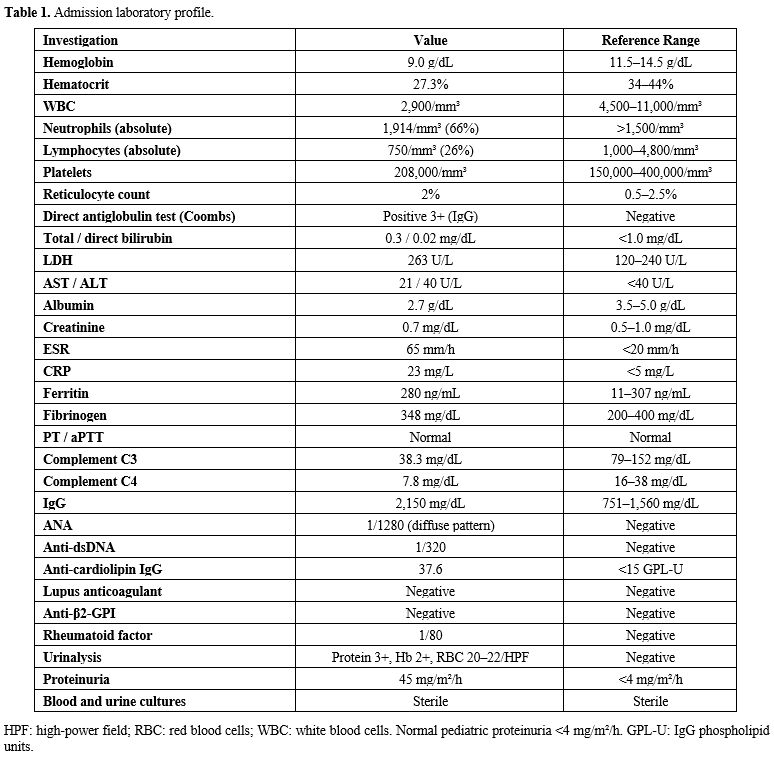
At the referring hospital (Day 14 of illness), clinical examination demonstrated a malar rash, borderline splenomegaly, and reduced breath sounds at the lung bases. Laboratory results showed: hemoglobin (Hb) 9 g/dL (MCV 78 fL) with a positive direct antiglobulin test (DAT, IgG subtype) without evidence of active hemolysis; leukopenia (leukocytes 2,900/mm³) with lymphopenia (750/mm³); elevated inflammatory markers (ESR 65 mm/h, CRP 23 mg/L), ferritin 280 ng/mL, hypoalbuminemia (2.7 g/dL); hypocomplementemia (C3 38.3mg/dL, C4 7.8 mg/dL) and urinalysis with proteinuria and hemoglobinuria. An autoimmune process was suspected, and she was referred to our hospital.
In-Hospital Course (Day 15 of Illness)
Initial Management and Clinical Deterioration. On admission, vital signs were stable except for tachycardia (128 bpm). Physical examination revealed basal breath sounds with dullness, mild splenomegaly, malar rash, livedo reticularis of the extremities, and frontotemporal alopecia. Joints and lymph nodes were normal.Laboratory evaluation at admission was similar to day 14 and the results are detailed in Table 1. Immunological profiling confirmed ANA (1/1280, diffuse pattern), anti-dsDNA (1/320), hypergammaglobulinemia, markedly reduced C3/C4, and anti-cardiolipin IgG (37.6 GPL-U). Urinalysis showed microscopic hematuria and proteinuria (45 mg/m²/hour). Imaging revealed bilateral pleural effusions, hepatosplenomegaly on ultrasound, and a small pericardial effusion on echocardiography.
 |
|
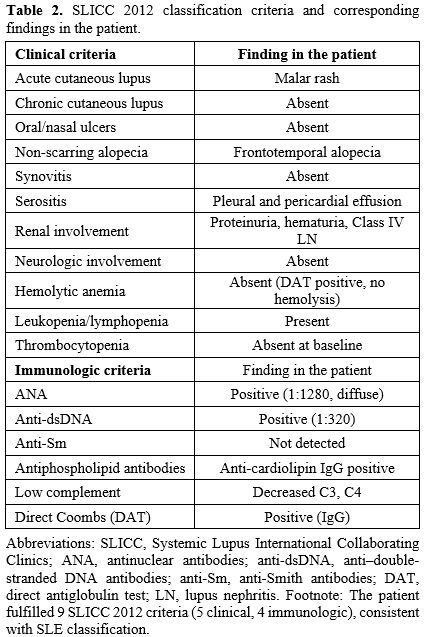
The patient fulfilled 9 Systemic Lupus International Collaborating Clinics Classification (SLICC) 2012 criteria (5 clinical, 4 immunologic), consistent with SLE classification (Table 2).[1]
 |
|
Despite the compelling evidence for SLE, a simultaneous and systematic workup for fever of unknown origin was undertaken given the patient’s rural background. Extended infectious disease serology for CMV, EBV, HSV, Toxoplasma, Brucella, Bartonella, Borrelia, Leptospira, Rickettsia, Hepatitis A/B/C, and HIV was entirely negative. Leishmania serology by enzyme-linked immunosorbent assay (ELISA) and indirect immunofluorescence assay (IFA) was also negative. The Mantoux test was anergic (0 mm).
