Epstein-Barr virus (EBV) infection is causally associated with 25–40% of classical HL cases, particularly among older individuals and those with a personal history of autoimmune disease or immunodeficiency.[2] A significantly increased standardized incidence ratio (SIR) for HL has been reported in several autoimmune diseases, including autoimmune hemolytic anemia, sarcoidosis, systemic lupus erythematosus, immune thrombocytopenic purpura, polyarteritis nodosa, polymyositis/dermatomyositis, Behcet's disease, Sjögren's syndrome, rheumatoid arthritis, polymyalgia rheumatica, and psoriasis.[3] The incidence of HL is 5- to 25-fold higher in people living with HIV (PLWH) and in other immunodeficient conditions, and HL in these populations is almost universally EBV-positive.[4] Although the incidence of HL is increased in PLWH, HL is not considered an acquired immunodeficiency syndrome (AIDS)-defining malignancy and is usually treated as in immunocompetent patients. Currently, evidence supporting a role for other specific environmental risk factors is limited.[2] Registry-based studies have shown that the risk of HL in first-degree relatives of affected individuals ranges from 1.2- to 5.8-fold, with a stronger association observed among siblings than between parents and offspring. Several genome-wide association studies (GWASs) have shown that the risk of HL is strongly influenced by variation in the human leukocyte antigen (HLA) genotype as well as by non-HLA genotype variation.[5,6] In rare cases, HL can arise from the transformation of an underlying low-grade B-cell lymphoma, mostly chronic lymphocytic leukemia, as “Hodgkin-like Richter transformation”.[7,8]
Biology and histopathological subtypes
Classical HL (cHL) originates form the neoplastic transformation of germinal center B-cells and is characterized by a paucity of tumor cells within an abundant immunosuppressive microenvironment. The diagnostic Hodgkin/Reed-Sternberg (HRS) cells are large, atypical cells with a defective B-cell program. They lack expression of the B-cell receptor and characteristically express CD30 (100% of cells), CD15 (75–80%), and weakly PAX5 (95%).[7,8] The B cell antigen CD20 can be expressed in up to 20% of cases. HRS cells actively interact with the surrounding microenvironment and create a supportive network of reactive immune cells, which promote cellular proliferation and inhibit apoptosis. Constitutively expressed NF-κB transcription factor, along with clonal EBV infection in a subset of cases, contribute to HRS cell survival and proliferation. Moreover, HRS cells evade antitumor immune responses through multiple mechanisms including expression of PD-1 ligands PD-L1 and PD-L2, often driven by copy-number alterations of chromosome 9p24.1 (Figure 1).[9]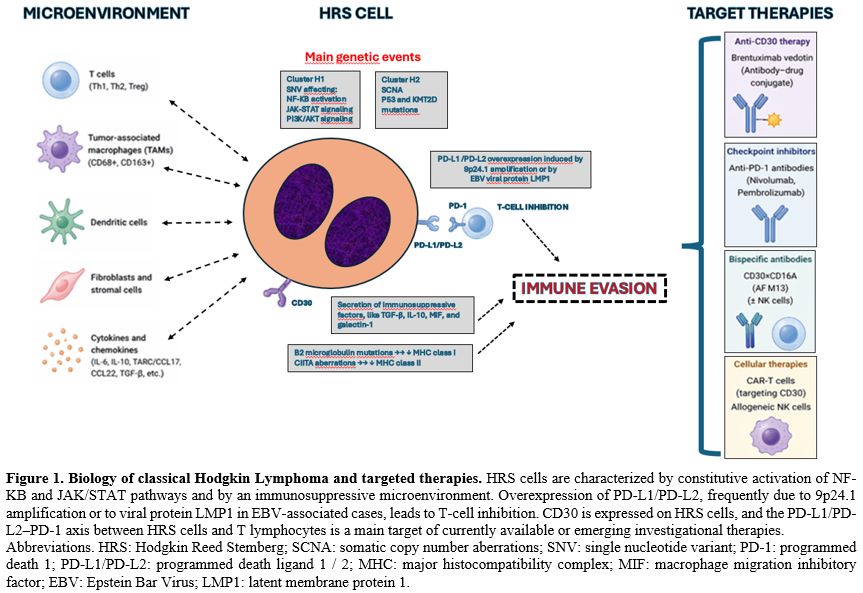 |
|
Although the relative paucity of malignant cells within cHL tumors has historically hampered its molecular profiling, liquid biopsies have helped to overcome this limitation by enabling noninvasive cHL genotyping.[10-12] Tumor-derived cHL mutations are often enriched in circulating cell-free DNA in blood plasma compared with corresponding bulk tumor specimens. Molecular profiling of liquid biopsies identified recurrent somatic mutations in at least 41 genes as well as recurrent amplifications and deletions. Moreover, two distinct molecular clusters have been described: cluster H1, accounting for approximately 68% of cases, is more common in in younger patients, and is characterized by a higher somatic single nucleotide variant (SNV) mutational burden with enrichment of mutations affecting key signaling pathways, including NF-kB, JAK/STAT, and PI3K. In contrast, cluster H2 tumors representing about 32% of cases, is characterized by a variety of somatic copy number alterations (SCNA) as well as mutations in TP53 and KMT2D (Figure 1). This subgroup shows the typical bimodal age distribution, is enriched for EBV-positive tumors and the mixed cellularity subtype and is associated with higher ctDNA levels and inferior clinical outcomes.[11]
The WHO-HAEM5 and the International Consensus Classification (ICC) retain the histological subtypes of cHL and their diagnostic criteria, which remain unchanged from the WHO-HAEM4: nodular sclerosis (NSCHL), mixed cellularity (MCCHL), lymphocyte-rich (LRCHL), and lymphocyte-depleted (LDCHL). Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL) differs biologically and morphologically from cHL, as it lacks HRS cells and is instead characterized by a neoplastic population of larger CD20+, CD30- cells with folded lobulated nuclei known as lymphocytic and histiocytic (L&H) cells. The WHO-HAEM5 continues to list NLPHL under the family of HL, while the ICC changed the term NLPHL into “Nodular Lymphocyte Predominant B-Cell Lymphoma”, since the neoplastic cells conserve a functional B-cell program and show a closer relationship to T-cell/histiocyte-rich large B-cell lymphoma than to cHL.[7,8]
Clinical presentation, staging, and prognosis
HL patients usually present with painless superficial lymphadenopathy, most commonly involving the cervical and supraclavicular sites. Mediastinal involvement occurs in 60% of patients, with 20-25% having mediastinal bulk disease associated with symptoms such as cough, shortness of breath, or even superior vena cava syndrome. Advanced stages occur in 40% cases with extranodal site involvement, including lung (21%), bone (15%), liver (10%), and bone marrow (9%). Other types of extranodal involvement are uncommon. B-symptoms, such as fevers, drenching night sweats, or unintentional weight loss, occur in 40% of patients, approximately in 20% of patients with localized disease and 70% with advanced-stage disease. Pruritus sine materia can be a presenting symptom in classical HL.According to the Lugano recommendations, fluorodeoxyglucose (FDG) positron emission tomography (PET)–computed tomography (CT) is the preferred staging modality, given its higher accuracy than CT scanning for both nodal and extranodal disease, upstaging the disease in up to 41% of patients and downstaging in up to 10% of patients. However, contrast-enhanced computed tomography (CE-CT) is still useful in the setting of compression or thrombosis of mediastinal vessels and for radiation planning. PET-CT has high sensitivity in detecting bone involvement in patients with HL, therefore eliminating the need for bone marrow biopsy in most cases.[13]
Routine prognostic scores at the diagnosis, including both clinical, imaging and laboratory parameters, differ between early stages (the European Organization for Research and Treatment of Cancer (EORTC) and the German Hodgkin Study Group (GHSG) prognostic systems), and advanced stages (International Prognostic Score (IPS)). The major difference between the EORTC and GHSG classification systems concerns the advanced stage, for which the GHSG system includes stage IIB disease with either bulky mediastinal or extranodal disease alongside stage III/IV diseases (Table 1-2).[14,15]
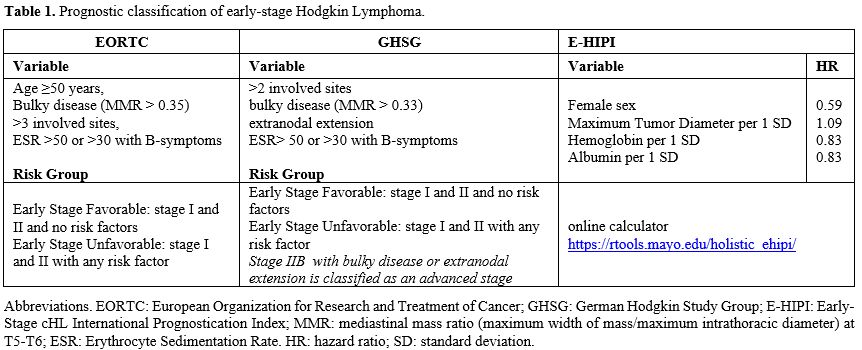 |
Table 1. Prognostic classification of early-stage Hodgkin Lymphoma. |
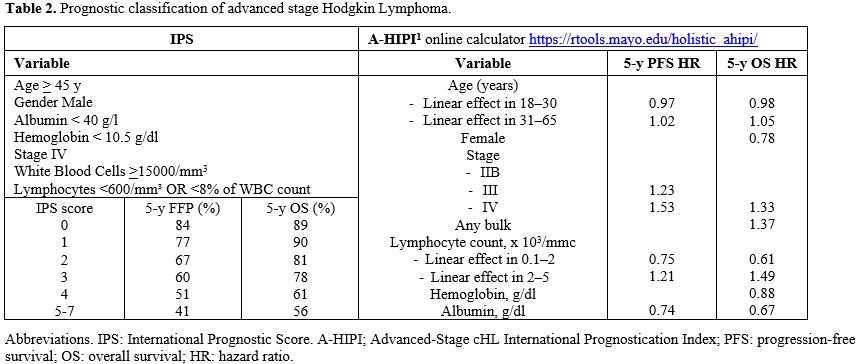 |
Table 2. Prognostic classification of advanced stage Hodgkin Lymphoma. |
Using the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) guidelines, the Holistic Consortium developed novel prognostic scoring systems for both early (E-HIPI) and advanced (A-HIPI) stages of cHL. These models include continuous variables and provide improved prognostic accuracy compared with traditional prognostication systems (Table 1-2).[16,17]
Early PET evaluation after the first cycles of chemotherapy, assessed according to the Deauville criteria, has been established as a robust prognostic factor. It is now widely used to guide subsequent treatment de-escalation or intensification, and, over the past decade, most pivotal clinical trials in cHL have incorporated interim PET assessment.[18-20]
Baseline metabolic tumor volume (MTV) has also been shown to influence the risk of relapses in cHL, with the risk increasing by approximately 19 to 21% for each additional cm increase in baseline tumor size. Importantly, MTV provides prognostic information independent of PET‐2 results.[21-23] However, several methods are currently used to measure MTV, and standardization is required before its routine integration into clinical practice.[24]
Pretreatment plasma ctDNA has emerged as an important prognostic biomarker showing a strong correlation with total MTV, with higher levels associated with inferior PFS.[11] Dynamic assessment of ctDNA during therapy represents a promising, radiation-free tool for tracking residual disease and identifying clonal evolution in cHL. It may complement PET imaging for the early identification of chemorefractory patients, to distinguish ambiguous PET-positive lesions after treatment, and to detect radiographically occult minimal residual disease.[11-13]
Finally, several tumor microenvironment-related parameters have been associated with poorer outcomes, including the proportion of tumor-infiltrating CD68+ macrophages greater than 5%, and elevated plasma levels of thymus and activation‐regulated chemokine (TARC) and Interleukin-10 (IL10).[25-27]
Treatment
Treatment modalities for patients with Hodgkin lymphoma vary according to disease stage (early versus advanced), prognostic factors (favorable versus unfavorable), age (children versus young-adult and elderly), patient comorbidities and, importantly, national guidelines and healthcare reimbursement policy.[14,28,29]Over the past decade, the treatment landscape of cHL has evolved significantly with the adoption of PET-guided strategies and the integration of novel targeted agents modifying conventional chemotherapy regimens, such as ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) and BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone). These newer agents have, in part, replaced more toxic components of traditional therapies. The key agents of this change include the antibody-drug conjugate BV, which consists of a chimeric anti-CD30 monoclonal antibody carrying the microtubule-disrupting agent monomethyl auristatin E (MMAE) as a payload, and the anti-PD1 checkpoint inhibitors nivolumab and pembrolizumab, which enhance the antitumor immune response. Initially approved as monotherapy for relapsed/refractory disease, these agents are increasingly being incorporated into earlier lines of treatment.[30-32] These novel frontline chemo/immunotherapy combinations resulted in higher response rates and longer durations compared to historical regimens. In this evolving therapeutic landscape, the role of consolidative radiotherapy remains an area of ongoing investigation.
For the purposes of this review, we will discuss the treatment of young adult and elderly patients with cHL separately.
Treatmnt of Favorable Early-Stage HL
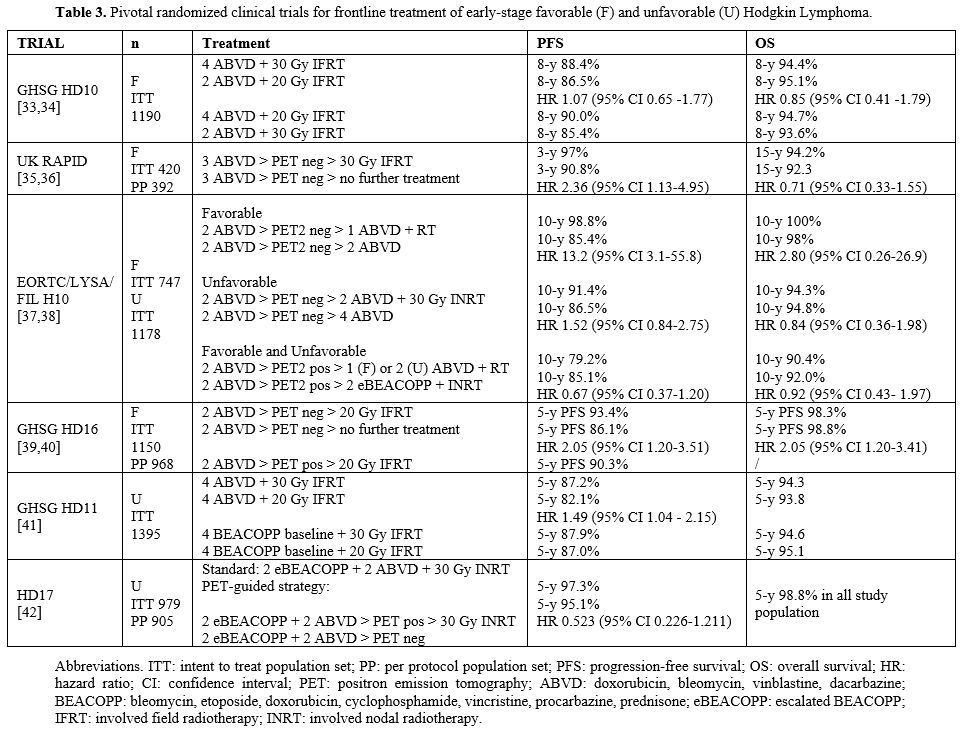
Current guidelines recommend two cycles of ABVD followed by involved nodal/involved site radiotherapy (INRT/ISRT) as the preferred treatment approach for patients with early-stage cHL without risk factors, according to the GHSG risk stratification system.[29] This approach was validated by the GHSG HD10 clinical trial, which randomized 1190 patients with newly diagnosed favorable early-stage cHL to two or four cycles of ABVD, followed by 20 Gy or 30 Gy involved-field radiotherapy (IFRT).[33] Ten-year PFS and OS were 87% and 94%, respectively, both in those treated with two cycles of ABVD followed by 20 Gy IFRT and those treated with four cycles of ABVD followed both by 30 Gy IFRT, confirming the non-inferiority of reduced intensity combined modality treatment (CMT) in this patient population.[34]Several studies have subsequently explored the omission of radiotherapy in patients with favorable early-stage HL achieving a negative early PET (Table 3).
 |
|
In the RAPID trial, 392 patients with favorable early-stage HL and a negative PET after three cycles of ABVD were randomized to receive either 30 Gy IFRT or no further treatment. The 3-year PFS was 94.6% in the radiotherapy group and 90.8% in the group that received no further therapy, therefore the study failed to demonstrate the non-inferiority of the strategy of no further treatment after chemotherapy.[35] However, no differences in long term OS were observed.[36]
Similarly, the EORTC/LYSA/FIL H10F trial randomized 747 patients with favorable early-stage HL to either a standard arm consisting of three ABVD followed by INRT or a PET-guided experimental arm. In the experimental arm, PET2-negative patients after two ABVD cycles continued with two additional cycles for a total of four ABVD, whereas PET2-positive patients switched to escalated BEACOPP (eBEACOPP), receiving a total of two ABVD cycles, two eBEACOPP cycles, and INRT.[37] At 10 years of follow-up, among PET2-negative patients, the PFS rate was significantly higher with the combined treatment modality (98.8%) than with chemotherapy alone (85.4%). In the PET2-positive group, the difference in PFS between standard ABVD and intensified eBEACOPP was no longer statistically significant.[38]
Similarly, the GHSG HD16 trial reported a 5-year PFS of 93.4% in PET2 negative patients with favorable early-stage HL receiving IFRT after two cycles ABVD versus 86.1% in PET2 negative patients who did not receive further treatment after chemotherapy.[39,40]
Collectively, the RAPID, EORTC H10, and GHSG HD16 trials failed to demonstrate non-inferiority of PET-adapted omission of radiotherapy with respect to PFS compared with CMT in patients with favorable early-stage cHL. However, no significant differences in OS were observed in early PET negative patients not receiving radiotherapy. Omission of radiotherapy may reduce long-term toxicities including the risk of secondary primary neoplasms. Consequently, in real-world clinical practice, many clinicians favor a chemotherapy-only approach for selected patients with early-stage cHL, accepting a modest reduction in PFS in the light of the availability of effective savage treatments capable of achieving durable remissions in most relapsed patients.
