Symptomatic lactic acidosis due to
relapse of T-cell acute lymphoblastic leukemia in the kidney.
Nephrology Dialysis Transplantation. 2003 Jun;18(6):1214-6. https://doi.org/10.1093/ndt/gfg053 PMid:12748358
- Canet
E, Zafrani L, Lambert J, Thieblemont C, Galicier L, Schnell D, Raffoux
E, Lengline E,Chevret S, Darmon M, Azoulay E. Acute Kidney Injury in
Patients with Newly Diagnosed High-Grade Hematological Malignancies:
Impact on Remission and Survival. PLoS ONE. 2013 Feb;8(2):e55870. https://doi.org/10.1371/journal.pone.0055870 PMid:23457485 PMCid:PMC3573047
- Ganguli
A, Sawinski D, Berns JS. Kidney diseases associated with haematological
cancers. Nat Rev Nephrol. 2015 Aug;11(8):478-90. https://doi.org/10.1038/nrneph.2015.81 PMid:26035773
- Hazim
H, Chacko B. Acute kidney injury in acute leukaemia: there is more to
this than meets the eye. Internal Medicine Journal. 2025
Jan;55(1):165-6. https://doi.org/10.1111/imj.16620 PMid:39815645
- Ghrewati
M, Manji F, Modi V, Chandran C, Maroules M. Severe Metabolic Acidemia
in a Patient with Aleukemic Leukemia. Case Reports in Nephrology. 2018
Nov;2018:1-5. https://doi.org/10.1155/2018/1019034 PMid:30581637 PMCid:PMC6276439
- Vagha K, Bakane A, Malik A, Javvaji CK, Vagha S, Murhekar S. Unmasking the Rarity: A Case Report on Type B Lactic Acidosis in Pediatric Acute Lymphoblastic Leukemia. Cureus. 2024 May DOI: 10.7759/cureus.61201 https://doi.org/10.7759/cureus.61201