Initial Management and Clinical Deterioration. On Day 16 of illness (Day 2 of hospitalization), a bone marrow aspirate was performed to investigate persistent cytopenias in the context of fever and hepatosplenomegaly. Cytological examination showed a normocellular marrow with trilineage hematopoiesis, no evidence of malignancy, dysplasia, granulomatous inflammation, hemophagocytosis, or Leishmania; flow cytometry was unremarkable, and cultures remained sterile. A kidney biopsy was also performed on the same day. While awaiting the renal biopsy result, prednisolone was commenced at 1 mg/kg/day, together with an angiotensin-converting enzyme (ACE) inhibitor (ramipril 0.1 mg/kg/day) and hydroxychloroquine (5 mg/kg/day).
On Day 22 of illness (Day 8 of hospitalization), significant clinical worsening occurred: high-grade fever returned to up to 40°C and proteinuria worsened to 100 mg/m²/h, while serum creatinine remained normal.
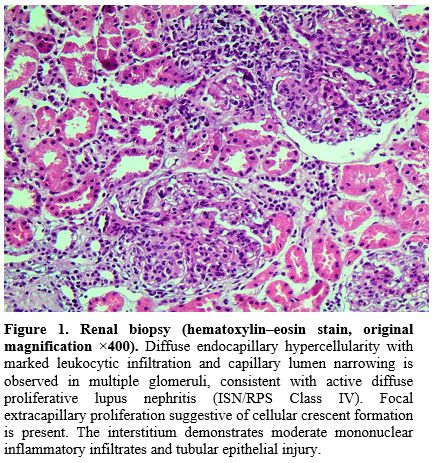
Renal Biopsy and Acute Deterioration (Day 28 of Illness). The renal biopsy result became available on Day 28 (Day 14 of hospitalization). Light microscopy of 12 glomeruli demonstrated moderate mesangial expansion, endocapillary hypercellularity with endothelial cell proliferation, fibrocellular crescents in 2 glomeruli, and segmental sclerosis in 1 glomerulus. Immunofluorescence showed granular mesangial and subendothelial deposits in a full-house pattern: IgG (2+), IgA (1+), IgM (3+), C3 (3+), C1q (3+). The histological diagnosis was Class IV diffuse proliferative lupus nephritis (ISN/RPS 2003) (Figure 1).[2]
 |
|
On the same day, the patient developed petechiae and increased bleeding tendency with rapid laboratory deterioration: ferritin 13,900 ng/mL; platelets 67,000/mm³; absolute neutrophil count (ANC) 1,290/mm³; hemoglobin 9.5 g/dL; fibrinogen 1.28 g/L; triglycerides 368 mg/dL (fasting); LDH 336 U/L; AST 209 U/L; ALT 88 U/L. A repeat bone marrow aspirate now showed numerous activated macrophages with unequivocal hemophagocytosis (engulfment of erythrocytes, erythroid precursors, platelets, and neutrophils); again, no Leishmania amastigotes were identified.
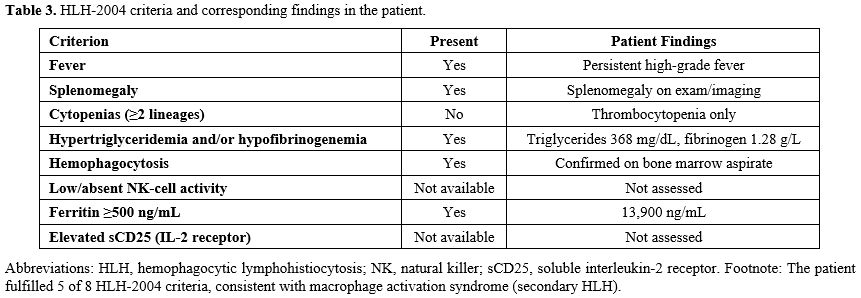
Five of the eight HLH-2004 criteria[3] were met (Table 3): fever, splenomegaly, hyperferritinemia (13,900 ng/mL), hypertriglyceridemia (368 mg/dL), and confirmed hemophagocytosis on bone marrow aspirate. The cytopenia criterion was not formally met (thrombocytopenia only); natural killer (NK)-cell activity and sCD25 were unavailable locally. MAS was further confirmed by an H Score ≥170.[4] Three consecutive intravenous pulses of methylprednisolone (1 g/day) were administered for MAS and Class IV LN. Mycophenolate mofetil (MMF) (2 g/day) was added; oral prednisolone 1 mg/kg/day was continued, together with ramipril and hydroxychloroquine. Cotrimoxazole prophylaxis (trimethoprim 5 mg/kg/day, 3 days/week) was initiated. A calcineurin inhibitor (CNI) was deliberately withheld given active clinical suspicion of an undiagnosed intracellular infection. Given the endemic context - the patient’s lifelong residence in a Leishmania infantum-endemic region - bone marrow and peripheral blood were submitted for Leishmania PCR (kDNA minicircle target) despite persistently negative serology.