Treatment of Early-Stage Unfavorable HL
Current guidelines recommend four cycles of ABVD followed by 30 Gy INRT/ISRT as the preferred treatment approach for patients with unfavorable early-stage cHL.[29] Key randomized clinical trials evaluating frontline treatment in this setting are summarized in Table 3.In the GHSG HD11 trial, four cycles of ABVD, followed by 30 Gy IFRT, were not inferior to four cycles of baseline BEACOPP, followed by 20 or 30 Gy IFRT. In contrast, treatment consisting of four cycles of ABVD followed by 20 Gy IFRT was associated with inferior PFS in this not-PET-guided approach.[41]
In the PET-guided EORTC/LYSA/FIL H10U trial, four cycles of ABVD followed by INRT resulted in a higher PFS than the experimental arm, which received 6 cycles of ABVD, in early PET-negative patients; however, this difference was modest and not statistically significant. At 10-year follow-up analysis, there was no statistically significant difference in PFS between PET2-positive patients after two ABVD cycles who continued standard therapy (two cycles of ABVD followed by 30 Gy INRT) and those who received an intensified approach consisting of two cycles of eBEACOPP followed by 30 Gy INRT.[37,38]
In GHSG HD17 trial, the omission of INRT in patients with unfavorable early‐stage cHL who achieved a negative PET after two cycles of eBEACOPP and continued with two cycles of ABVD was not inferior to standard CMT consisting of the same chemotherapy induction followed by 30 Gy INRT.[42]
Overall, these studies suggest that when more intensive upfront chemotherapy is administered such as six cycles of ABVD or intensified therapy with eBEACOPP, the additional benefit of consolidative radiotherapy in terms of PFS may be limited or absent.
New agent combinations in early stage cHL
Several phase II clinical trials have investigated the incorporation of novel monoclonal antibodies into frontline regimens for early stage cHL(Table 4).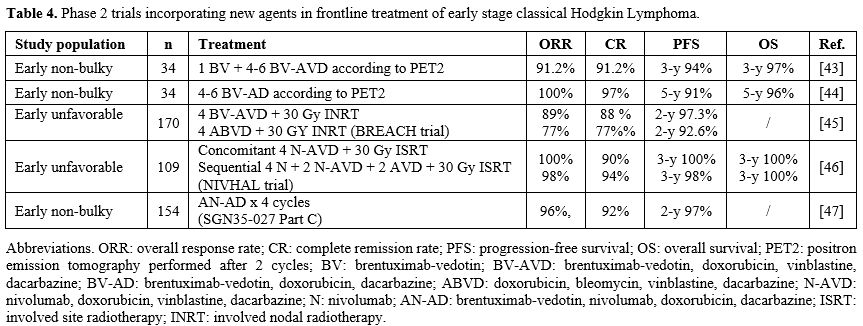 |
|
In the RAPID trial, 392 patients with favorable early-stage HL and a negative PET after three cycles of ABVD were randomized to receive either 30 Gy IFR
The addition of BV to doxorubicin, vinblastine and dacarbazine (AVD) for 4-6 cycles, guided by PET2 evaluation, while omitting both bleomycin and consolidative radiotherapy, resulted in a high response rate and a 3-year PFS of 94%. However, this approach was associated with a higher incidence of grade > 3 febrile neutropenia (35%) and peripheral sensory neuropathy (24%).[43] To reduce the overlapping toxicity of BV and vinblastine, BV was combined with doxorubicin and dacarbazine alone (BV-AD) in 34 patients with non-bulky limited-stage cHL. Treatment duration (4 or 6 cycles) was guided by interim PET. ORR and CR were 100% and 97%, respectively, and 5-year PFS was 91%. No cases of febrile neutropenia, grade >3, or peripheral sensory neuropathy were reported.[44]
The multicenter, randomized, open-label, phase II BREACH trial enrolled 170 patients with early-unfavorable cHL and compared 4 cycles of BV-AVD or standard ABVD, both followed by 30 Gy INRT. PET2-negativity was achieved in 82.3% of patients in the BV-AVD arm and in 75.4% in the ABVD arm. Two-year PFS was higher in the BV-AVD arm compared to the ABVD arm (97.3% versus 92.6%, respectively).[45]
The NIVAHL Trial incorporated the checkpoint inhibitor nivolumab into the AVD regimen in adult patients with early-stage unfavorable cHL. One hundred nine patients were randomly assigned to either concomitant treatment with four cycles of N-AVD or sequential treatment with four cycles of nivolumab, two cycles of N-AVD, and two cycles of AVD. Both strategies were followed by 30 Gy ISRT. CR rates reached 100% with 3-year PFS rates of 100% and 98% in the concomitant and sequential groups, respectively.[46]
In another phase II study, BV and nivolumab were combined with doxorubicin and dacarbazine (AN+AD) in 154 patients with non-bulky early stage cHL. This regimen achieved an ORR of 96%, a CR rate of 92%, and a 2-year PFS of 97%, with a favorable safety profile, including a low incidence of grade ≥3 peripheral sensory neuropathy (3%) and no reported cases of febrile neutropenia.[47]
Overall, these strategies aim to reduce chemotherapy intensity by replacing more toxic agents with targeted monoclonal antibodies, potentially diminishing the need for radiotherapy and reducing both acute and long-term toxicities. However, compared with the large phase III randomized trials that established current standards of care, larger patient cohorts and longer follow-up are required to confirm their superiority in terms of efficacy and safety over the current standard CMT.
Advanced stage
For more than two decades, the optimal treatment of advanced-stage cHL has been debated, balancing the greater efficacy but higher toxicity of intensified regimens such as eBEACOPP against the more favorable safety profile but slightly lower efficacy of ABVD.[48] This dilemma has been largely addressed through PET-guided clinical trials, in which treatment is escalated or de-escalated based on early interim PET assessment, typically performed after two cycles of treatment (Table 5).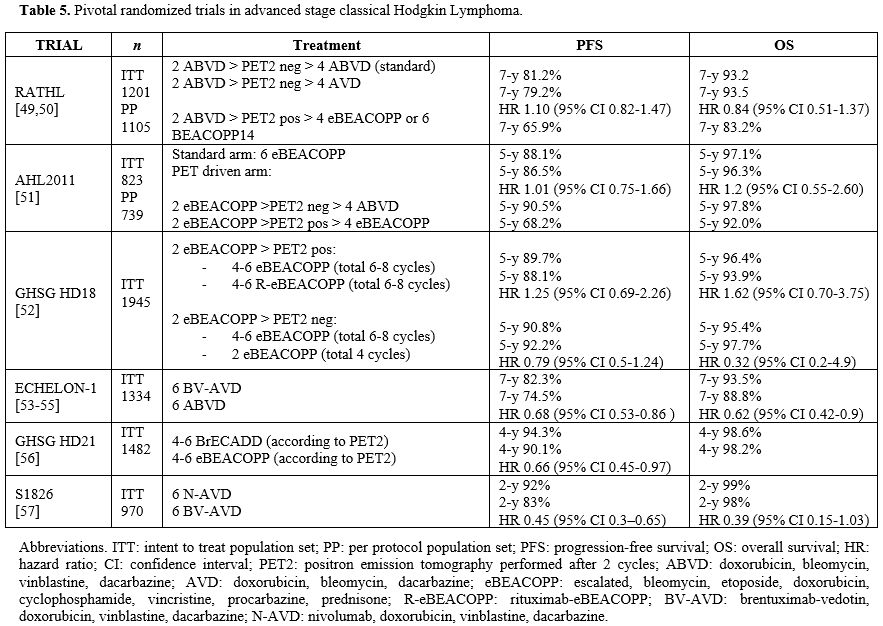 |
|
The RATHL trial explored a de-escalation strategy in PET2-negative patients after two cycles of ABVD by omitting bleomycin and continuing four cycles of AVD. The study included patients with cHL in stage IIB, III, IV, as well as selected high-risk stage IIA. The non-inferiority analysis showed comparable efficacy between the two approaches, with a lower incidence of pulmonary toxicity in patients receiving AVD compared with those continuing ABVD. In contrast, PET2 positive patients underwent treatment escalation to four cycles of eBEACOPP or six cycles of BEACOPP14, achieving favorable efficacy outcomes without any increase in secondary malignancies.[49,50]
Similarly, in the AHL2011 trial, de-escalation to four cycles of ABVD after two initial cycles of eBEACOPP in PET2-negative patients with advanced stage cHL resulted in PFS and OS similar to that of patients continuing four more cycles of eBEACOPP. In contrast, patients with PET2 positive disease – whether PET4-negative or PET4-positive - had inferior outcomes.[51]
In GHSG HD18 trial, PET2-negative patients with advanced stage cHL after two initial cycles of eBEACOPP were randomized to further 4-6 cycles (total of 6-8) or only 2 further cycles (total of 4) of eBEACOPP. Both approaches resulted in similar PFS and OS, while the abbreviated regimen was associated with reduced hematological toxicity and lower transfusion requirements. The addition of rituximab to eBEACOPP in PET2-positive patients did not improve outcomes.[52]
More recently, randomized clinical trials have integrated novel agents such as antibody drug conjugated BV and the checkpoint inhibitors nivolumab and pembrolizumab, into the chemotherapy backbone for first line treatment of advanced stage cHL.
The randomized ECHELON-1 trial demonstrated a significant improvement in long-term PFS and OS for patients with stage III and IV cHL treated with 6 cycles of BV-AVD versus ABVD. At a median follow-up of 89.3 months, the 7-year PFS rates were 82.3% versus 74.5% (HR 0.68; p=0.001), and the 7-year OS rates were 93.5% versus 88.8% (HR 0.62; p=0.011) for BV-AVD and ABVD, respectively. A higher incidence of febrile neutropenia and peripheral sensory neuropathy was observed in the BV-AVD arm.[53-55]
In the phase III GHSG HD21 trial, the novel regimen brentuximab vedotin, etoposide, cyclophosphamide, doxorubicin, dacarbazine, and dexamethasone (BrECADD) was compared with eBEACOPP in a PET-guided strategy in adult patients aged ≤60 years with advanced-stage, cHL. PET2-negative patients received two further cycles of the assigned regimen while PET2-positive patients received four further cycles. In both arms, 30 Gy IFRT or INRT was permitted on residual PET-positive disease at the end of treatment. BrECADD was associated with lower treatment-related morbidity and improved PFS compared with eBEACOPP, with no difference in OS. With a 4-year PFS of 94.3%, BrECADD achieved an unprecedented primary cure rate in large, randomized trials for advanced-stage cHL. Together with its more favorable toxicity profile compared with eBEACOPP and, in some respects, also with ABVD, these results strongly support BrECADD as a new standard treatment option for adult patients aged ≤60 years with newly diagnosed adult advanced stage cHL.[56]
The phase III SWOG S1826 trial compared nivolumab plus AVD (N-AVD) for 6 cycles with BV-AVD in adolescent and adult patients with advanced-stage cHL. At a median follow-up of 2.1 years, both PFS and EFS were superior in the N-AVD arm, and this advantage was confirmed across subgroups defined by age, stage, and IPS score. BV-AVD was associated with a higher rate of peripheral neuropathy and treatment discontinuation, whereas neutropenia was more frequent in the N-AVD arm where G-CSF prophylaxis was not mandatory. Compared with BV-AVD, N-AVD was well tolerated in older patients and showed outcomes similar to those in younger patients, without significantly increased morbidity or mortality.[57]
Pembrolizumab has also been evaluated in combination with AVD in either sequential or concomitant schedules in two single-arm phase 2 trials, both enrolling approximately 30 patients. Overall response rates were 100% in both studies, with CR rates of 100% and 90% in the sequential and concomitant cohorts, respectively, and approximately 100% 2-year PFS in both studies.[58,59] However, larger studies with longer follow-up are needed to confirm these promising results.
In the phase II SGN35-027 clinical trial, treatment-naïve patients with bulky stage I-II and stage III-IV cHL received up to 6 cycles of brentuximab-vedotin, nivolumab, doxorubicin, and dacarbazine (AN+AD). The aim of the study was to reduce the high rate of peripheral neuropathy of BV-AVD caused by concurrent use of two microtubule-disrupting agents by substituting vinblastine with nivolumab. Among 57 patients (aged 19-78 years), the ORR was 93%, CR 88%, and 2-year PFS 88%. Peripheral neuropathy occurred in 44% of patients, with only 4% grade 3.[60]
Elderly patients with Hodgkin lymphoma
Older patients account for approximately 20% of newly diagnosed cases of cHL, and this proportion is expected to increase in the coming years. Advanced age at diagnosis is often associated with a more aggressive disease biology, including a higher prevalence of mixed cellularity and lymphocyte-depleted subtypes, as well as EBV-associated HL. In addition, older patients show reduced tolerance to chemotherapy with a higher rate of treatment-related toxicities such as neurotoxicity, cytopenias, infections, bleomycin-induced pulmonary toxicity, and anthracycline-related cardiotoxicity. Consequently, long-term outcomes in older adults remain significantly inferior, with 5-year OS rates ranging from 49 to 65%, compared with approximately 90% in younger patients. Comorbidities, functional decline and organ dysfunction further limit tolerance to chemotherapy, and frailty itself represents an independent adverse prognostic factor even with intensive therapy.[61]Several geriatric assessment tools and scoring systems, including the Charlson Comorbidity Index (CCI), Cumulative Illness Rating Scale for Geriatrics (CIRS-G), and activities of daily living (ADL) and instrumental ADL (IADL) scales, have been used in lymphoma clinical trials, including those in HL. The Fondazione Italiana Linfomi (FIL) has conducted a prospective study to improve prognostic stratification of older patients with cHL aged ≥65 years, incorporating a simplified Geriatric Assessment (sGA) previously validated in DLBCL (clinicaltrials.gov ID: NCT03552003).[62,63] Fit older patients with cHL are often treated with the same regimens used in younger patients, and ABVD remains the cornerstone of treatment in both early and advanced stages. Several strategies have been adopted to mitigate toxicity. These include omitting bleomycin from the outset (AVD) or after two cycles of ABVD in PET2-negative patients, as in the RATHL trial, to reduce the risk of pulmonary toxicity. Substituting conventional doxorubicin with non-pegylated liposomal doxorubicin (MBVD) has also been shown to be safe and effective in elderly patients (> 70 years) or those with underlying cardiac disease.[64] Alternative lower-intensity regimens, such as PVAG (prednisone, vinblastine, doxorubicin, and gemcitabine), AVG (doxorubicin, vinblastine, gemcitabine), and PVAB (prednisone, vinblastine, doxorubicin, bendamustine), may offer durable remissions with improved tolerability in this population.[65-67]
BV monotherapy has demonstrated activity in elderly patients unfit for chemotherapy, although responses are often not durable.[68,69] To increase the response rate, combination strategies with single cytotoxic drugs have been explored in elderly, unfit patients. BV plus bendamustine was associated with a high incidence of serious adverse events (65%), leading to early trial termination. In contrast, a combination of BV with dacarbazine achieved a 100% ORR and 62% CR rate with a median PFS of 17.9 months, representing a reasonable frontline option for frail patients.[70]
In the ECHELON-1 trial, concomitant BV-AVD was not superior to ABVD in the subgroup of 187 patients over age 60 and was associated with increased toxicity, including higher rates of febrile neutropenia, peripheral neuropathy, and treatment-related mortality.[53] The 5-year PFS rates for BV-AVD (67.1%) and ABVD (61.8%) were not significantly different.[71] Conversely, a sequential approach incorporating BV followed by AVD (2 cycles of BV + 6 cycles of AVD + 4 cycles of BV) was better tolerated in elderly patients, with 2-year PFS and OS rates of 84% and 93%, respectively, and manageable toxicity.[72]
In the HD21 older cohort, PET-guided BrECADD was shown to be feasible and effective in patients aged 61-75 years with advanced stage cHL, although it required more frequent dose adjustments compared with younger patients. Among 85 patients, the estimated 2-year PFS and OS were 91.5% and 90.7%, respectively, after a median follow-up of 23 months. Neutropenic fever and sensory neuropathy occurred in 54% and 38% of patients, respectively, and no treatment-related deaths were reported.[73]
The non-overlapping toxicity profiles of checkpoint inhibitors and conventional chemotherapy have prompted investigation of anti-PD1 agents as frontline treatment in elderly patients with cHL. In a French trial of older frail patients with cHL and significant comorbidities (CIRS-G ≥ 6), frontline nivolumab monotherapy resulted in 28.6% complete metabolic responses (CMR) and a median PFS of 9.8 months, providing temporary disease control without curative potential.[61] The N-AVD regimen has shown favorable tolerability in fit older patients, with outcomes comparable to those observed in younger patients and without a significant increase of morbidity or mortality. In a subgroup analysis of patients aged more than 60 years from the SWOG S1826 trial, 2-year PFS and OS were 89% and 96%, respectively, with N-AVD, compared with 64% and 85% with BV-AVD. Notably, treatment discontinuation rates for the targeted agent were lower with nivolumab (14%) than with BV (55%).[74]
The multicenter phase II ACCRU trial evaluated the combination of BV plus nivolumab as first-line therapy in older or chemotherapy-ineligible patients with cHL. Although the prespecified efficacy endpoint was not met, the regimen achieved an ORR of 61% and a CMR of 48%, with a favorable safety profile and a low incidence of grade >3 adverse events.[75]
More recently, a non-comparative phase II study assessed BV combined with dacarbazine or nivolumab in elderly patients aged (≥60 years), unfit for conventional chemotherapy. Among 22 patients (median age 74 years) treated with BV and dacarbazine, ORR was 95%, CR 64%, median PFS 46.2 months and median OS not reached. In 21 patients treated with BV plus nivolumab (median age 72.1 years), ORR was 86%, CR 67%, median PFS, and median OS were not reached.[76] These results demonstrate safety and promising durable efficacy of BV-dacarbazine and BV-nivolumab combinations as potential alternatives for frontline treatment of older patients with cHL unfit for conventional chemotherapy.