 |
|
The Diagnostic Turning Point: A Positive PCR (Day 30 of Illness)
On Day 30 (Day 16 of hospitalization), the Leishmania PCR returned positive for Leishmania infantum from the bone marrow and negative from the peripheral blood. Repeated Leishmania serology by ELISA and IFA remained entirely negative at this point. In the context of the patient’s immunocompromised state, seronegative PCR-confirmed VL was interpreted as most likely representing reactivation of a latent Leishmania infantum infection under iatrogenic and disease-related immunosuppression, consistent with the patient’s lifelong residence in an endemic area.[5,6] Seroconversion was ultimately observed only at Month 5 of follow-up.The complete diagnosis was therefore: severe SLE with Class IV diffuse proliferative lupus nephritis, complicated by macrophage activation syndrome and seronegative visceral leishmaniasis (Leishmania infantum), with VL reactivation considered the most plausible precipitant of MAS.
Therapeutic Dilemma and Resolution. This diagnosis introduced a critical therapeutic dilemma: aggressive immunosuppression was required for Class IV LN and MAS, while the same immunosuppression was driving or sustaining the parasitic infection. Pentavalent antimonials were excluded, given their nephrotoxic and cardiotoxic potential in the setting of active LN. Liposomal amphotericin B (L-AmB) was administered at 3 mg/kg once daily for 5 consecutive days with one repeat dose at Day 10 of treatment (total 6 doses, ~18.5 mg/kg), consistent with recommendations for VL in moderately immunocompromised non-HIV patients.[7]
Following L-AmB alongside prednisolone, MMF, ramipril, and hydroxychloroquine, the fever resolved within days, and hematological parameters, ferritin, and liver enzymes normalized over the following weeks.
Hospital Discharge and Follow-Up. On Day 44 of illness (Day 30 of hospitalization), the patient was discharged on oral prednisolone (1 mg/kg/day), ramipril, hydroxychloroquine, and cotrimoxazole. At discharge laboratory results showed Hb 14.2 g/dL, WBC 9,650/mm³, platelets 195,000/mm³, creatinine 0.7 mg/dL, albumin 4.3 g/dL, and proteinuria 20.4 mg/m²/h.
At Month 5 follow-up, the patient was asymptomatic with cushingoid features. Full blood count was normal (Hb 15 g/dL, WBC 10,700/mm³, platelets 210,000/mm³); creatinine 0.7 mg/dL; proteinuria 10.2 mg/m²/h (≥90% reduction from peak; partial renal response per KDIGO 2024). Albumin normalized (4.7 g/dL); C3/C4 returned to normal; ANA (1/160) and anti-dsDNA (1/20) were markedly reduced; anti-cardiolipin IgG fell to borderline (18 GPL-U). DAT converted to negative and ferritin was 130 ng/mL. Anti-Leishmania IgG ELISA was weakly positive (expected post-treatment seroconversion); peripheral blood and bone marrow PCR were negative. Prednisolone tapering was initiated.
At Month 7, proteinuria was absent (<4 mg/m²/h; complete renal response per KDIGO 2024). Prednisolone, ramipril, and cotrimoxazole were discontinued while MMF was continued. Cushingoid features resolved. At Month 12, C3/C4 were normal, anti-dsDNA and anti-cardiolipin IgG were negative; ANA titers were 1/160, peripheral blood Leishmania PCR was negative, and frontotemporal alopecia had significantly improved.
The timeline of the course of the patient is presented in Table 4 and Figure 2.
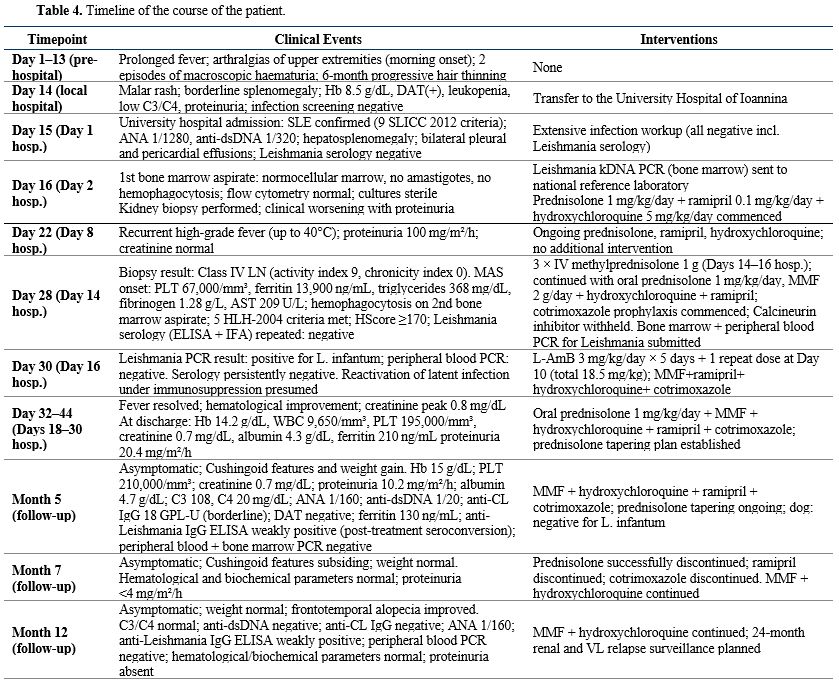 |
Table 4. Timeline of the course of the patient. |
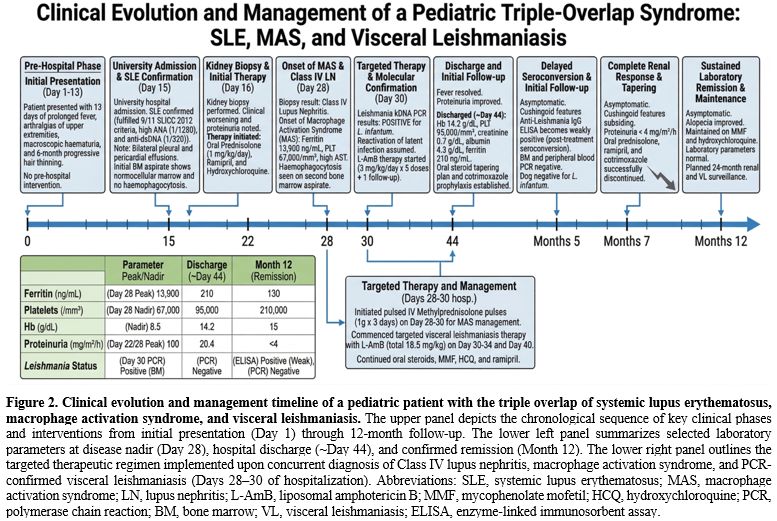 |
Figure 2. Clinical
evolution and management timeline of a pediatric patient with the
triple overlap of systemic lupus erythematosus, macrophage activation
syndrome, and visceral leishmaniasis. The upper panel depicts
the chronological sequence of key clinical phases and interventions
from initial presentation (Day 1) through 12-month follow-up. The lower
left panel summarizes selected laboratory parameters at disease nadir
(Day 28), hospital discharge (~Day 44), and confirmed remission (Month
12). The lower right panel outlines the targeted therapeutic regimen
implemented upon concurrent diagnosis of Class IV lupus nephritis,
macrophage activation syndrome, and PCR-confirmed visceral
leishmaniasis (Days 28–30 of hospitalization). Abbreviations: SLE,
systemic lupus erythematosus; MAS, macrophage activation syndrome; LN,
lupus nephritis; L-AmB, liposomal amphotericin B; MMF, mycophenolate
mofetil; HCQ, hydroxychloroquine; PCR, polymerase chain reaction; BM,
bone marrow; VL, visceral leishmaniasis; ELISA, enzyme-linked
immunosorbent assay. |
Discussion
Context and Novelty. The simultaneous occurrence of severe SLE with Class IV lupus nephritis, MAS, and VL in a single pediatric patient is exceptionally rare. To our knowledge, prior reports of this simultaneous triad in a pediatric patient are scarce; the available literature includes only dyadic combinations: Costa et al.[8] reported VL-triggered MAS in an adult lupus patient, and Higel et al.[9] described VL presenting as a lupus-like syndrome complicated by MAS in a child. The present case appears to be among the first in which all three conditions were documented simultaneously by biopsy, clinical criteria, and molecular diagnostics in an adolescent, although under-reporting and ascertainment bias should be acknowledged.Diagnostic Challenges: Overlapping Phenotype of SLE, MAS, and VL. The principal diagnostic challenge in this case arose from the profound phenotypic overlap between the three conditions. All three share fever, hepatosplenomegaly, cytopenias, hyperferritinemia, and autoantibody positivity.[10,11] The SLE diagnosis in our patient was well established (9 SLICC criteria, Class IV LN). The anti-cardiolipin antibodies may partly reflect Leishmania-induced polyclonal B-cell activation rather than true primary antiphospholipid syndrome; this is supported by their subsequent disappearance at 12-month follow-up.