Relapsed/refractory disease
Although cHL is a highly curable disease with frontline therapy, 10-25% of patients develop refractory disease or experience relapse. Established adverse prognostic factors at relapse include primary refractory disease (failure to achieve complete remission), relapse within 12 months from the end of first-line therapy, extranodal involvement at relapse, B symptoms, and stage IV disease.[77] Historically, salvage chemotherapy followed by high-dose therapy (HDT) and autologous stem cell transplantation (ASCT) has represented the standard treatment for eligible fit patients aged < 65-70 years without significant comorbidities. PET imaging performed after salvage chemotherapy and before ASCT has emerged as the strongest prognostic factor for ASCT outcome. Achieving PET negativity (Deauville score 1-3) is now considered a key prerequisite before proceeding to ASCT.[78-79] Several salvage regimes are currently used in patients with relapsed/refractory cHL and can be broadly grouped into platinum-based or gemcitabine-based combinations.[80,81] No randomized trials demonstrated superiority of one regimen over another. Traditional salvage chemotherapies include DHAP (dexamethasone, high-dose cytarabine, and cisplatin), ESHAP (etoposide, methylprednisolone, high-dose cytarabine, and cisplatin), GDP (gemcitabine, dexamethasone, and cisplatin), GVD (gemcitabine, vinorelbine, and liposomal doxorubicin), IGEV (ifosfamide, gemcitabine, and vinorelbine), ICE (ifosfamide, carboplatin, and etoposide), and BEGEV (bendamustine, gemcitabine, and vinorelbine). Complete responses with these regimens occur in a range from approximately 50% of patients reported for platinum-based regimens to 70% reported for the BEGEV regimen, resulting in PFS rates of 52–77% at 3-5 years for patients who successfully undergo ASCT (Table 6).[82-90]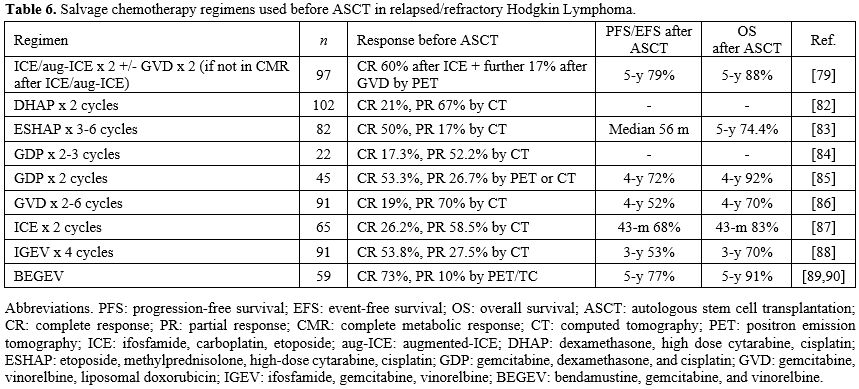 |
|
Until the early 2010s, patients with refractory or relapsed cHL after ASCT had a poor prognosis, with limited therapeutic options aside from allogeneic stem cell transplantation (SCT) in selected cases achieving a second remission. This scenario has changed drastically with the advent of novel targeted therapies, which have reshaped the therapeutic landscape of cHL across all treatment lines.
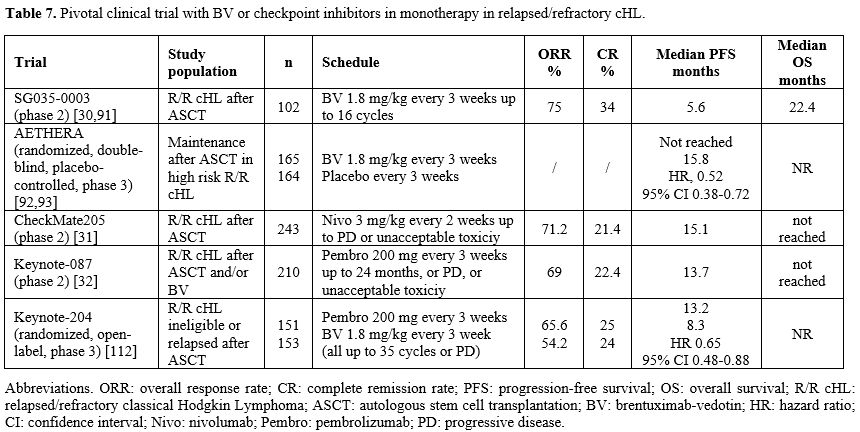
In 2012, Younes and colleagues published the results of a pivotal phase II study evaluating treatment with the anti-CD30 antibody-drug conjugate BV in 102 patients with relapsed or refractory cHL after ASCT. Results were encouraging, with an ORR of 75%, a CR rate of 34%, a median PFS of 5.6 months, and a median duration of response (DOR) of 20.5 months among patients achieving CR. During the 5 years of follow-up, patients who achieved a CR had estimated OS and PFS rates of 64% and 52%, respectively. The most common treatment-emergent adverse event was peripheral sensory neuropathy, which occurred in 43% of patients (grade 3 events occurred in 8%) and resolved or improved after drug discontinuation in 88% of cases (Table 7).[30,91]
 |
|
Thereafter, BV was evaluated in multiple settings in relapsed/refractory cHL. In the randomized, double-blind, placebo-controlled, phase III AETHERA trial, 329 patients with high-risk relapsed or primary refractory cHL who had undergone ASCT were randomly assigned 16 cycles of BV or placebo every 3 weeks, starting 30-45 days after transplantation. 5-year PFS was significantly improved with BV maintenance (59% vs 41% with placebo).[92,93] As the AETHERA trial did not include patients previously exposed to BV, the EBMT Lymphoma Working Party performed a retrospective real-world analysis of 353 refractory/relapsed cHL patients who received BV maintenance after ASCT. Of these, 52.6% received BV prior to ASCT. The 5-year OS and PFS from the start of BV maintenance were 85.1% and 69.9%, respectively, and a trend toward improved PFS and lower relapse risk was observed in patients exposed to BV before ASCT.[94]
The combination of BV with the CPI Nivolumab as post-ASCT consolidation has also been explored. In a study of 59 high-risk patients, 8 cycles of BV plus nivolumab, administered every 3 weeks, resulted in an 18-month PFS of 94%.[95]
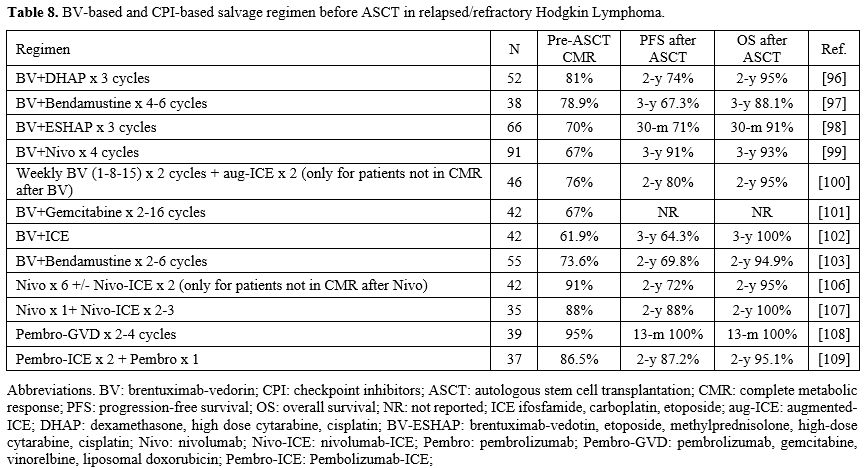
BV was incorporated into several salvage regimens before ASCT, both sequentially and concomitantly with chemotherapy, yielding high CMR rates of 66% to 83%. However, no randomized studies have directly compared these approaches with conventional chemotherapy-based salvage regimens (Table 8).[96-103] A propensity score-matched analysis of 10 single-arm salvage studies found that BV-based salvage regimens did not increase pre-ASCT CMR but improved 3-year PFS in patients with relapsed HL. Notably, this benefit was not observed in patients with primary refractory disease, suggesting that BV may not overcome chemoresistance in this subgroup.[104]
 |
|
A second class of drugs that has revolutionized the treatment of relapsed/refractory cHL consists of the anti-PD1 CPI. By blocking the interaction between PD-L1 on HRS cells and tumor-associated macrophages, and between PD1 on tumor-infiltrating T-lymphocytes, these drugs restore host immune responses, leading to meaningful clinical responses even in heavily pretreated and chemo refractory patients. Two pivotal clinical studies led to the approval of nivolumab and pembrolizumab by FDA and EMA for the treatment of refractory/relapsed patients after or ineligible for ASCT (Table 7).[31,32] In the multicenter, single-arm, phase II CheckMate-205 study, which enrolled 243 patients, nivolumab monotherapy until disease progression or unacceptable toxicity achieved an ORR of 71.2%, with CR rate of 21.4%, a median PFS of 15.1 months, a median DOR of 18.2 months, a median duration of CR of 30.3 months, and a 5-year OS of 71.4%.[31] Similarly, in the KEYNOTE-087 trial, pembrolizumab administered as monotherapy for up to 2 years in 210 cHL patients resulted in an ORR of 71.4%, with CR rate of 27.6%, a median PFS of 13.7 months, a median DOR of 16.6 months; median duration of CR and median OS were not reached. Retreatment upon relapse after discontinuation achieved a secondary ORR of 73.7% and a median secondary DOR of 15.2 months.[32] The widespread use of CPI has led to a revision of PET response criteria, as immune-mediated inflammatory changes may mimic disease progression (pseudo-progression). This has prompted the development of Lymphoma Response to Immunomodulatory Therapy Criteria (LYRIC), which better captures these atypical response patterns.[105]
As observed with BV, once their efficacy as monotherapy was established in relapsed/refractory patients, anti-PD1 CPI were combined with several agents in pretransplant salvage regimens, including ICE, GVD or BV, with high pretransplant CMR rates (Table 8).[99,106-109] In a large retrospective study, including 1280 patients with relapsed/refractory cHL who underwent ASCT from 2010 to 2022 in 6 transplant centers, patients who received PD-1 inhibitors at any point before ASCT had a significantly higher 2-year PFS than those who received BV without PD-1 inhibitors or patients receiving chemotherapy alone (88.2%, 70.2%, and 67.4%, respectively; P < 0.0001). This benefit was observed both in patients achieving CMR and those in partial metabolic response (PMR) prior to ASCT, although no differences in OS were noted. These findings support the use of PD-1–based salvage regimens in patients proceeding to ASCT.[110]
The introduction of novel agents has significantly improved outcomes in cHL patients relapsed after ASCT with PFS increasing from 43 % to 71 %.[111] Anti-PD1 CPI have shown superior efficacy and are considered the preferred treatment option in this setting. In the phase III KEYNOTE-204 trial, pembrolizumab treatment resulted in superior PFS compared with BV among 304 patients with cHL who relapsed after ASCT or were ineligible for ASCT (Table 7).[112]
For younger and fit patients who relapse after ASCT, either responding to CPI or with disease refractory to CPI, allogeneic SCT still represents a potentially curative option owing to the graft-versus-lymphoma effect. However, concerns persist regarding the increased risk of acute graft-versus-host disease (GVHD) following prior CPI exposure. A large analysis from the Center for International Blood and Marrow Transplant Research (CIBMTR) and European Society for Blood and Marrow Transplantation (EBMT) including 2186 adult patients transplanted between 2008 to 2023, demonstrated that prior CPI exposure was associated with improved PFS and reduced relapse risk, but also with increased incidence of grade 2-4 acute GVHD, without impacting OS, non-relapse mortality and chronic GVHD. Importantly, the use of post-transplant cyclophosphamide (PTCy) was associated with improved OS and reduced rates of grade 2-4 acute GVHD and chronic GVHD in this setting.[113] These findings are supported by additional retrospective studies showing improved PFS and lower relapse rates in patients treated with CPI prior to allogeneic SCT compared with those treated with chemotherapy alone or BV-containing regimens without CPI before allogeneic SCT.[114,115] The increased risk of acute GVHD associated with pretransplant exposure to CPI appears to be mitigated in those receiving longer immunosuppression (day 180) compared with a shorter duration (60 days).[115]
Based on current evidence, the American Society of Transplantation and Cellular Therapy Committee on Practice Guidelines recommends a washout period of at least 30-60 days between exposure to CPI and allogeneic SCT, the use of reduced intensity conditioning, and post-transplant cyclophosphamide for GVHD prophylaxis.[116]
Novel agents
Despite the substantial advances achieved by the introduction of the antibody drug conjugate BV and the anti-PD1 CPI nivolumab and pembrolizumab, therapeutic options remain limited for patients who progress after these agents. Novel immunotherapies are under development for patients with relapsed/refractory cHL, including chimeric antigen receptor-T cell (CAR-T) products, EBV-specific T cells, bispecific antibodies, and new checkpoint inhibitor combinations.[117] Among these, anti-CD30 CAR-T cells and the anti-CD30/CD16A bispecific antibody AFM13 represent particularly promising approaches.A meta-analysis of 151 patients from eight studies investigating anti-CD30 CAR-T cell therapy in relapsed/refractory cHL reported an ORR of 57% with 34% CR, 1-year PFS of 39%, and 1-year OS of 89%. The most common hematologic adverse event was leukopenia (71.4%), while among non-hematologic adverse events, cytokine release syndrome (CRS) and immune effector cells associated neurologic syndrome (ICANS) occurred in 30.4% and 13.2% of patients, respectively.[118]
AFM13 (Acimtamig) is a first-in-class, tetravalent anti-CD30/CD16A bispecific antibody, designed to engage and activate NK cells to the selective killing of CD30+ tumor cells. In a phase I-II trial, AFM13 showed modest activity, with ORR ranging from 16.7-23%.[119,120] However, when combined with pembrolizumab in a phase Ib study enrolling 30 heavily pretreated patients with CD30+ HL, the ORR increased to 83% with a CR rate of 37%.[121] More recently, AFM13 was combined with preactivated allogeneic cord blood-derived NK cells and administered to heavily pretreated patients with CD30+ lymphomas (37 of the 42 patients had HL), resulting in ORR and CR rates of 92.8% and 66.7%, respectively. No cases of CRS, neurotoxicity, or GVHD were reported, and 2-year EFS and OS were 26.2% and 76.2%, respectively. Overall, these emerging immunotherapeutic strategies represent promising options for relapsed patients with cHL and warrant further investigations.[122]
Follow-up and Survivorship
Follow-up for patients with cHL aims to detect disease relapses and to monitor treatment-related late toxicities. Given the high curability of cHL, long-term survivorship care is a crucial component of post-treatment management. Current recommendations, largely based on international guidelines, distinguish between follow-up during the first five years after therapy and long-term monitoring beyond this period.[14,28,29]At the completion of treatment, response assessment should include FDG-PET/CT within three months to document complete remission.
During the first five years after therapy, clinical follow-up is primarily based on periodic history and physical examination, performed every 3–6 months during the first two years, every 6–12 months until the third year, and annually thereafter. Laboratory testing generally includes complete blood count and metabolic profile as clinically indicated, with annual thyroid function testing in patients who received cervical irradiation. Preventive care is also recommended during this phase, including annual influenza vaccination, reduction of cardiovascular risk factors, and patient education on the risk of secondary malignancies.
Routine surveillance imaging is no longer recommended in asymptomatic patients. Imaging studies should be performed only when clinically indicated, as surveillance PET/CT is associated with a high rate of false-positive findings and does not improve survival outcomes.[13] This approach is supported by population-based data showing no survival benefit from routine surveillance imaging in patients with cHL in first complete remission.[123]
Beyond 5 years, follow-up focuses primarily on detecting and preventing late treatment-related complications, particularly cardiovascular disease and second primary malignancies. Long-term observational studies have demonstrated that survivors of cHL have a two- to four-fold increased risk of these conditions, which represent the leading causes of late mortality.[124] Although contemporary treatment strategies, such as PET-adapted approaches and reduced use of radiotherapy, may mitigate some of these risks, long-term monitoring remains essential.