An important additional complexity deserves emphasis: VL alone can produce a complete lupus-like syndrome - including ANA, anti-dsDNA, hypocomplementemia and cytopenias - through polyclonal B-cell activation and immune complex deposition, without true underlying SLE.[12] Critically, several infections, including Leishmania and Treponema pallidum, have been reported to induce a full-house immunofluorescence pattern on renal biopsy indistinguishable from lupus nephritis.[13,14] In view of these mimicry potentials, we have sought to distinguish what is documented from what is inferred or speculative in this case. Documented findings include fulfilment of nine SLICC criteria, biopsy-proven Class IV proliferative lupus nephritis with active lesions, PCR-confirmed Leishmania infantum on bone marrow with subsequent seroconversion at Month 5, and fulfilment of HLH-2004 criteria for MAS. Strongly supported but inferential is the conclusion that genuine SLE coexisted with VL rather than VL alone simulating lupus; this is supported principally by the persistence of clinical and serological disease activity beyond parasite clearance and by sustained remission requiring continued immunosuppression. Speculative - and framed accordingly - is whether VL specifically triggered SLE in a susceptible host, whether the two diseases arose independently, or whether VL exacerbated subclinical autoimmunity; with the available data, we cannot adjudicate between these possibilities, although the close temporal relationship between VL reactivation and MAS onset is consistent with the first interpretation.
MAS Precipitants and Differential Diagnosis of Secondary HLH. The emergence of MAS fulfilled 5/8 HLH-2004 criteria,[3] with an HScore ≥170 (>93% probability of reactive HLH).[4] VL reactivated under immunosuppression was considered the most plausible MAS trigger, as Leishmania impairs NK-cell and cytotoxic T-lymphocyte surveillance, directly driving the hyperinflammatory cascade.[15,16] Although primary (genetic) HLH can present in adolescence and may be unmasked by infection or autoimmune disease,[3] the clinical picture favored secondary MAS with SLE (Class IV LN) and Leishmania infantum infection as plausible precipitants. Leishmania is among the most common protozoan triggers of HLH/MAS;[10] a recent systematic review identified 135 pediatric VL-related HLH cases.[17]
Genetic HLH was not performed, which is a limitation of this case. The 2022 EULAR/ACR guidance recommends genetic HLH investigation in patients with severe MAS who fail conventional therapy, and genetic testing is recommended if MAS recurs.[18]
Seronegative VL in Immunocompromised Hosts: The Critical Role of Bone Marrow PCR. A critical teaching point of this case was the persistently negative Leishmania serology at initial presentation, despite VL being confirmed by bone marrow PCR, with seroconversion occurring only on Month 5. This is well explained by impaired humoral response during active immunosuppression. Piarroux et al. demonstrated 82% PCR sensitivity versus only 55% for microscopy in immunocompromised patients.[5] The rK39 rapid test, with 90–100% sensitivity in immunocompetent Mediterranean hosts, has a markedly reduced sensitivity of 40–60% in immunocompromised individuals.[19] Bone marrow PCR achieves approximately 90–95% sensitivity in immunocompromised outperforming microscopy and peripheral blood PCR,[5,6] providing a strong rationale for bone marrow sampling without awaiting serological confirmation.
In the broader pediatric VL-related HLH literature, seronegative confirmed VL is well documented. Chen et al.[17] identified cases where serological testing was entirely negative, and diagnosis relied exclusively on bone marrow microscopy or PCR. Van Griensven et al. estimated that up to 30–40% of VL cases in immunocompromised non-HIV patients may be seronegative.[20] These data support a PCR-based diagnostic approach that prioritizes bone marrow testing in immunosuppressed patients with unexplained fever in endemic areas, regardless of serology.
Immunosuppressive Strategy: MMF versus Cyclophosphamide. MMF was chosen over intravenous cyclophosphamide. Pivotal randomized controlled trials[21,22] demonstrated equivalent or superior MMF efficacy for LN induction, with a more favorable toxicity profile. The compelling argument for MMF in this patient was avoidance of gonad toxicity with pediatric data supporting equivalent renal outcomes[23] and KDIGO 2024 recommending MMF as the preferred induction agent where gonad toxicity is a concern.[24] A calcineurin inhibitor was deliberately withheld despite KDIGO 2024 triple-therapy recommendations, due to concerns about impaired T-cell–mediated immunity and the risk of Leishmania dissemination in the setting of active intracellular infection.[8]
MAS Management in the Setting of Active Infection. High-dose glucocorticoids remain the cornerstone of MAS therapy; the 2025 METAPHOR systematic review[25] found methylprednisolone reported in virtually all MAS cases. Cyclosporine was withheld due to the risk of exacerbating intracellular infection. Current guidance emphasizes prioritizing treatment of the underlying infection alongside control of hyperinflammation. The 2022 EULAR/ACR guidance emphasizes that infection-driven MAS requires treatment of the infectious cause as a priority alongside anti-hyperinflammatory therapy.[18]
Biologic second-line options merit discussion. Anakinra (IL-1 receptor antagonist) has been used successfully in SLE-associated MAS refractory to steroids, with a more favorable infection-risk profile than cyclosporine.[26] Emapalumab (an anti-interferon-γ monoclonal antibody) has emerging evidence for use in secondary HLH/MAS.[27] Neither was required in our patient given the rapid response to steroids and L-AmB. In future cases of VL-driven MAS refractory to steroids where cyclosporine is contraindicated, anakinra would be the preferred second-line agent given its shorter half-life and compatibility with concurrent anti-infective therapy.
Antileishmanial Therapy: Choice and Dosing of Liposomal Amphotericin B. Pentavalent antimonials were excluded, given nephrotoxic and cardiotoxic risk in the setting of active glomerulonephritis. L-AmB is the treatment of choice for VL in Europe and specifically recommended for immunocompromised patients.[10] In immunocompetent Mediterranean patients, a total dose of 18–21 mg/kg achieves high cure rates,[28] whereas guidelines recommend higher cumulative doses (up to 40 mg/kg) in severe immunosuppression due to the risk of relapse.[29] Our patient received approximately 18.5 mg/kg, appropriate for moderate immunosuppression with preserved renal function; Leishmania PCR remained negative at 3, 5, and 12 months.
Infection Prophylaxis. Cotrimoxazole prophylaxis was initiated simultaneously with high-dose corticosteroid pulses and MMF, consistent with pediatric rheumatology guidelines recommending Pneumocystis jirovecii prophylaxis during combined immunosuppression that exceeds prednisolone 20 mg/day for more than 4 weeks.[24] No other antimicrobial prophylaxis was administered during acute admission.
Conclusions
Despite the life-threatening presentation with proliferative lupus nephritis, macrophage activation syndrome and PCR-confirmed visceral leishmaniasis, this patient achieved sustained clinical remission at 12 months. Disease activity markedly improved from a highly active baseline to low activity with complete renal response according to KDIGO 2024 criteria by Month 7; hematological and complement parameters normalized, Leishmania PCR remained persistently negative and corticosteroids were successfully tapered. Maintenance therapy with MMF and hydroxychloroquine was sufficient to sustain remission.Although conclusions from a single case must be interpreted cautiously, this case highlights key clinical considerations for immunosuppressed SLE patients in endemic regions. Negative serology does not exclude VL in immunocompromised hosts; early PCR testing should be pursued when hepatosplenomegaly, cytopenias, or MAS are present. Infectious triggers should be excluded before immunosuppressive escalation, and L-AmB remains the preferred therapy when concomitant nephritis is present. Early molecular diagnosis and coordinated pathogen-directed and immunomodulatory therapy are essential to achieve durable recovery in complex autoimmune–infectious overlap syndromes.
The case also demonstrates that, with timely diagnosis, simultaneous and carefully tailored immunosuppressive and antiparasitic therapy sustained remission can be achieved in this life-threatening overlap syndrome.
Practical Teaching Points
1. In a known SLE patient receiving immunosuppression, persistent or recurrent fever should prompt early reassessment for occult infection rather than reflex escalation of immunosuppressive therapy.2. Macrophage activation syndrome should be considered not only as a complication of active autoimmune disease but also as a potential herald of an underlying infection, particularly in patients from areas endemic for visceral pathogens.
3. A negative Leishmania serology does not exclude visceral leishmaniasis in immunocompromised hosts; rK39 and conventional serological assays show markedly reduced sensitivity (approximately 40–60%) under iatrogenic or disease-related immunosuppression.
4. Bone marrow PCR is the most reliable diagnostic test for suspected VL in immunocompromised patients (sensitivity ≈90–95%) and should be pursued without awaiting serological confirmation when clinical suspicion is high.
5. In autoimmune - infectious overlap syndromes, therapy must balance control of hyperinflammation with prioritised treatment of the underlying infection; agents that further impair intracellular pathogen control (in particular calcineurin inhibitors) should be avoided where reasonable alternatives exist (e.g., mycophenolate mofetil for lupus nephritis induction, anakinra as a second-line agent for refractory MAS).