In this context, the use of advanced echocardiographic assessment tools may provide additional clinical value. Beyond conventional parameters, such as left ventricular ejection fraction (LVEF) and global longitudinal strain (GLS), myocardial work (MW) analysis enables a more comprehensive and less load-dependent evaluation of cardiac function, by integrating blood pressure into the assessment. In a cohort of Hodgkin lymphoma survivors, global work index (WI) and global constructive work (GCW) has been shown to be reduced compared with healthy controls, suggesting the presence of subclinical myocardial impairment, whereas global wasted work (GWW) and global wasted efficiency (GWE) remain unchanged. MW indices have been found to correlate strongly with LVEF and systolic blood pressure, consistent with prior evidence. Importantly, MW may facilitate the diagnosis of cancer therapy-related cardiac dysfunction (CTRCD), particularly in patients with preserved LVEF and borderline GLS. As such, it represents a sensitive tool for the early detection of cardiac dysfunction in this high-risk population, reinforcing the importance of incorporating advanced echocardiographic parameters into long-term survivorship surveillance strategies.[125]
Critical Perspectives and Future Directions
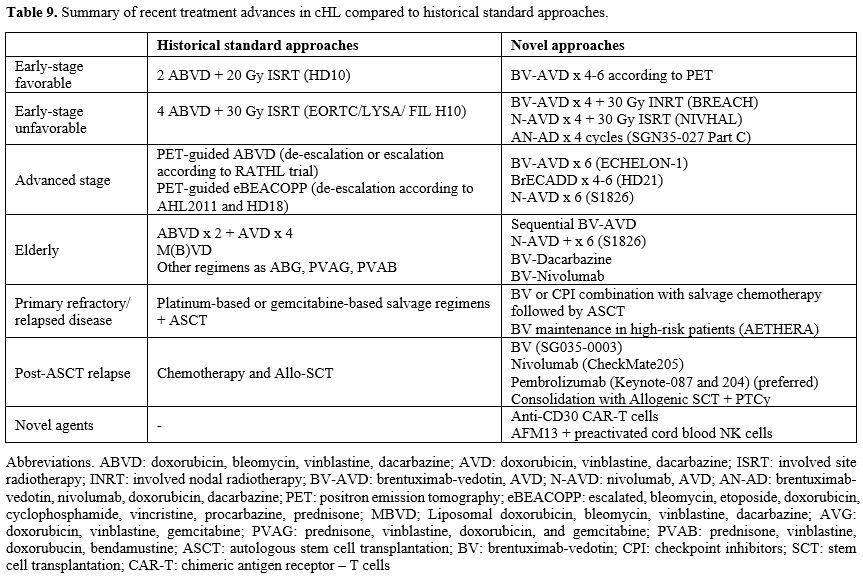
In recent years, significant progress has been made in the treatment of Hodgkin lymphoma, with improved efficacy and reduced toxicity. These advances have been driven by pivotal clinical trials based on PET-adapted approaches and the integration of novel targeted agents into modified multi-agent chemotherapy regimens.In early-stage cHL, two ABVD followed by 20 Gy ISRT/INRT and four ABVD followed by 30 Gy ISRT/INRT represent the standard of treatment in favorable and unfavorable risk groups, respectively. For now, radiotherapy is far from being abandoned. Omission of radiotherapy is associated with inferior PFS but can reduce the risk of late toxicities, especially secondary primary malignancies, although this may be debated given modern approaches such as INRT and ISRT, which significantly limit the irradiation fields. The advantage of CMT is not significant when a more intensive chemotherapy regimen, like eBEACOPP, or a longer chemotherapy course, like six cycles of ABVD, is used as induction treatment, but in these cases, patients should deal with other kinds of toxicities. Moreover, both NIVHAL and BREACH trials, which combine Nivolumab or BV with AVD, respectively, still consider radiotherapy as consolidation after chemotherapy. Until randomized clinical trials with new drug combinations are available, eventual omission of radiotherapy should be personalized according to the patient’s preference and comorbidities, disease extension, fields of irradiation, and PET-related radiomic parameters.
For advanced-stage cHL, large randomized clinical trials have shown that BrECADD and N-AVD are superior to eBEACOPP and BV-AVD, respectively, in terms of PFS but not OS. In the absence of a direct comparison through randomized controlled trials or propensity score matching studies, both BrECADD and N-AVD are considered the preferred first-line treatments for advanced-stage cHL by current major published guidelines, in place of previously favored BV-AVD, eBEACOPP, and ABVD.[14,28,29] The strength of BrECADD lies in longer follow-up, the highest PFS rate ever achieved in this patient population, and a PET-adapted approach that may reduce the number of cycles in PET2-negative patients, making BrECADD the preferred treatment option for fit patients aged < 60 with advanced-stage cHL, according to European Society of Medical Oncology (ESMO) guidelines.[29] The strength of N-AVD consists of reduced hematologic toxicity without mandatory G-CSF use and optimal results in older populations comparable to those seen in younger patients, making N-AVD the preferred treatment option for older patients aged 60-80 years, as well as an alternative to BrECADD in younger patients.[29] Other valid first-line treatments, such as PET-guided regimens like ABVD and eBEACOPP, or concomitant or sequential BV-AVD, can be considered where BrECADD and N-AVD are not available.
In the relapsed/refractory patients, the role of BV and CPI should be reconsidered according to their use in first line. While the benefit of BV incorporation in salvage regimens seems more evident in relapsed than in primary refractory patients, its role as maintenance after ASCT in high-risk patients is supported by the AETHERA randomized trial and has become a common clinical practice.[92,104] Previous BV use before ASCT does not negatively affect maintenance efficacy and should not be considered a contraindication.[94] On the contrary, the use of CPI at any point before ASCT significantly increases the post-transplant PFS, supporting the use of PD-1–based salvage regimens in patients proceeding to ASCT.[110] For patients who relapse after ASCT or are not candidates for it, pembrolizumab is, at present, the best available treatment, followed by allogeneic SCT with PTCy, depending on donor availability and the patient’s age, comorbidities, and preferences.
Table 9 summarizes novel treatments in cHL compared with historical standard approaches.
 |
|
The translation of the most recent advances of cHL treatment into routine clinical practice is often delayed due to the lengthy process of regulatory approval and reimbursement negotiations within of national health care systems. As a result, patient management may vary considerably across countries.
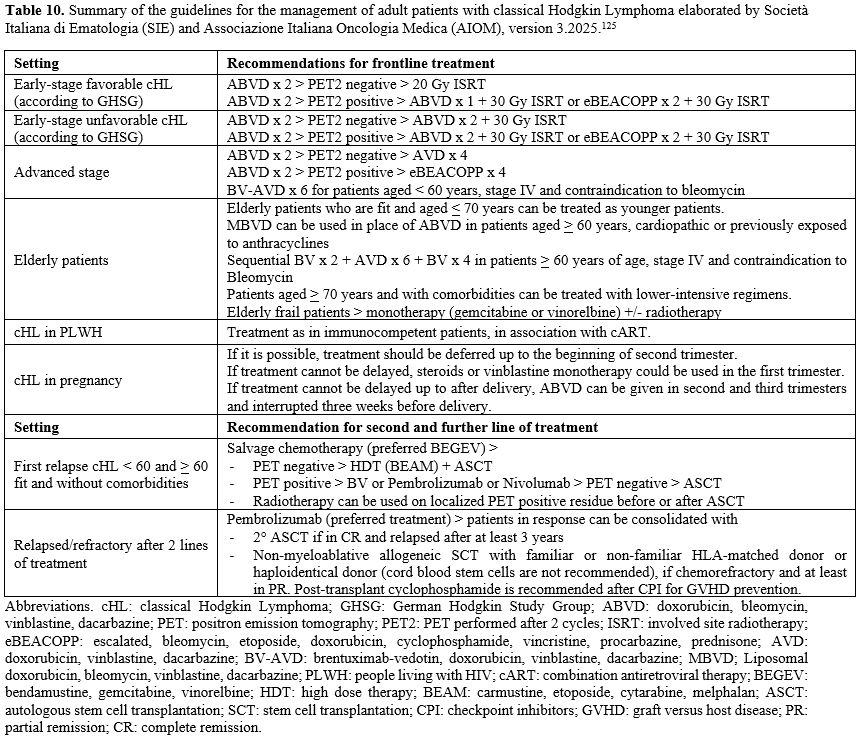
In Italy, current clinical practice is guided by the “Guidelines for the management of adult patients with classical Hodgkin Lymphoma” (version 3.2025), developed by the Società Italiana di Ematologia (SIE) and Associazione Italiana di Oncologia Medica (AIOM), and published within the National Guideline System of the Istituto Superiore di Sanità. These guidelines define the treatment strategies that are currently approved and reimbursed within the Italian HealthCare System.[126] (Table 10). Compared to the most recent ESMO, Lymphoma Study Association (LYSA) and National Comprehensive Cancer Network (NCCN) guidelines,[14,28,29] the Italian recommendations do not yet incorporate recently developed therapeutic approaches, such as BrECADD and Nivo-AVD in the frontline settings, as well as BV or CPI-based combinations in salvage regimens for refractory/relapsed patients. These treatments are therefore generally limited to off-label use. Future regulatory approvals are expected to help bridge the gap between emerging clinical evidence and its implementation in routine clinical practice.
 |
|
For the next future, huge expectations are put on the anti-CD30 CAR-T cells and mostly on the combination of the anti-CD30/CD16A bispecific antibody AFM13 with preactivated allogeneic cord blood derived NK cells, which configure as interesting solution for multiple relapsed/refractory heavily pretreated patients, who have failed CPI.
Finally, ct-DNA and MTV are established as innovative and effective prognostic tools in clinical trials but need standardization to become integrated in current clinical practice and overcome limits of historical prognostic classification systems and ambiguous PET interpretations. This will further contribute to personalizing treatment, increasing cure rate and sparing needless toxicities in patients with cHL.
References
- Cancer Stat Facts: Hodgkin Lymphoma, https://seer.cancer.gov/statfacts/html/hodg.html
- Brice P, de Kerviler E, Friedberg JW. Classical Hodgkin lymphoma. Lancet. 2021; 398:1518-27. https://doi.org/10.1016/S0140-6736(20)32207-8 PMid:33493434
- Fallah
M, Liu X, Ji J, Försti A, Sundquist K, Hemminki K. Hodgkin lymphoma
after autoimmune diseases by age at diagnosis and histological subtype.
Ann Oncol. 2014;25:1397-04. https://doi.org/10.1093/annonc/mdu144 PMid:24718892
- Alibrahim
MN, Gloghini A, Carbone A, Immune Deficiency/Dysregulation-Associated
EBV-Positive Classic Hodgkin Lymphoma. Cancers (Basel) 2025;17:1433. https://doi.org/10.3390/cancers17091433 PMid:40361360 PMCid:PMC12070896
- Thomsen
H, da Silva Filho MI, Försti A, Fuchs M, Ponader S, von Strandmann EP,
Eisele L, Herms S, Hofmann P, Sundquist J, Engert A, Hemminki K.
Heritability estimates on Hodgkin's lymphoma: a genomic-versus
population-based approach. Eur J Hum Genet. 2015;23:824-30. https://doi.org/10.1038/ejhg.2014.184 PMid:25227146 PMCid:PMC4795060
- Roganovic
J, Matijasic Stjepovic N, Dordevic A. Unfolding the enigma of familial
Hodgkin lymphoma: Current insights. World J Clin Cases. 2026;14:111246.
https://doi.org/10.12998/wjcc.v14.i1.111246 PMid:41551691 PMCid:PMC12809157
- Alaggio
R, Amador C, Anagnostopoulos I, Attygalle AD, Araujo IBO, Berti E,
Bhagat G, Borges AM, Boyer D, Calaminici M, Chadburn A, Chan JKC, Cheuk
W, Chng WJ, Choi JK, Chuang SS, Coupland SE, Czader M, Dave SS, de Jong
D, Du MQ, Elenitoba-Johnson KS, Ferry J, Geyer J, Gratzinger D, Guitart
J, Gujral S, Harris M, Harrison CJ, Hartmann S, Hochhaus A, Jansen PM,
Karube K, Kempf W, Khoury J, Kimura H, Klapper W, Kovach AE, Kumar S,
Lazar AJ, Lazzi S, Leoncini L, Leung N, Leventaki V, Li XQ, Lim MS, Liu
WP, Louissaint A Jr, Marcogliese A, Medeiros LJ, Michal M, Miranda RN,
Mitteldorf C, Montes-Moreno S, Morice W, Nardi V, Naresh KN, Natkunam
Y, Ng SB, Oschlies I, Ott G, Parrens M, Pulitzer M, Rajkumar SV,
Rawstron AC, Rech K, Rosenwald A, Said J, Sarkozy C, Sayed S, Saygin C,
Schuh A, Sewell W, Siebert R, Sohani AR, Tooze R, Traverse-Glehen A,
Vega F, Vergier B, Wechalekar AD, Wood B, Xerri L, Xiao W. The 5th
edition of the World Health Organization Classification of
Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022;36:1720-48.
https://doi.org/10.1038/s41375-022-01620-2 PMid:35732829 PMCid:PMC9214472
- Campo
E, Jaffe ES, Cook JR, Quintanilla-Martinez L, Swerdlow SH, Anderson KC,
Brousset P, Cerroni L, de Leval L, Dirnhofer S, Dogan A, Feldman AL,
Fend F, Friedberg JW, Gaulard P, Ghia P, Horwitz SM, King RL, Salles G,
San-Miguel J, Seymour JF, Treon SP, Vose JM, Zucca E, Advani R, Ansell
S, Au WY, Barrionuevo C, Bergsagel L, Chan WC, Cohen JI, d'Amore F,
Davies A, Falini B, Ghobrial IM, Goodlad JR, Gribben JG, Hsi ED, Kahl
BS, Kim WS, Kumar S, LaCasce AS, Laurent C, Lenz G, Leonard JP, Link
MP, Lopez-Guillermo A, Mateos MV, Macintyre E, Melnick AM, Morschhauser
F, Nakamura S, Narbaitz M, Pavlovsky A, Pileri SA, Piris M, Pro B,
Rajkumar V, Rosen ST, Sander B, Sehn L, Shipp MA, Smith SM, Staudt LM,
Thieblemont C, Tousseyn T, Wilson WH, Yoshino T, Zinzani PL, Dreyling
M, Scott DW, Winter JN, Zelenetz AD. The International Consensus
Classification of Mature Lymphoid Neoplasms: a report from the Clinical
Advisory Committee. Blood. 2022;140:1229-53. https://doi.org/10.1182/blood.2022015851 PMid:35653592 PMCid:PMC9479027
- Green
MR, Monti S, Rodig SJ, Juszczynski P, Currie T, O'Donnell E, Chapuy B,
Takeyama K, Neuberg D, Golub TR, Kutok JL, Shipp MA. Integrative
analysis reveals selective 9p24.1 amplification, increased PD-1 ligand
expression, and further induction via JAK2 in nodular sclerosing
Hodgkin lymphoma and primary mediastinal large B-cell lymphoma. Blood.
2010;116:3268-77. https://doi.org/10.1182/blood-2010-05-282780 PMid:20628145 PMCid:PMC2995356
- Spina
V, Bruscaggin A, Cuccaro A, Martini M, Di Trani M, Forestieri G,
Manzoni M, Condoluci A, Arribas A, Terzi-Di-Bergamo L, Locatelli SL,
Cupelli E, Ceriani L, Moccia AA, Stathis A, Nassi L, Deambrogi C, Diop
F, Guidetti F, Cocomazzi A, Annunziata S, Rufini V, Giordano A, Neri A,
Boldorini R, Gerber B, Bertoni F, Ghielmini M, Stüssi G, Santoro A,
Cavalli F, Zucca E, Larocca LM, Gaidano G, Hohaus S, Carlo-Stella C,
Rossi D. Circulating tumor DNA reveals genetics, clonal evolution, and
residual disease in classical Hodgkin lymphoma. Blood.
2018;131:2413-25. https://doi.org/10.1182/blood-2017-11-812073 PMid:29449275
- Alig
SK, Shahrokh Esfahani M, Garofalo A, Li MY, Rossi C, Flerlage T,
Flerlage JE, Adams R, Binkley MS, Shukla N, Jin MC, Olsen M, Telenius
A, Mutter JA, Schroers-Martin JG, Sworder BJ, Rai S, King DA, Schultz
A, Bögeholz J, Su S, Kathuria KR, Liu CL, Kang X, Strohband MJ,
Langfitt D, Pobre-Piza KF, Surman S, Tian F, Spina V, Tousseyn T,
Buedts L, Hoppe R, Natkunam Y, Fornecker LM, Castellino SM, Advani R,
Rossi D, Lynch R, Ghesquières H, Casasnovas O, Kurtz DM, Marks LJ, Link
MP, André M, Vandenberghe P, Steidl C, Diehn M, Alizadeh AA. Distinct
Hodgkin lymphoma subtypes defined by noninvasive genomic profiling.