Abbreviations
ANA: Antinuclear
antibody; ANC: Absolute neutrophil count; CNI: Calcineurin inhibitor; CRP:
C-reactive protein; DAT: Direct antiglobulin test; ELISA: Enzyme-linked
immunosorbent assay; ESR: Erythrocyte sedimentation rate; HLH: Hemophagocytic
lymphohistiocytosis; HPF: High-power field; IFA: Indirect immunofluorescence
assay; ISN/RPS: International Society of Nephrology/Renal Pathology Society;
KDIGO: Kidney Disease: Improving Global Outcomes; L-AmB: Liposomal amphotericin
B; LN: Lupus nephritis; MAS: Macrophage activation syndrome; MMF: Mycophenolate
mofetil; PCR: Polymerase chain reaction; SLE: Systemic lupus erythematosus;
SLICC: Systemic Lupus International Collaborating Clinics Classification; VL:
Visceral leishmaniasis; WBC: White blood cell; EULAR/ACR: European Alliance of
Associations for Rheumatology / American College of Rheumatology; BM: Bone
marrow; CMV: Cytomegalovirus; EBV: Epstein–Barr virus; Hb: Haemoglobin; HCQ:
Hydroxychloroquine; HIV: Human immunodeficiency virus; HScore: Hemophagocytic
syndrome diagnostic score; HSV: Herpes simplex virus; IL-1: Interleukin-1; LDH:
Lactate dehydrogenase; MCV: Mean corpuscular volume; NK: Natural killer (cell);
aPTT: activated partial thromboplastin time; sCD25: soluble CD25 (interleukin-2
receptor α chain).
References
- Petri M, Orbai AM, Alarcon GS, et al. Derivation
and validation of the Systemic Lupus International Collaborating
Clinics classification criteria for systemic lupus erythematosus.
Arthritis Rheum 2012;64:2677-2686. https://doi.org/10.1002/art.34473 PMid:22553077 PMCid:PMC3409311
- Weening
JJ, D'Agati VD, Schwartz MM, et al. The classification of
glomerulonephritis in systemic lupus erythematosus revisited. J Am Soc
Nephrol 2004;15:241-250. https://doi.org/10.1097/01.ASN.0000108969.21691.5D PMid:14747370 PMCid:PMC11265893
- Henter
JI, Horne A, Arico M, et al. HLH-2004: Diagnostic and therapeutic
guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer
2007;48:124-131. https://doi.org/10.1002/pbc.21039 PMid:16937360
- Fardet
L, Galicier L, Lambotte O, et al. Development and validation of the
HScore, a score for the diagnosis of reactive hemophagocytic syndrome.
Arthritis Rheumatol 2014;66:2613-2620. https://doi.org/10.1002/art.38690 PMid:24782338 PMCid:PMC9548873
- Piarroux
R, Gambarelli F, Dumon H, et al. Comparison of PCR with direct
examination of bone marrow aspiration, myeloculture, and serology for
diagnosis of visceral Leishmaniasis in immunocompromised patients. J
Clin Microbiol 1994;32:746-749. https://doi.org/10.1128/jcm.32.3.746-749.1994 PMid:8195388 PMCid:PMC263118
- Antinori
S, Calattini S, Longhi E, et al. Clinical use of polymerase chain
reaction performed on peripheral blood and bone marrow samples for the
diagnosis and monitoring of visceral leishmaniasis in HIV-infected and
HIV-uninfected patients. Clin Infect Dis 2007;44:1602-1610. https://doi.org/10.1086/518167 PMid:17516404
- WHO. Report of a WHO informal consultation on liposomal amphotericin B in the treatment of visceral leishmaniasis. 2005.
- Costa
A, Pais C, Cerqueira S, Salvador F. Visceral Leishmaniasis Associated
with Macrophage Activation Syndrome and Diffuse Alveolar Hemorrhage in
a Lupus Patient. Acta Med Port 2018;31:593-596. https://doi.org/10.20344/amp.9028 PMid:30387429
- Higel
L, Froehlich C, Pages MP, et al. Macrophage activation syndrome and
autoimmunity due to visceral leishmaniasis. Arch Pediatr
2015;22:397-400. https://doi.org/10.1016/j.arcped.2014.11.025 PMid:25617995
- Mantadakis
E, Alexiadou S, Totikidis G, Grapsa A, Chatzimichael A. A Brief Report
and Mini-Review of Visceral Leishmaniasis-associated Hemophagocytic
Lymphohistiocytosis in Children. J Pediatr Hematol Oncol
2021;43:e223-e226. https://doi.org/10.1097/MPH.0000000000001747 PMid:32049769
- Avar-Aydin PO, Brunner HI. Revisiting Childhood-Onset Systemic Lupus Erythematosus. Turk Arch Pediatr 2024;59:336-344. https://doi.org/10.5152/TurkArchPediatr.2024.24097 PMid:39102578 PMCid:PMC11332533
- Santana
IU, Dias B, Nunes EA, et al. Visceral leishmaniasis mimicking systemic
lupus erythematosus: Case series and a systematic literature review.
Semin Arthritis Rheum 2015;44:658-665. https://doi.org/10.1016/j.semarthrit.2014.12.004 PMid:25704907
- Scaperotti
MM, Kwon D, Kallakury BV, Steen V. Not all that is 'full house' is
systemic lupus erythematosus: a case of membranous nephropathy due to
syphilis infection. BMJ Case Rep 2021;14. https://doi.org/10.1136/bcr-2021-244466 PMid:34413046 PMCid:PMC8378353
- Jaunin
E, Kissling S, Rotman S, Waeber G, Halfon M. Syphilis and parvovirus
B19 co-infection imitating a lupus nephropathy: A case report. Medicine
(Baltimore) 2019;98:e17040. https://doi.org/10.1097/MD.0000000000017040 PMid:31490394 PMCid:PMC6739001
- Mouhoub
B, Bensalah M, Berhili A, et al. Visceral leishmaniasis associated with
macrophage activation syndrome: Case report and literature review.