Nature. 2024;625:778-87. https://doi.org/10.1038/s41586-023-06903-x PMid:38081297 PMCid:PMC11293530
- Pirosa
MC, Bruscaggin A, Terzi di Bergamo L, Salehi M, Jauk F, Forestieri G,
Bocchetta S, Piffaretti D, Moia R, Cristaldi V, di Trani M, Galimberti
GA, Pini K, Spina V, Giordano C, Condoluci A, Romano I, Annunziata S,
Bergesio F, Boldorini R, Borsatti E, Bulian P, Calabretta E, Chauvie S,
Corrado F, Crisci S, Cuzzocrea M, De Filippi R, Gerber B, Kurlapski M,
Larocca LM, Merlo E, Rinaldi A, Rodari M, Romanowicz G, Sacchetti GM,
Stathis A, Stüssi G, Zangrilli I, Pinto A, Mazzucchelli L, Gattei V,
Zaucha JM, Santoro A, Hohaus S, Cavalli F, Tzankov A, Carlo-Stella C,
Gaidano G, Ceriani L, Zucca E, Rossi D. A comprehensive genetic study
of classic Hodgkin lymphoma using circulating tumor DNA. Blood.
2025;146:1207-12. https://doi.org/10.1182/blood.2024027355 PMid:40359477
- Cheson
BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, Lister
TA; Alliance, Australasian Leukaemia and Lymphoma Group; Eastern
Cooperative Oncology Group; European Mantle Cell Lymphoma Consortium;
Italian Lymphoma Foundation; European Organisation for Research;
Treatment of Cancer/Dutch Hemato-Oncology Group; Grupo Español de
Médula Ósea; German High-Grade Lymphoma Study Group; German Hodgkin's
Study Group; Japanese Lymphorra Study Group; Lymphoma Study
Association; NCIC Clinical Trials Group; Nordic Lymphoma Study Group;
Southwest Oncology Group; United Kingdom National Cancer Research
Institute. Recommendations for initial evaluation, staging, and
response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano
classification. J Clin Oncol. 2014;32:3059-68. https://doi.org/10.1200/JCO.2013.54.8800 PMid:25113753 PMCid:PMC4979083
- Rossi
C, Manson G, Marouf A, Cabannes-Hamy A, Nicolas-Virelizier E, Maerevoet
M, Alcantara M, Molina L, Ceraulo A, Poirée M, Galtier J, Diop N,
Delette C, Segot A, Dubois S, Waultier A, Bernard S, Noël R, Guidez S,
Kohn M, Bailly S, Moatti H, Touati M, Renaud L, Kanoun S, Cottereau AS,
Kirova Y, Peignaux K, Dourthe ME, Simonin M, Leblanc T, Quéro L,
Krzisch D, Duléry R, Grenier A, Gastinne T, Casasnovas O, Gallamini A,
André M, Morschhauser F, Deau B, Fornecker LM, Ghesquières H. Classic
Hodgkin Lymphoma: The LYSA pragmatic guidelines. Eur J Cancer.
2024;213:115073. https://doi.org/10.1016/j.ejca.2024.115073 PMid:39509848
- Hasenclever
D, Diehl V. A prognostic score for advanced Hodgkin's disease.
International Prognostic Factors Project on Advanced Hodgkin's Disease.
N Engl J Med. 1998;339:1506-14. https://doi.org/10.1056/NEJM199811193392104 PMid:9819449
- Rodday
AM, Evens AM, Maurer MJ, Upshaw JN, Counsell N, Rossetti S, Chang C,
Cui Z, Xiang Q, Mwangi R, Advani R, Andre M, Gallamini A, Hay AE,
Hodgson DC, Hoppe RT, Hutchings M, Johnson P, Mou E, Opat S, Raemaekers
J, Savage KJ, Parsons SK, Radford J. An Individualized Prediction Model
for Early-Stage Classic Hodgkin's Lymphoma. NEJM Evid.
2025;4:EVIDoa2500115. https://doi.org/10.1056/EVIDoa2500115 PMid:40536772 PMCid:PMC12498259
- Rodday
AM, Parsons SK, Upshaw JN, Friedberg JW, Gallamini A, Hawkes E, Hodgson
D, Johnson P, Link BK, Mou E, Savage KJ, Zinzani PL, Maurer M, Evens
AM. The Advanced-Stage Hodgkin Lymphoma International Prognostic Index:
Development and Validation of a Clinical Prediction Model From the
HoLISTIC Consortium. J Clin Oncol. 2023;41:2076-86. https://doi.org/10.1200/JCO.22.02473 PMid:36495588 PMCid:PMC10082254
- Barrington
SF, Mikhaeel NG, Kostakoglu L, Meignan M, Hutchings M, Müeller SP,
Schwartz LH, Zucca E, Fisher RI, Trotman J, Hoekstra OS, Hicks RJ,
O'Doherty MJ, Hustinx R, Biggi A, Cheson BD. Role of imaging in the
staging and response assessment of lymphoma: consensus of the
International Conference on Malignant Lymphomas Imaging Working Group.
J Clin Oncol. 2014;32:3048-58. https://doi.org/10.1200/JCO.2013.53.5229 PMid:25113771 PMCid:PMC5015423
- Gallamini
A, Rigacci L, Merli F, Nassi L, Bosi A, Capodanno I, Luminari S, Vitolo
U, Sancetta R, Iannitto E, Trentin L, Stelitano C, Tavera S, Biggi A,
Castagnoli A, Versari A, Gregianin M, Pelosi E, Torchio P, Levis A. The
predictive value of positron emission tomography scanning performed
after two courses of standard therapy on treatment outcome in advanced
stage Hodgkin's disease. Haematologica. 2006;91:475-81
- Gallamini
A, Barrington SF, Biggi A, Chauvie S, Kostakoglu L, Gregianin M,
Meignan M, Mikhaeel GN, Loft A, Zaucha JM, Seymour JF, Hofman MS,
Rigacci L, Pulsoni A, Coleman M, Dann EJ, Trentin L, Casasnovas O,
Rusconi C, Brice P, Bolis S, Viviani S, Salvi F, Luminari S, Hutchings
M The predictive role of interim positron emission tomography for
Hodgkin lymphoma treatment outcome is confirmed using the
interpretation criteria of the Deauville five-point scale.
Haematologica. 2014;99:1107-13. https://doi.org/10.3324/haematol.2013.103218 PMid:24658820 PMCid:PMC4040916
- Illidge
TM, Phillips EH, Counsell N, Pettengell R, Johnson PWM, Culligan DJ,
Popova B, Clifton-Hadley L, McMillan A, Hoskin P, Barrington SF,
Radford J. Maximum tumor diameter is associated with event-free
survival in PET-negative patients with stage I/IIA Hodgkin lymphoma.
Blood Adv. 2020;4:203-6. https://doi.org/10.1182/bloodadvances.2019001023 PMid:31935289 PMCid:PMC6960465
- Phillips
EH, Counsell N, Illidge T, Andre M, Aurer I, Fiaccadori V, Fortpied C,
Neven A, Federico M, Barrington SF, Raemaekers J, Radford J. Maximum
tumor diameter is associated with relapse risk in limited-stage Hodgkin
lymphoma: an international study. Blood Adv. 2025;9:2266-74. https://doi.org/10.1182/bloodadvances.2024015140 PMid:39774828 PMCid:PMC12124608
- Rossi
C, André M, Dupuis J, Morschhauser F, Joly B, Lazarovici J, Ghesquières
H, Stamatoullas A, Nicolas-Virelizier E, Feugier P, Gac AC, Moatti H,
Fornecker LM, Deau B, Joubert C, Fortpied C, Raemaekers J, Federico M,
Kanoun S, Meignan M, Traverse-Glehen A, Cottereau AS, Casasnova RO.
High-risk stage IIB Hodgkin lymphoma treated in the H10 and AHL2011
trials: total metabolic tumor volume is a useful risk factor to
stratify patients at baseline. Haematologica. 2022;107:2897-904. https://doi.org/10.3324/haematol.2021.280004 PMid:35638548 PMCid:PMC9713544
- Boellaard
R, Buvat I, Nioche C, Ceriani L, Cottereau AS, Guerra L, Hicks RJ,
Kanoun S, Kobe C, Loft A, Schöder H, Versari A, Voltin CA, Zwezerijnen
GJC, Zijlstra JM, Mikhaeel NG, Gallamini A, El-Galaly TC, Hanoun C,
Chauvie S, Ricci R, Zucca E, Meignan M, Barrington SF. International
Benchmark for Total Metabolic Tumor Volume Measurement in Baseline
(18)F-FDG PET/CT of Lymphoma Patients: A Milestone Toward Clinical
Implementation. J Nucl Med. 2024;65:1343-8. https://doi.org/10.2967/jnumed.124.267789 PMid:39089812 PMCid:PMC11372260
- Steidl
C, Lee T, Shah SP, Farinha P, Han G, Nayar T, Delaney A, Jones SJ,
Iqbal J, Weisenburger DD, Bast MA, Rosenwald A, Muller-Hermelink HK,
Rimsza LM, Campo E, Delabie J, Braziel RM, Cook JR, Tubbs RR, Jaffe ES,
Lenz G, Connors JM, Staudt LM, Chan WC, Gascoyne RD. Tumor-associated
macrophages and survival in classic Hodgkin's lymphoma. N Engl J Med.
2010;362:875-85. https://doi.org/10.1056/NEJMoa0905680 PMid:20220182 PMCid:PMC2897174
- Cuccaro
A, Annunziata S, Cupelli E, Martini M, Calcagni ML, Rufini V, Giachelia
M, Bartolomei F, Galli E, D'Alò F, Voso MT, Leone G, Giordano A,
Larocca LM, Hohaus S. CD68+ cell count, early evaluation with PET and
plasma TARC levels predict response in Hodgkin lymphoma. Cancer Med.
2016;5:398-406. https://doi.org/10.1002/cam4.585 PMid:26758564 PMCid:PMC4799945
- Hohaus
S, Giachelia M, Massini G, Vannata B, Criscuolo M, Martini M, D'Alo' F,
Voso MT, Larocca LM, Leone G. Clinical significance of interleukin-10
gene polymorphisms and plasma levels in Hodgkin lymphoma. Leuk Res.
2009;33:1352-6. https://doi.org/10.1016/j.leukres.2009.01.009 PMid:19201467
- Advani
RH, Kelsey CR, Armand P, Bello CM, Benitez CM, Bond D, Chen W, Cherian
S, Czader M, Dabaja B, Daly ME, Frosch Z, Gordon LI, Hansen N, Herrera
AF, Hochberg EP, Hoppe RT, Isufi I, Johnston PB, Kelly K, Kenkre VP,
Kline J, Lynch RC, McConathy J, Morgan D, Niu A, Paul S, Rabinovitch R,
Salavati A, Sano D, Shah H, Spinner M, Svoboda J, Winter JN, Yahalom J,
Yang JC, Montgomery S, Stehman K. Hodgkin Lymphoma, Version 1.2026,
NCCN Clinical Practice Guidelines In Oncology. J Natl Compr Canc Netw.
2026;24:41-60. https://doi.org/10.6004/jnccn.2026.0006 PMid:41671432
- Eyre
TA, Cwynarski K, d'Amore F, de Leval L, Dreyling M, Eichenauer DA,
Ferreri AJM, Giné E, Kersten MJ, Ladetto M, Specht L, Thieblemont C,
Walewski J, Zucca E, Jerkeman M; ESMO Guidelines Committee. Electronic
address: clinicalguidelines@esmo.org. Lymphomas: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2025;36:1263-84. https://doi.org/10.1016/j.annonc.2025.07.014 PMid:40774601
- Younes
A, Gopal AK, Smith SE, Ansell SM, Rosenblatt JD, Savage KJ, Ramchandren
R, Bartlett NL, Cheson BD, de Vos S, Forero-Torres A, Moskowitz CH,
Connors JM, Engert A, Larsen EK, Kennedy DA, Sievers EL, Chen R.
Results of a pivotal phase II study of brentuximab vedotin for patients
with relapsed or refractory Hodgkin's lymphoma. J Clin Oncol.
2012;30:2183-9. https://doi.org/10.1200/JCO.2011.38.0410 PMid:22454421 PMCid:PMC3646316
- Ansell
SM, Bröckelmann PJ, von Keudell G, Lee HJ, Santoro A, Zinzani PL,
Collins GP, Cohen JB, de Boer JP, Kuruvilla J, Savage KJ, Trněný M,
Provencio M, Jäger U, Willenbacher W, Wen R, Akyol A, Mikita-Geoffroy
J, Shipp MA, Engert A, Armand P. Nivolumab for relapsed/refractory
classical Hodgkin lymphoma: 5-year survival from the pivotal phase 2
CheckMate 205 study. Blood Adv. 2023;7:6266-74. https://doi.org/10.1182/bloodadvances.2023010334 PMid:37530622 PMCid:PMC10589773
- Armand
P, Zinzani PL, Lee HJ, Johnson NA, Brice P, Radford J, Ribrag V, Molin
D, Vassilakopoulos TP, Tomita A, von Tresckow B, Shipp MA, Herrera AF,
Lin J, Kim E, Chakraborty S, Marinello P, Moskowitz CH. Five-year
follow-up of KEYNOTE-087: pembrolizumab monotherapy for
relapsed/refractory classical Hodgkin lymphoma. Blood. 2023;142:878-86.
https://doi.org/10.1182/blood.2022019386 PMid:37319435 PMCid:PMC10624931
- Engert
A, Plütschow A, Eich HT, Lohri A, Dörken B, Borchmann P, Berger B,
Greil R, Willborn KC, Wilhelm M, Debus J, Eble MJ, Sökler M, Ho A, Rank
A, Ganser A, Trümper L, Bokemeyer C, Kirchner H, Schubert J, Král Z,
Fuchs M, Müller-Hermelink HK, Müller RP, Diehl V. Reduced treatment
intensity in patients with early-stage Hodgkin's lymphoma. N Engl J
Med. 2010;363:640-52. https://doi.org/10.1056/NEJMoa1000067 PMid:20818855
- Sasse
S, Bröckelmann PJ, Goergen H, Plütschow A, Müller H, Kreissl S, Buerkle
C, Borchmann S, Fuchs M, Borchmann P, Diehl V, Engert A. Long-Term
Follow-Up of Contemporary Treatment in Early-Stage Hodgkin Lymphoma:
Updated Analyses of the German Hodgkin Study Group HD7, HD8, HD10, and
HD11 Trials. J Clin Oncol. 2017;35:1999-2007. https://doi.org/10.1200/JCO.2016.70.9410 PMid:28418763
- Radford
J, Illidge T, Counsell N, Hancock B, Pettengell R, Johnson P, Wimperis
J, Culligan D, Popova B, Smith P, McMillan A, Brownell A, Kruger A,
Lister A, Hoskin P, O'Doherty M, Barrington S. Results of a trial of
PET-directed therapy for early-stage Hodgkin's lymphoma. N Engl J Med.
2015;372:1598-607. https://doi.org/10.1056/NEJMoa1408648 PMid:25901426
- Radford
J, Williams J, Edwards D, Pettengell R, Johnson P, Hoskin P, Illidge T,
Counsell N Involved Field Radiotherapy Versus No Further Treatment in
Patients with Newly Diagnosed Stage 1A or 2A Hodgkin Lymphoma and a
'Negative' PET Scan after 3 Cycles ABVD. Survival and Cause of Death
after a Median of 16 Years Follow-up in the UK RAPID Trial. Blood.
2024;144 (Supplement 1): 457. https://doi.org/10.1182/blood-2024-200662
- Versari
A, Hutchings M, Meignan M, Raemaekers J. Early Positron Emission
Tomography Response-Adapted Treatment in Stage I and II Hodgkin
Lymphoma: Final Results of the Randomized EORTC/LYSA/FIL H10 Trial. J
Clin Oncol. 2017;35:1786-94. https://doi.org/10.1200/JCO.2016.68.6394 PMid:28291393 PMCid:PMC10905319
- Federico
M, Fortpied C, Stepanishyna Y, Gotti M, van der Maazen R, Cristinelli
C, Re A, Plattel W, Lazarovici J, Merli F, Specht L, Schiano de Colella
JM, Hutchings M, Versari A, Edeline V, Stamatoulas A, Girinsky T,
Ricardi U, Aleman B, Meulemans B, Tonino S, Raemaekers J, André M.
Long-Term Follow-Up of the Response-Adapted Intergroup EORTC/LYSA/FIL
H10 Trial for Localized Hodgkin Lymphoma. J Clin Oncol. 2024;42:19-25. https://doi.org/10.1200/JCO.23.01745 PMid:37967311 PMCid:PMC10730029
- Fuchs
M, Goergen H, Kobe C, Kuhnert G, Lohri A, Greil R, Sasse S, Topp MS,
Schäfer E, Hertenstein B, Soekler M, Vogelhuber M, Zijlstra JM, Keller
UB, Krause SW, Wilhelm M, Maschmeyer G, Thiemer J, Dührsen U, Meissner
J, Viardot A, Eich H, Baues C, Diehl V, Rosenwald A, von Tresckow B,
Dietlein M, Borchmann P, Engert A. Positron Emission Tomography-Guided
Treatment in Early-Stage Favorable Hodgkin Lymphoma: Final Results of
the International, Randomized Phase III HD16 Trial by the German
Hodgkin Study Group. J Clin Oncol. 2019;37:2835-45. https://doi.org/10.1200/JCO.19.00964 PMid:31498753
- Fuchs
M, Jacob AS, Kaul H, Kobe C, Kuhnert G, Pabst T, Greil R, Bröckelmann
PJ, Topp MS, Just M, Hertenstein B, Soekler M, Vogelhuber M, Zijlstra
JM, Keller UB, Krause SW, Dührsen U, Meissner J, Viardot A, Eich HT,
Baues C, Diehl V, Rosenwald A, Buehnen I, von Tresckow B, Dietlein M,
Borchmann P, Engert A, Eichenauer DA. Follow-up of the GHSG HD16 trial
of PET-guided treatment in early-stage favorable Hodgkin lymphoma.
Leukemia. 2024;38:160-7. https://doi.org/10.1038/s41375-023-02064-y PMid:37845285 PMCid:PMC10776396
- Eich
HT, Diehl V, Görgen H, Pabst T, Markova J, Debus J, Ho A, Dörken B,
Rank A, Grosu AL, Wiegel T, Karstens JH, Greil R, Willich N,
Schmidberger H, Döhner H, Borchmann P, Müller-Hermelink HK, Müller RP,
Engert A. Intensified chemotherapy and dose-reduced involved-field
radiotherapy in patients with early unfavorable Hodgkin's lymphoma:
final analysis of the German Hodgkin Study Group HD11 trial. J Clin
Oncol. 2010;28:4199-206. https://doi.org/10.1200/JCO.2010.29.8018 PMid:20713848
- Borchmann
P, Plütschow A, Kobe C, Greil R, Meissner J, Topp MS, Ostermann H,
Dierlamm J, Mohm J, Thiemer J, Sökler M, Kerkhoff A, Ahlborn M,
Halbsguth TV, Martin S, Keller U, Balabanov S, Pabst T, Vogelhuber M,
Hüttmann A, Wilhelm M, Zijlstra JM, Moccia A, Kuhnert G, Bröckelmann
PJ, von Tresckow B, Fuchs M, Klimm B, Rosenwald A, Eich H, Baues C,
Marnitz S, Hallek M, Diehl V, Dietlein M, Engert A. PET-guided omission
of radiotherapy in early-stage unfavourable Hodgkin lymphoma (GHSG
HD17): a multicentre, open-label, randomised, phase 3 trial. Lancet
Oncol. 2021;22:223-34. https://doi.org/10.1016/S1470-2045(20)30601-X PMid:33539742 PMCid:PMC8458171
- Abramson
JS, Arnason JE, LaCasce AS, Redd R, Barnes JA, Sokol L, Joyce R, Avigan
D, Neuberg D, Takvorian RW, Hochberg EP, Bello CM. Brentuximab vedotin,
doxorubicin, vinblastine, and dacarbazine for nonbulky limited-stage
classical Hodgkin lymphoma. Blood. 2019;134:606-13. https://doi.org/10.1182/blood.2019001272 PMid:31186274
- Abramson
JS, Bengston E, Redd R, Barnes JA, Takvorian T, Sokol L, Lansigan F,
Armand P, Shah B, Jacobsen E, Martignetti R, Turba E, Metzler S,
Patterson V, LaCasce AS, Bello CM. Brentuximab vedotin plus doxorubicin
and dacarbazine in nonbulky limited-stage classical Hodgkin lymphoma.
Blood Adv. 2023;7:1130-36. https://doi.org/10.1182/bloodadvances.2022008420 PMid:36053786 PMCid:PMC10111342
- Fornecker
LM, Lazarovici J, Aurer I, Casasnovas RO, Gac AC, Bonnet C, Bouabdallah
K, Feugier P, Specht L, Molina L, Touati M, Borel C, Stamatoullas A,
Nicolas-Virelizier E, Pascal L, Lugtenburg P, Di Renzo N, Vander Borght
T, Traverse-Glehen A, Dartigues P, Hutchings M, Versari A, Meignan M,
Federico M, André M; LYSA-FIL-EORTC Intergroup. Brentuximab Vedotin
Plus AVD for First-Line Treatment of Early-Stage Unfavorable Hodgkin
Lymphoma (BREACH): A Multicenter, Open-Label, Randomized, Phase II
Trial. J Clin Oncol. 2023;41:327-335. https://doi.org/10.1200/JCO.21.01281 PMid:35867960
- Bröckelmann
PJ, Bühnen I, Meissner J, Trautmann-Grill K, Herhaus P, Halbsguth TV,
Schaub V, Kerkhoff A, Mathas S, Bormann M, Dickhut A, Kaul H, Fuchs M,
Kobe C, Baues C, Borchmann P, Engert A, von Tresckow B. Nivolumab and
Doxorubicin, Vinblastine, and Dacarbazine in Early-Stage Unfavorable
Hodgkin Lymphoma: Final Analysis of the Randomized German Hodgkin Study
Group Phase II NIVAHL Trial. J Clin Oncol. 2023;41:1193-99. https://doi.org/10.1200/JCO.22.02355 PMid:36508302
- Abramson
JS, Straus DJ, Bartlett NL, Burke JM, Lynch RC, Domingo-Domenech E,
Hess BT, Schuster SR, Linhares Y, Gandhi MD, Shah HR, Jurczak W, Re A,
Hahn U, Prince HM, Guo W, Davis G, Ho L, Fanale M, Yasenchak CA, Lee
HJJ. Brentuximab Vedotin and Nivolumab in Combination With Chemotherapy
for Nonbulky, Early-Stage Classical Hodgkin Lymphoma. Blood.
2026;147:1713-22. https://doi.org/10.1182/blood.2025030190 PMid:41460964 PMCid:PMC13077476
- André
MPE, Carde P, Viviani S, Bellei M, Fortpied C, Hutchings M, Gianni AM,
Brice P, Casasnovas O, Gobbi PG, Zinzani PL, Dupuis J, Iannitto E,
Rambaldi A, Brière J, Clément-Filliatre L, Heczko M, Valagussa P,
Douxfils J, Depaus J, Federico M, Mounier N. Long-term overall survival
and toxicities of ABVD vs BEACOPP in advanced Hodgkin lymphoma: A
pooled analysis of four randomized trials. Cancer Med. 2020;9:6565-75. https://doi.org/10.1002/cam4.3298 PMid:32710498 PMCid:PMC7520354
- Johnson
P, Federico M, Kirkwood A, Fosså A, Berkahn L, Carella A, d'Amore F,
Enblad G, Franceschetto A, Fulham M, Luminari S, O'Doherty M, Patrick
P, Roberts T, Sidra G, Stevens L, Smith P, Trotman J, Viney Z, Radford
J, Barrington S. Adapted Treatment Guided by Interim PET-CT Scan in
Advanced Hodgkin's Lymphoma. N Engl J Med. 2016;374:2419-29. https://doi.org/10.1056/NEJMoa1510093 PMid:27332902 PMCid:PMC4961236
- Luminari
S, Fossa A, Trotman J, Molin D, d'Amore F, Enblad G, Berkahn L,
Barrington SF, Radford J, Federico M, Kirkwood AA, Johnson PWM
Long-Term Follow-Up of the Response-Adjusted Therapy for Advanced
Hodgkin Lymphoma Trial. J Clin Oncol. 2024;42:13-18. https://doi.org/10.1200/JCO.23.01177 PMid:37883739 PMCid:PMC10730066
- Casasnovas
RO, Bouabdallah R, Brice P, Lazarovici J, Ghesquieres H, Stamatoullas
A, Dupuis J, Gac AC, Gastinne T, Joly B, Bouabdallah K,
Nicolas-Virelizier E, Feugier P, Morschhauser F, Sibon D, Bonnet C,
Berriolo-Riedinger A, Edeline V, Parrens M, Damotte D, Coso D, André M,
Meignan M, Rossi C. Positron Emission Tomography-Driven Strategy in
Advanced Hodgkin Lymphoma: Prolonged Follow-Up of the AHL2011 Phase III
Lymphoma Study Association Study. J Clin Oncol. 2022;40:1091-101. https://doi.org/10.1200/JCO.21.01777 PMid:34990281
- Borchmann
P, Goergen H, Kobe C, Lohri A, Greil R, Eichenauer DA, Zijlstra JM,
Markova J, Meissner J, Feuring-Buske M, Hüttmann A, Dierlamm J, Soekler
M, Beck HJ, Willenbacher W, Ludwig WD, Pabst T, Topp MS, Hitz F, Bentz
M, Keller UB, Kühnhardt D, Ostermann H, Schmitz N, Hertenstein B,
Aulitzky W, Maschmeyer G, Vieler T, Eich H, Baues C, Stein H, Fuchs M,
Kuhnert G, Diehl V, Dietlein M, Engert A. PET-guided treatment in
patients with advanced-stage Hodgkin's lymphoma (HD18): final results
of an open-label, international, randomised phase 3 trial by the German
Hodgkin Study Group. Lancet. 2017;390:2790-802. https://doi.org/10.1016/S0140-6736(17)32134-7 PMid:29061295
- Josephson
NC, Song E, Sachs J, Liu R, Jolin HA, Huebner D, Radford J; ECHELON-1
Study Group. Brentuximab Vedotin with Chemotherapy for Stage III or IV
Hodgkin's Lymphoma. N Engl J Med. 2018;378:331-344. https://doi.org/10.1056/NEJMoa1708984 PMid:29224502 PMCid:PMC5819601
- Ansell
SM, Radford J, Connors JM, Długosz-Danecka M, Kim WS, Gallamini A,
Ramchandren R, Friedberg JW, Advani R, Hutchings M, Evens AM, Smolewski
P, Savage KJ, Bartlett NL, Eom HS, Abramson JS, Dong C, Campana F,
Fenton K, Puhlmann M, Straus DJ; ECHELON-1 Study Group. Overall
Survival with Brentuximab Vedotin in Stage III or IV Hodgkin's
Lymphoma. N Engl J Med. 2022;387:310-20. https://doi.org/10.1056/NEJMoa2206125 PMid:35830649
- Ansell
SM, Straus DJ, Connors JM, Jurczak W, Kim WS, Gallamini A, Ramchandren
R, Friedberg JW, Advani RH, Hutchings M, Evens AM, Savage KJ, Eom HS,
Feldman TA, Abramson JS, Dong C, Savani BN, Zomas A, Fenton K, Radford
J. Seven-year overall survival analysis from ECHELON-1 study of A+AVD
versus ABVD in patients with previously untreated stage III/IV
classical Hodgkin lymphoma. J Clin Oncol. 2024; 42(16_suppl.):7053 https://doi.org/10.1200/JCO.2024.42.16_suppl.7053
- Borchmann
P, Ferdinandus J, Schneider G, Moccia A, Greil R, Hertzberg M, Schaub
V, Hüttmann A, Keil F, Dierlamm J, Hänel M, Novak U, Meissner J,
Zimmermann A, Mathas S, Zijlstra JM, Fosså A, Viardot A, Hertenstein B,
Martin S, Giri P, Scholl S, Topp MS, Jung W, Vucinic V, Beck HJ,
Kerkhoff A, Unger B, Rank A, Schroers R, Zum Büschenfelde CM, de Wit M,
Trautmann-Grill K, Kamper P, Molin D, Kreissl S, Kaul H, von Tresckow
B, Borchmann S, Behringer K, Fuchs M, Rosenwald A, Klapper W, Eich HT,
Baues C, Zomas A, Hallek M, Dietlein M, Kobe C, Diehl V; German Hodgkin
Study Group; Swiss Group for Clinical Cancer Research;
Arbeitsgemeinschaft Medikamentöse Tumortherapie; Nordic Lymphoma Group;
Australasian Leukaemia and Lymphoma Group. Assessing the efficacy and
tolerability of PET-guided BrECADD versus eBEACOPP in advanced-stage,
classical Hodgkin lymphoma (HD21): a randomised, multicentre, parallel,
open-label, phase 3 trial. Lancet. 2024;404:341-52. https://doi.org/10.1016/S0140-6736(24)01315-1 PMid:38971175
- Herrera
AF, LeBlanc M, Castellino SM, Li H, Rutherford SC, Evens AM, Davison K,
Punnett A, Parsons SK, Ahmed S, Casulo C, Bartlett NL, Tuscano JM, Mei
MG, Hess BT, Jacobs R, Saeed H, Torka P, Hu B, Moskowitz C, Kaur S,
Goyal G, Forlenza C, Doan A, Lamble A, Kumar P, Chowdhury S, Brinker B,
Sharma N, Singh A, Blum KA, Perry AM, Kovach AE, Hodgson D, Constine
LS, Shields LK, Prica A, Dillon H, Little RF, Shipp MA, Crump M, Kahl
B, Leonard JP, Smith SM, Song JY, Kelly KM, Friedberg JW. Nivolumab+AVD
in Advanced-Stage Classic Hodgkin's Lymphoma. N Engl J Med. 2024 Oct
17;391(15):1379-1389. doi: 10.1056/NEJMoa2405888. https://doi.org/10.1056/NEJMoa2405888 PMid:39413375 PMCid:PMC11488644
- Allen
PB, Savas H, Evens AM, Advani RH, Palmer B, Pro B, Karmali R, Mou E,
Bearden J, Dillehay G, Bayer RA, Eisner RM, Chmiel JS, O'Shea K, Gordon
LI, Winter JN. Pembrolizumab followed by AVD in untreated early
unfavorable and advanced-stage classical Hodgkin lymphoma. Blood.
2021;137:1318-26. https://doi.org/10.1182/blood.2020007400 PMid:32992341 PMCid:PMC7955404
- Lynch
RC, Ujjani CS, Poh C, Warren EH, Smith SD, Shadman M, Till B,
Raghunathan VM, Alig S, Alizadeh AA, Gulhane A, Chen DL, Tseng Y, Coye
H, Shelby M, Ottemiller S, Keo S, Verni K, Du H, Vandermeer J, Gaston
A, Rasmussen H, Martin P, Marzbani E, Voutsinas J, Gopal AK. Concurrent
pembrolizumab with AVD for untreated classic Hodgkin lymphoma.
Blood.;141:2576-86.
- Lee
HJ, Ramchandren R, Friedman J, Melear J, Flinn IW, Burke JM, Linhares
Y, Gonzales P, Peterson M, Raval M, Chintapatla R, Feldman TA, Yimer H,
Islas-Ohlmayer M, Patel A, Metheny L, Dean A, Rana V, Gandhi MD,
Renshaw J, Ho L, Fanale MA, Guo W, Yasenchak CA. Brentuximab vedotin,
nivolumab, doxorubicin, and dacarbazine for advanced-stage classical
Hodgkin lymphoma. Blood. 2025;145:290-99. https://doi.org/10.1182/blood.2024024681 PMid:39622165
- Park CH, Cho H, Kim SJ. Treatment of older patients with Hodgkin lymphoma. Blood Res. 2025;60:35. https://doi.org/10.1007/s44313-025-00084-4 PMid:40504313 PMCid:PMC12162405
- Merli
F, Luminari S, Tucci A, Arcari A, Rigacci L, Hawkes E, Chiattone CS,
Cavallo F, Cabras G, Alvarez I, Fabbri A, Re A, Puccini B, Barraclough
A, Delamain MT, Ferrero S, Usai SV, Ferrari A, Cencini E, Pennese E,
Zilioli VR, Marino D, Balzarotti M, Cox MC, Zanni M, Di Rocco A, Lleshi
A, Botto B, Hohaus S, Merli M, Sartori R, Gini G, Nassi L, Musuraca G,
Tani M, Bottelli C, Kovalchuk S, Re F, Flenghi L, Molinari A, Tarantini
G, Chimienti E, Marcheselli L, Mammi C, Spina M. Simplified geriatric
assessment in older patients with diffuse large B- cell lymphoma: the
prospective elderly project of the Fondazione Italiana Linfomi. J Clin
Oncol. 2021;39:1214-22. https://doi.org/10.1200/JCO.20.02465 PMid:33577377
- Zilioli
VR, Tucci A, Spina M, Merli F, Arcari A; Elderly Lymphoma Committee of
the Fondazione Italiana Linfomi. The importance of assessing the
fitness of older patients with newly diagnosed diffuse large B-cell
lymphoma and classic Hodgkin lymphoma. Br J Haematol. 2026;208:58-66. https://doi.org/10.1111/bjh.70290 PMid:41449752 PMCid:PMC12819097
- Salvi
F, Luminari S, Tucci A, Massidda S, Liberati AM, Stelitano C, Zanni M,
Re A, Centurioni R, Freilone R, Musuraca G, Nassi L, Patti C, Arcari A,
Tani M, Pulsoni A, Pavone V, Volpetti S, Peli A, Evangelista A, Spina
M, Ladetto M, Merli F. Bleomycin, vinblastine and dacarbazine combined
with nonpegylated liposomal doxorubicin (MBVD) in elderly ( 70 years)
or cardiopathic patients with Hodgkin lymphoma: a phase-II study from
Fondazione Italiana Linfomi (FIL). Leuk Lymphoma. 2019;60:2890-98. https://doi.org/10.1080/10428194.2019.1608529 PMid:31282794
- Böll
B, Bredenfeld H, Görgen H, Halbsguth T, Eich HT, Soekler M, Markova J,
Keller U, Graeven U, Kremers S, Geissler M, Trenn G, Fuchs M, von
Tresckow B, Eichenauer DA, Borchmann P, Engert A. Phase 2 study of PVAG
(prednisone, vinblastine, doxorubicin, gemcitabine) in elderly patients
with early unfavorable or advanced stage Hodgkin lymphoma. Blood.