IDCases 2021;26:e01247. https://doi.org/10.1016/j.idcr.2021.e01247 PMid:34430207 PMCid:PMC8371194
- Scalzone
M, Ruggiero A, Mastrangelo S, et al. Hemophagocytic lymphohistiocytosis
and visceral leishmaniasis in children: case report and systematic
review of literature. J Infect Dev Ctries 2016;10:103-108. https://doi.org/10.3855/jidc.6385 PMid:26829545
- Chen
Z, Gao Y, Zhang C, Mao J. Hemophagocytic lymphohistiocytosis secondary
to visceral leishmaniasis in children: case report and systematic
review. Front Pediatr 2025;13:1561600. https://doi.org/10.3389/fped.2025.1561600 PMid:40292113 PMCid:PMC12021907
- Shakoory
B, Geerlinks A, Wilejto M, et al. The 2022 EULAR/ACR points to consider
at the early stages of diagnosis and management of suspected
haemophagocytic lymphohistiocytosis/macrophage activation syndrome
(HLH/MAS). Ann Rheum Dis 2023;82:1271-1285. https://doi.org/10.1136/ard-2023-224123 PMid:37487610 PMCid:PMC11017727
- Humbert
MV, Costa LE, Katis I, et al. A rapid diagnostic test for human
Visceral Leishmaniasis using novel Leishmania antigens in a Laser
Direct-Write Lateral Flow Device. Emerg Microbes Infect
2019;8:1178-1185. https://doi.org/10.1080/22221751.2019.1635430 PMid:31381478 PMCid:PMC6713177
- van
Griensven J, Carrillo E, Lopez-Velez R, Lynen L, Moreno J.
Leishmaniasis in immunosuppressed individuals. Clin Microbiol Infect
2014;20:286-299. https://doi.org/10.1111/1469-0691.12556 PMid:24450618
- Ginzler
EM, Dooley MA, Aranow C, et al. Mycophenolate mofetil or intravenous
cyclophosphamide for lupus nephritis. N Engl J Med 2005;353:2219-2228. https://doi.org/10.1056/NEJMoa043731 PMid:16306519
- Appel
GB, Contreras G, Dooley MA, et al. Mycophenolate mofetil versus
cyclophosphamide for induction treatment of lupus nephritis. J Am Soc
Nephrol 2009;20:1103-1112. https://doi.org/10.1681/ASN.2008101028 PMid:19369404 PMCid:PMC2678035
- Chbihi
M, Eveillard LA, Riller Q, et al. Induction therapy for pediatric onset
class IV lupus nephritis: Mycophenolate Mofetil versus
Cyclophosphamide. J Nephrol 2023;36:829-839. https://doi.org/10.1007/s40620-022-01438-2 PMid:36208405
- Rovin
BH, Ayoub IM, Chan TM, et al. Executive summary of the KDIGO 2024
Clinical Practice Guideline for the Management of Lupus Nephritis.
Kidney Int 2024;105:31-34. https://doi.org/10.1016/j.kint.2023.09.001 PMid:38182299
- Baldo
F, Erkens RGA, Mizuta M, et al. Current treatment in macrophage
activation syndrome worldwide: a systematic literature review to inform
the METAPHOR project. Rheumatology (Oxford) 2025;64:32-44. https://doi.org/10.1093/rheumatology/keae391 PMid:39058514 PMCid:PMC11701305
- Lee
J, Bae KS, Rhim JW, Lee SY, Jeong DC, Kang JH. Macrophage Activation
Syndrome in Children: Update on Diagnosis and Treatment. Children
(Basel) 2024;11. https://doi.org/10.3390/children11070755 PMid:39062205 PMCid:PMC11274371
- De
Benedetti F, Grom AA, Brogan PA, et al. Efficacy and safety of
emapalumab in macrophage activation syndrome. Ann Rheum Dis
2023;82:857-865. https://doi.org/10.1136/ard-2022-223739 PMid:37001971 PMCid:PMC10314091
- Davidson
RN, Di Martino L, Gradoni L, et al. Liposomal amphotericin B (AmBisome)
in Mediterranean visceral leishmaniasis: a multi-centre trial. Q J Med
1994;87:75-81.
- Burza S, Croft SL, Boelaert M. Leishmaniasis. Lancet 2018;392:951-970. https://doi.org/10.1016/S0140-6736(18)31204-2 PMid:30126638 PMCid:PMC8757988