2011;118:6292-8. https://doi.org/10.1182/blood-2011-07-368167 PMid:21917759
- Straus
DJ, Johnson JL, LaCasce AS, Bartlett NL, Kostakoglu L, Hsi ED, Schöder
H, Hall NC, Jung SH, Canellos GP, Schwartz LH, Takvorian RW, Juweid ME,
Cheson BD; Cancer and Leukemia Group B. Doxorubicin, vinblastine, and
gemcitabine (CALGB 50203) for stage I/II nonbulky Hodgkin lymphoma:
pretreatment prognostic factors and interim PET. Blood.
2011;117:5314-20. https://doi.org/10.1182/blood-2010-10-314260 PMid:21355087 PMCid:PMC3109706
- Ghesquières
H, Krzisch D, Nicolas-Virelizier E, Kanoun S, Gac AC, Guidez S, Touati
M, Laribi K, Morschhauser F, Bonnet C, Waultier-Rascalou A,
Orsini-Piocelle F, André M, Fournier M, Morand F, Berriolo-Riedinger A,
Burroni B, Damotte D, Traverse-Glehen A, Quittet P, Casasnovas O. The
phase 2 LYSA study of prednisone, vinblastine, doxorubicin, and
bendamustine for untreated Hodgkin lymphoma in older patients. Blood.
2024;143:983-95. https://doi.org/10.1182/blood.2023021564 PMid:37979133
- Forero-Torres
A, Holkova B, Goldschmidt J, Chen R, Olsen G, Boccia RV, Bordoni RE,
Friedberg JW, Sharman JP, Palanca-Wessels MC, Wang Y, Yasenchak CA.
Phase 2 study of frontline brentuximab vedotin monotherapy in Hodgkin
lymphoma patients aged 60 years and older. Blood. 2015;126:2798-804. https://doi.org/10.1182/blood-2015-06-644336 PMid:26377597 PMCid:PMC4692140
- Gibb
A, Pirrie SJ, Linton K, Warbey V, Paterson K, Davies AJ, Collins GP,
Menne T, McKay P, Fields PA, Miall FM, Nagy E, Wheatley K, Reed R,
Baricevic-Jones I, Barrington S, Radford J. Results of a UK National
Cancer Research Institute Phase II study of brentuximab vedotin using a
response-adapted design in the first-line treatment of patients with
classical Hodgkin lymphoma unsuitable for chemotherapy due to age,
frailty or comorbidity (BREVITY). Br J Haematol. 2021;193:63-71. https://doi.org/10.1111/bjh.17073 PMid:32926420
- Friedberg
JW, Forero-Torres A, Bordoni RE, Cline VJM, Patel Donnelly D, Flynn PJ,
Olsen G, Chen R, Fong A, Wang Y, Yasenchak CA. Frontline brentuximab
vedotin in combination with dacarbazine or bendamustine in patients
aged ≥60 years with HL. Blood. 2017;130:2829-37. https://doi.org/10.1182/blood-2017-06-787200 PMid:29038340
- Evens
AM, Connors JM, Younes A, Ansell SM, Kim WS, Radford J, Feldman T,
Tuscano J, Savage KJ, Oki Y, Grigg A, Pocock C, Dlugosz-Danecka M,
Fenton K, Forero-Torres A, Liu R, Jolin H, Gautam A, Gallamini A. Older
patients (aged 60 years) with previously untreated advanced-stage
classical Hodgkin lymphoma: a detailed analysis from the phase III
ECHELON-1 study. Haematologica. 2022;107:1086-94. https://doi.org/10.3324/haematol.2021.278438 PMid:34162178 PMCid:PMC9052913
- Evens
AM, Advani RH, Helenowski IB, Fanale M, Smith SM, Jovanovic BD, Bociek
GR, Klein AK, Winter JN, Gordon LI, Hamlin PA. Multicenter Phase II
Study of Sequential Brentuximab Vedotin and Doxorubicin, Vinblastine,
and Dacarbazine Chemotherapy for Older Patients With Untreated
Classical Hodgkin Lymphoma. J Clin Oncol. 2018;36:3015-22. https://doi.org/10.1200/JCO.2018.79.0139 PMid:30179569
- Ferdinandus
J, Kaul H, Fosså A, Hüttmann A, Keil F, Ko YD, Hitz F, Schwarz M,
Trenker C, Kerkhoff A, Staib P, Wille K, Dresel I, Hahn D, Hertenstein
B, Moosmann P, Mey U, Balabanov S, Armytage T, Roncolato F, Hellmuth
JC, Kreissl S, Fuchs M, Schneider G, Tharmaseelan H, Eichenauer DA, von
Tresckow B, Borchmann P, Bröckelman PJ. PET-Guided Brecadd in Older
Patients with Advanced-Stage Classic Hodgkin Lymphoma: Results of the
Phase 2 Part of the GHSG HD21 Trial. Blood. 2024;144(Supplement 1):568.
https://doi.org/10.1182/blood-2024-207946
- Rutherford
SC, Li H, Herrera AF, LeBlanc M, Ahmed S, Davison K, Parsons SK, Unger
JM, Perry AM, Casulo C, Bartlett NL, Tuscano JM, Hess BT, Torka P,
Kumar P, Jacobs R, Song JY, Castellino SM, Kahl B, Leonard JP, Smith
SM, Friedberg JW, Evens AM. Nivolumab-AVD Versus Brentuximab
Vedotin-AVD in Older Patients With Advanced-Stage Classic Hodgkin
Lymphoma Enrolled on S1826. J Clin Oncol. 2025;43:2968-73. https://doi.org/10.1200/JCO-25-00204 PMid:40523203 PMCid:PMC12353409
- Cheson
BD, Bartlett NL, LaPlant B, Lee HJ, Advani RJ, Christian B, Diefenbach
CS, Feldman TA, Ansell SM. Brentuximab vedotin plus nivolumab as
first-line therapy in older or chemotherapy-ineligible patients with
Hodgkin lymphoma (ACCRU): a multicentre, single-arm, phase 2 trial.
Lancet Haematol. 2020;7:e808-e815. https://doi.org/10.1016/S2352-3026(20)30275-1 PMid:33010817
- Friedberg
JW, Bordoni R, Patel-Donnelly D, Larson T, Goldschmidt J, Boccia R,
Cline VJM, Mamidipalli A, Liu J, Akyol A, Yasenchak CA. Brentuximab
vedotin with dacarbazine or nivolumab as frontline cHL therapy for
older patients ineligible for chemotherapy. Blood. 2024;143:786-95. https://doi.org/10.1182/blood.2022019536 PMid:37946283
- Castagna
L, Carlo-Stella C, Mazza R, Santoro A. Current role of autologous and
allogeneic stem cell transplantation for relapsed and refractory
hodgkin lymphoma. Mediterr J Hematol Infect Dis. 2015;7:e2015015. https://doi.org/10.4084/mjhid.2015.015 PMid:25745542 PMCid:PMC4344175
- Devillier
R, Coso D, Castagna L, Brenot Rossi I, Anastasia A, Chiti A, Ivanov V,
Schiano JM, Santoro A, Chabannon C, Balzarotti M, Blaise D, Bouabdallah
R. Positron emission tomography response at the time of autologous stem
cell transplantation predicts outcome of patients with relapsed and/or
refractory Hodgkin's lymphoma responding to prior salvage therapy.
Haematologica. 2012;97:1073-9. https://doi.org/10.3324/haematol.2011.056051 PMid:22271893 PMCid:PMC3396680
- Moskowitz
CH, Matasar MJ, Zelenetz AD, Nimer SD, Gerecitano J, Hamlin P, Horwitz
S, Moskowitz AJ, Noy A, Palomba L, Perales MA, Portlock C, Straus D,
Maragulia JC, Schoder H, Yahalom J. Normalization of pre-ASCT, FDG-PET
imaging with second-line, non-cross-resistant, chemotherapy programs
improves event-free survival in patients with Hodgkin lymphoma. Blood.
2012;119:1665-70. https://doi.org/10.1182/blood-2011-10-388058 PMid:22184409 PMCid:PMC3790950
- Castagna
L, Santoro A, Carlo-Stella C. Salvage Therapy for Hodgkin's Lymphoma: A
Review of Current Regimens and Outcomes. J Blood Med. 2020;11:389-403. https://doi.org/10.2147/JBM.S250581 PMid:33149713 PMCid:PMC7603406
- Luttwak E, Moskowitz AJ. What is the best salvage therapy for Hodgkin lymphoma? Curr Opin Oncol. 2024;36:346-52. https://doi.org/10.1097/CCO.0000000000001073 PMid:39007229
- Josting
A, Rudolph C, Reiser M, Mapara M, Sieber M, Kirchner HH, Dörken B,
Hossfeld DK, Diehl V, Engert A; Participating Centers. Time-intensified
dexamethasone/cisplatin/cytarabine: an effective salvage therapy with
low toxicity in patients with relapsed and refractory Hodgkin's
disease. Ann Oncol. 2002;13:1628-35. https://doi.org/10.1093/annonc/mdf221 PMid:12377653
- Labrador
J, Cabrero-Calvo M, Pérez-López E, Mateos MV, Vázquez L, Caballero MD,
García-Sanz R. ESHAP as salvage therapy for relapsed or refractory
Hodgkin's lymphoma. Ann Hematol. 2014;93:1745-53. https://doi.org/10.1007/s00277-014-2114-0 PMid:24863692
- Baetz
T, Belch A, Couban S, Imrie K, Yau J, Myers R, Ding K, Paul N, Shepherd
L, Iglesias J, Meyer R, Crump M. Gemcitabine, dexamethasone and
cisplatin is an active and non-toxic chemotherapy regimen in relapsed
or refractory Hodgkin's disease: a phase II study by the National
Cancer Institute of Canada Clinical Trials Group. Ann Oncol.
2003;14:1762-7. https://doi.org/10.1093/annonc/mdg496 PMid:14630682
- Gokmen
A, Sahin U, Soydan E, Gokgoz Z, Okcu MK, Ozan U, Arslan O, Ilhan O,
Ozcan M. Gemcitabine, Cisplatin, and Dexamethasone as a Salvage and
Mobilization Chemotherapy Before Autologous Stem Cell Transplantation
is Effective and Safe Outpatient Regimen in Relapsed and Refractory
Hodgkin Lymphoma Patients. Clin Lymphoma Myeloma Leuk.
2022;22:e885-e892. https://doi.org/10.1016/j.clml.2022.06.015 PMid:35927182
- Bartlett
NL, Niedzwiecki D, Johnson JL, Friedberg JW, Johnson KB, van Besien K,
Zelenetz AD, Cheson BD, Canellos GP; Cancer Leukemia Group B.
Gemcitabine, vinorelbine, and pegylated liposomal doxorubicin (GVD), a
salvage regimen in relapsed Hodgkin's lymphoma: CALGB 59804. Ann Oncol.
2007;18:1071-9. https://doi.org/10.1093/annonc/mdm090 PMid:17426059
- Moskowitz
CH, Nimer SD, Zelenetz AD, Trippett T, Hedrick EE, Filippa DA, Louie D,
Gonzales M, Walits J, Coady-Lyons N, Qin J, Frank R, Bertino JR, Goy A,
Noy A, O'Brien JP, Straus D, Portlock CS, Yahalom J. A 2-step
comprehensive high-dose chemoradiotherapy second-line program for
relapsed and refractory Hodgkin disease: analysis by intent to treat
and development of a prognostic model. Blood. 2001;97:616-23. https://doi.org/10.1182/blood.V97.3.616 PMid:11157476
- Santoro
A, Magagnoli M, Spina M, Pinotti G, Siracusano L, Michieli M, Nozza A,
Sarina B, Morenghi E, Castagna L, Tirelli U, Balzarotti M. Ifosfamide,
gemcitabine, and vinorelbine: a new induction regimen for refractory
and relapsed Hodgkin's lymphoma. Haematologica. 2007 Jan;92:35-41. https://doi.org/10.3324/haematol.10661 PMid:17229633
- Santoro
A, Mazza R, Pulsoni A, Re A, Bonfichi M, Zilioli VR, Salvi F, Merli F,
Anastasia A, Luminari S, Annechini G, Gotti M, Peli A, Liberati AM, Di
Renzo N, Castagna L, Giordano L, Carlo-Stella C. Bendamustine in
Combination With Gemcitabine and Vinorelbine Is an Effective Regimen As
Induction Chemotherapy Before Autologous Stem-Cell Transplantation for
Relapsed or Refractory Hodgkin Lymphoma: Final Results of a Multicenter
Phase II Study. J Clin Oncol. 2016;34:3293-9. https://doi.org/10.1200/JCO.2016.66.4466 PMid:27382096
- Santoro
A, Mazza R, Pulsoni A, Re A, Bonfichi M, Zilioli VR, Zanni M, Merli F,
Anastasia A, Luminari S, Annechini G, Gotti M, Peli A, Liberati AM, Di
Renzo N, Castagna L, Giordano L, Ricci F, Carlo-Stella C. Five-year
results of the BEGEV salvage regimen in relapsed/refractory classical
Hodgkin lymphoma. Blood Adv. 2020;4:136-40. https://doi.org/10.1182/bloodadvances.2019000984 PMid:31935284 PMCid:PMC6960479
- Chen
R, Gopal AK, Smith SE, Ansell SM, Rosenblatt JD, Savage KJ, Connors JM,
Engert A, Larsen EK, Huebner D, Fong A, Younes A. Five-year survival
and durability results of brentuximab vedotin in patients with relapsed
or refractory Hodgkin lymphoma. Blood. 2016;128:1562-6. https://doi.org/10.1182/blood-2016-02-699850 PMid:27432875 PMCid:PMC5034737
- Moskowitz
CH, Nademanee A, Masszi T, Agura E, Holowiecki J, Abidi MH, Chen AI,
Stiff P, Gianni AM, Carella A, Osmanov D, Bachanova V, Sweetenham J,
Sureda A, Huebner D, Sievers EL, Chi A, Larsen EK, Hunder NN, Walewski
J; AETHERA Study Group. Brentuximab vedotin as consolidation therapy
after autologous stem-cell transplantation in patients with Hodgkin's
lymphoma at risk of relapse or progression (AETHERA): a randomised,
double-blind, placebo-controlled, phase 3 trial. Lancet.
2015;385:1853-62. https://doi.org/10.1016/S0140-6736(15)60165-9 PMid:25796459
- Moskowitz
CH, Walewski J, Nademanee A, Masszi T, Agura E, Holowiecki J, Abidi MH,
Chen AI, Stiff P, Viviani S, Bachanova V, Sureda A, McClendon T, Lee C,
Lisano J, Sweetenham J. Five-year PFS from the AETHERA trial of
brentuximab vedotin for Hodgkin lymphoma at high risk of progression or
relapse. Blood. 2018;132:2639-42. https://doi.org/10.1182/blood-2018-07-861641 PMid:30266774
- Martínez
C, Khvedelidze I, Fekom M, Deau Fischer B, Marouf A, Ghesquières H,
Fornecker LM, Merli F, Stefani PM, Massaro F, Botto B, Ferhanoğlu B,
Akay OM, Özbalak M, Espeso de Haro M, Romero S, Galimard JE, Glass B,
Bazarbachi A, Sureda A. Outcomes of patients with Hodgkin lymphoma
receiving Brentuximab Vedotin (BV) as maintenance therapy after ASCT
according to previous exposure to BV. A retrospective analysis of the
EBMT Lymphoma Working Party in collaboration with GELTAMO, FIL, LYSA,
and Turkish Lymphoma Group. Bone Marrow Transplant. 2025;60:879-87. https://doi.org/10.1038/s41409-025-02568-4 PMid:40234724
- Herrera
AF, Chen L, Nieto Y, Holmberg L, Johnston P, Mei M, Popplewell L,
Armenian S, Cao T, Farol L, Sahebi F, Spielberger R, Chen R, Nademanee
A, Puverel S, Nwangwu M, Lee P, Song J, Skarbnik A, Kennedy N, Peters
L, Rosen ST, Kwak LW, Forman SJ, Feldman T. Brentuximab vedotin plus
nivolumab after autologous haematopoietic stem-cell transplantation for
adult patients with high-risk classic Hodgkin lymphoma: a multicentre,
phase 2 trial. Lancet Haematol. 2023;10:e14-e23. https://doi.org/10.1016/S2352-3026(22)00318-0 PMid:36403579
- Kersten
MJ, Driessen J, Zijlstra JM, Plattel WJ, Morschhauser F, Lugtenburg PJ,
Brice P, Hutchings M, Gastinne T, Liu R, Burggraaff CN, Nijland M,
Tonino SH, Arens AIJ, Valkema R, van Tinteren H, Lopez-Yurda M,
Diepstra A, De Jong D, Hagenbeek A. Combining brentuximab vedotin with
dexamethasone, high-dose cytarabine and cisplatin as salvage treatment
in relapsed or refractory Hodgkin lymphoma: the phase II HOVON/LLPC
Transplant BRaVE study. Haematologica. 2021;106:1129-1137. https://doi.org/10.3324/haematol.2019.243238 PMid:32273476 PMCid:PMC8018114
- Broccoli
A, Argnani L, Botto B, Corradini P, Pinto A, Re A, Vitolo U, Fanti S,
Stefoni V, Zinzani PL; Fondazione Italiana Linfomi ONLUS. First salvage
treatment with bendamustine and brentuximab vedotin in Hodgkin
lymphoma: a phase 2 study of the Fondazione Italiana Linfomi. Blood
Cancer J. 2019;9:100. https://doi.org/10.1038/s41408-019-0265-x PMid:31827067 PMCid:PMC6906387
- Garcia-Sanz
R, Sureda A, de la Cruz F, Canales M, Gonzalez AP, Pinana JL, Rodriguez
A, Gutierrez A, Domingo-Domenech E, Sanchez-Gonzalez B, Rodriguez G,
Lopez J, Moreno M, Rodriguez-Salazar MJ, Jimenez-Cabrera S, Caballero
MD, Martinez C. Brentuximab vedotin and ESHAP is highly effective as
second-line therapy for Hodgkin lymphoma patients (long-term results of
a trial by the Spanish GELTAMO Group). Ann Oncol. 2019;30:612-20. https://doi.org/10.1093/annonc/mdz009 PMid:30657848
- Advani
RH, Moskowitz AJ, Bartlett NL, Vose JM, Ramchandren R, Feldman TA,
LaCasce AS, Christian BA, Ansell SM, Moskowitz CH, Brown L, Zhang C,
Taft D, Ansari S, Sacchi M, Ho L, Herrera AF. Brentuximab vedotin in
combination with nivolumab in relapsed or refractory Hodgkin lymphoma:
3-year study results. Blood. 2021;138:427-38. https://doi.org/10.1182/blood.2020009178 PMid:33827139 PMCid:PMC11640334
- Moskowitz
AJ, Schöder H, Yahalom J, McCall SJ, Fox SY, Gerecitano J, Grewal R,
Hamlin PA, Horwitz S, Kobos R, Kumar A, Matasar M, Noy A, Palomba ML,
Perales MA, Portlock CS, Sauter C, Shukla N, Steinherz P, Straus D,
Trippett T, Younes A, Zelenetz A, Moskowitz CH. PET-adapted sequential
salvage therapy with brentuximab vedotin followed by augmented
ifosamide, carboplatin, and etoposide for patients with relapsed and
refractory Hodgkin's lymphoma: a non-randomised, open-label,
single-centre, phase 2 study. Lancet Oncol. 2015;16:284-92. https://doi.org/10.1016/S1470-2045(15)70013-6 PMid:25683846
- Cole
PD, McCarten KM, Pei Q, Spira M, Metzger ML, Drachtman RA, Horton TM,
Bush R, Blaney SM, Weigel BJ, Kelly KM. Brentuximab vedotin with
gemcitabine for paediatric and young adult patients with relapsed or
refractory Hodgkin's lymphoma (AHOD1221): a Children's Oncology Group,
multicentre single-arm, phase 1-2 trial. Lancet Oncol. 2018;19:1229-38.
https://doi.org/10.1016/S1470-2045(18)30426-1 PMid:30122620 PMCid:PMC6487196
- Stamatoullas
A, Ghesquières H, Feugier P, André M, Le Bras F, Gac AC, Borel C,
Gastinne T, Quittet P, Morschhauser F, Ribrag V, Guidez S,
Nicolas-Virelizier E, Berriolo-Riedinger A, Vander Borght T, Edeline V,
Brice P. Final results of brentuximab vedotin combined with
ifosfamide-carboplatin-etoposide in first refractory/relapsed Hodgkin
lymphoma: a lymphoma study association phase I/II study. Leuk Lymphoma.
2022;63:3063-71. https://doi.org/10.1080/10428194.2022.2107204 PMid:35975738
- LaCasce
AS, Bociek RG, Sawas A, Caimi P, Agura E, Matous J, Ansell SM,
Crosswell HE, Islas-Ohlmayer M, Behler C, Cheung E, Forero-Torres A,
Vose J, O'Connor OA, Josephson N, Wang Y, Advani R. Brentuximab vedotin
plus bendamustine: a highly active first salvage regimen for relapsed
or refractory Hodgkin lymphoma. Blood. 2018;132:40-8. https://doi.org/10.1182/blood-2017-11-815183 PMid:29703778 PMCid:PMC6073588
- Driessen
J, de Wit F, Herrera AF, Zinzani PL, LaCasce AS, Cole PD, Moskowitz CH,
García-Sanz R, Fuchs M, Müller H, Borchmann P, Santoro A, Schöder H,
Zijlstra JM, Hutten BA, Moskowitz AJ, Kersten MJ. Brentuximab vedotin
and chemotherapy in relapsed/refractory Hodgkin lymphoma: a propensity
score-matched analysis. Blood Adv. 2024;8:2740-52. https://doi.org/10.1182/bloodadvances.2023012145 PMid:38502227 PMCid:PMC11170165
- Cheson
BD, Ansell S, Schwartz L, Gordon LI, Advani R, Jacene HA, Hoos A,
Barrington SF, Armand P. Refinement of the Lugano Classification
lymphoma response criteria in the era of immunomodulatory therapy.
Blood. 2016;128:2489-96. https://doi.org/10.1182/blood-2016-05-718528 PMid:27574190
- Mei
MG, Lee HJ, Palmer JM, Chen R, Tsai NC, Chen L, McBride K, Smith DL,
Melgar I, Song JY, Bonjoc KJ, Armenian S, Nwangwu M, Lee PP, Zain J,
Nikolaenko L, Popplewell L, Nademanee A, Chaudhry A, Rosen S, Kwak L,
Forman SJ, Herrera AF. Response-adapted anti-PD-1-based salvage therapy
for Hodgkin lymphoma with nivolumab alone or in combination with ICE.
Blood. 2022;139:3605-16. https://doi.org/10.1182/blood.2022015423 PMid:35316328 PMCid:PMC9227101
- Mei
M, Palmer J, Lee HJ, Isufi I, Chen R, Tsai NC, Armenian S, Godfrey J,
Song JY, Baird JH, Thiruvengadam S, Samara Y, Flores J, Peters L, Rosen
S, Kwak L, Forman SJ, Herrera AF. Nivolumab plus ifosfamide,
carboplatin, and etoposide are a highly effective first salvage regimen
in high-risk relapsed/refractory Hodgkin lymphoma. Hemasphere.
2025;9:e70126. https://doi.org/10.1002/hem3.70126 PMid:40313510 PMCid:PMC12042211
- Moskowitz
AJ, Shah G, Schöder H, Ganesan N, Drill E, Hancock H, Davey T, Perez L,
Ryu S, Sohail S, Santarosa A, Galasso N, Neuman R, Liotta B, Blouin W,
Kumar A, Lahoud O, Batlevi CL, Hamlin P, Straus DJ, Rodriguez-Rivera I,
Owens C, Caron P, Intlekofer AM, Hamilton A, Horwitz SM, Falchi L,
Joffe E, Johnson W, Lee C, Palomba ML, Noy A, Matasar MJ, Pongas G,
Salles G, Vardhana S, Sanin BW, von Keudell G, Yahalom J, Dogan A,
Zelenetz AD, Moskowitz CH. Phase II Trial of Pembrolizumab Plus
Gemcitabine, Vinorelbine, and Liposomal Doxorubicin as Second-Line
Therapy for Relapsed or Refractory Classical Hodgkin Lymphoma. J Clin
Oncol. 2021;39:3109-17. https://doi.org/10.1200/JCO.21.01056 PMid:34170745 PMCid:PMC9851707
- Bryan
LJ, Casulo C, Allen PB, Smith SE, Savas H, Dillehay GL, Karmali R, Pro
B, Kane KL, Bazzi LA, Chmiel JS, Palmer BA, Mehta J, Gordon LI, Winter
JN. Pembrolizumab Added to Ifosfamide, Carboplatin, and Etoposide
Chemotherapy for Relapsed or Refractory Classic Hodgkin Lymphoma: A
Multi-institutional Phase 2 Investigator-Initiated Nonrandomized
Clinical Trial. JAMA Oncol. 2023;9:683-691. https://doi.org/10.1001/jamaoncol.2022.7975 PMid:36928527 PMCid:PMC10020934
- Desai
SH, Moskowitz AJ, Merryman RW, Shah H, Pederson LD, Geyer SM, Ganesan
N, Chang T, Othman T, Falade AS, Shah GL, Durani U, Sumransub N, Ng LS,
Baron K, Ong SY, Yoon K, Ansell SM, Armand P, Iyengar S, Micallef I,
Stuver R, Herrera AF, Mei M. PD-1-based combinations before autologous
transplant are associated with improved outcomes in classical Hodgkin
lymphoma. Blood. 2026;147:1125-34. https://doi.org/10.1182/blood.2025030151 PMid:41405496 PMCid:PMC13014084
- Spinner
MA, Sica RA, Tamaresis JS, Lu Y, Chang C, Lowsky R, Frank MJ, Johnston
LJ, Miklos DB, Muffly LS, Negrin RS, Rezvani AR, Shiraz P, Shizuru JA,
Weng WK, Binkley MS, Hoppe RT, Advani RH, Arai S. Improved outcomes for
relapsed/refractory Hodgkin lymphoma after autologous transplantation
in the era of novel agents. Blood. 2023;141:2727-37. https://doi.org/10.1182/blood.2022018827 PMid:36857637 PMCid:PMC13122320
- Kuruvilla
J, Ramchandren R, Santoro A, Paszkiewicz-Kozik E, Gasiorowski R,
Johnson NA, Fogliatto LM, Goncalves I, de Oliveira JSR, Buccheri V,
Perini GF, Goldschmidt N, Kriachok I, Dickinson M, Komarnicki M,
McDonald A, Ozcan M, Sekiguchi N, Zhu Y, Nahar A, Marinello P, Zinzani
PL; KEYNOTE-204 investigators. Pembrolizumab versus brentuximab vedotin
in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): an
interim analysis of a multicentre, randomised, open-label, phase 3
study. Lancet Oncol. 2021;22:512-24. https://doi.org/10.1016/S1470-2045(21)00005-X PMid:33721562
- Perales
MA, Awan FT, Boumendil A, Patel J, Castagna L, Angelucci E, Finel H,
Kulagin A, Glass B, Corradini P, Herrera AF, Blaise D, Kharfan-Dabaja
MA, Halahleh K, Ahmed S, Martínez C, Giebel S, Montoto S, Jones RJ,
Ahmed N, Lynch RC, De Lima MJ, Shadman M, Sauter CS, Ahn KW, Hamadani
M, Bazarbachi A, Sureda A. Outcomes of allogeneic HCT in Hodgkin
lymphoma in the era of checkpoint inhibitors: a joint CIBMTR and EBMT
analysis. Blood. 2025;146:1011-29. https://doi.org/10.1182/blood.2024027197 PMid:40623049
- Mariotti
J, Pinton C, Giordano L, Taurino D, Sarina B, De Philippis C, Mannina
D, Tentori C, Santoro A, Bramanti S. Reduced incidence of relapse after
checkpoint inhibitors relative to brentuximab vedotin as salvage
therapy before allogeneic stem cell transplantation for
refractory/relapsed Hodgkin lymphoma: A retrospective analysis. Br J
Haematol. 2025;207:1684-89. https://doi.org/10.1111/bjh.70091 PMid:40887735 PMCid:PMC12512095
- Tabbara
N, Zahurak M, Sterling CH, Trutzer IM, Jedrych J, Swinnen LJ, Fuchs EJ,
Bolaños-Meade J, Wagner-Johnston N, Jones RJ, Ambinder RF, Varadhan R,
Paul S. Improved overall survival with checkpoint inhibition and
allogeneic transplantation in relapsed Hodgkin lymphoma. Blood Adv.
2025;9:1202-09. https://doi.org/10.1182/bloodadvances.2024015048 PMid:39693511 PMCid:PMC11925506
- Ahmed
S, Kumar A, Carpenter P, Herrera A, Kelly K, Pinnix C, Rutherford S,
Grover N, Evens A, Lynch R, Kenkre V, Merryman R, Sauter C, Nishihori
T, Moskowitz A, Awan F, Svoboda J, Winter J, Allen P, Ermoian R, Ansell
S, Aljuhaishi T, Nieto Y, Hamadani M, Perales MA. American Society of
Transplantation and Cellular Therapy Clinical Practice Recommendations
for Transplantation in Classical Hodgkin Lymphoma. Transplant Cell
Ther. 2026;32:250-60. https://doi.org/10.1016/j.jtct.2025.12.944 PMid:41478324
- Reef
DK, Grover NS. Cellular and Novel Immunotherapies for Classic Hodgkin
Lymphoma. Hematol Oncol Clin North Am. 2026;40:303-19. https://doi.org/10.1016/j.hoc.2025.12.008 PMid:41667304
- Meng
F, Xiang M, Liu Y, Zeng D. Safety and efficacy of anti-CD30 CAR-T cell
therapy in relapsed/refractory classic Hodgkin lymphoma: a systematic
review and meta-analysis. BMC Cancer. 2025;25:78. https://doi.org/10.1186/s12885-024-13400-5 PMid:39806291 PMCid:PMC11731380
- Rothe
A, Sasse S, Topp MS, Eichenauer DA, Hummel H, Reiners KS, Dietlein M,
Kuhnert G, Kessler J, Buerkle C, Ravic M, Knackmuss S, Marschner JP,
Pogge von Strandmann E, Borchmann P, Engert A. A phase 1 study of the
bispecific anti-CD30/CD16A antibody construct AFM13 in patients with
relapsed or refractory Hodgkin lymphoma. Blood. 2015;125:4024-31. https://doi.org/10.1182/blood-2014-12-614636 PMid:25887777 PMCid:PMC4528081
- Sasse
S, Bröckelmann PJ, Momotow J, Plütschow A, Hüttmann A, Basara N,
Koenecke C, Martin S, Bentz M, Grosse-Thie C, Thorspecken S, de Wit M,
Kobe C, Dietlein M, Tresckow BV, Fuchs M, Borchmann P, Engert A. AFM13
in patients with relapsed or refractory classical Hodgkin lymphoma:
final results of an open-label, randomized, multicenter phase II trial.
Leuk Lymphoma. 2022;63:1871-78. https://doi.org/10.1080/10428194.2022.2095623 PMid:35848865
- Bartlett
NL, Herrera AF, Domingo-Domenech E, Mehta A, Forero-Torres A,
Garcia-Sanz R, Armand P, Devata S, Izquierdo AR, Lossos IS, Reeder C,
Sher T, Chen R, Schwarz SE, Alland L, Strassz A, Prier K, Choe-Juliak
C, Ansell SM. A phase 1b study of AFM13 in combination with
pembrolizumab in patients with relapsed or refractory Hodgkin lymphoma.
Blood. 2020;136:2401-9. https://doi.org/10.1182/blood.2019004701 PMid:32730586 PMCid:PMC7685206
- Nieto
Y, Banerjee P, Kaur I, Basar R, Li Y, Daher M, Rafei H, Kerbauy LN,
Kaplan M, Marin D, Griffin L, Barnett M, Bassett R, Uprety N, Shrestha
R, Silva FR, Islam S, Ganesh C, Borneo Z, Ramdial J, Ramirez A, Hosing
C, Alousi A, Popat U, Qazilbash M, Ahmed S, Iyer S, Sainz TP, Vega F,
Fowlkes NW, Alexis K, Emig M, Harstrick A, Overesch A, Shpall EJ,
Rezvani K. Allogeneic NK cells with a bispecific innate cell engager in
refractory relapsed lymphoma: a phase 1 trial. Nat Med.
2025;31:1987-93. https://doi.org/10.1038/s41591-025-03640-8 PMid:40186077 PMCid:PMC13218020
- Jakobsen
LH, Hutchings M, de Nully Brown P, Linderoth J, Mylam KJ, Molin D,
Johnsen HE, Bøgsted M, Jerkeman M, El-Galaly TC. No survival benefit
associated with routine surveillance imaging for Hodgkin lymphoma in
first remission: a Danish-Swedish population-based observational study.
Br J Haematol. 2016;173:236-44. https://doi.org/10.1111/bjh.13943 PMid:26846879
- van
Leeuwen FE, Ng AK. Long-term risk of second malignancy and
cardiovascular disease after Hodgkin lymphoma treatment. Hematology Am
Soc Hematol Educ Program. 2016;2016:323-30. https://doi.org/10.1182/asheducation-2016.1.323 PMid:27913498 PMCid:PMC6142518
- Camilli
M, Ballacci F, Lamendola P, Viscovo M, Tamburrini G, Tinti L, Torre I,
Amore L, Hohaus S, Crea F, Lanza GA, Burzotta F, Minotti G, Lombardo A.
Strain-derived myocardial work indices in adult cancer survivors:
results from an observational study and comparison with available
reference ranges. Cardiooncology. 2025;11:78. https://doi.org/10.1186/s40959-025-00373-y PMid:40885995 PMCid:PMC12398062
- Linee Guida Gestione dei pazienti adulti affetti da Linfoma di Hodgkin classico. Versione 3.2025. https://www.iss.it/-/lg-linfoma-hodgkin (published on September 3, 2025)