We report a case of late-onset, anicteric VOD/SOS following haploidentical HSCT, presenting in the setting of CMV reactivation.[3,4] A 20-year-old male with acute myeloid leukemia (AML, M4 subtype) achieved complete remission after induction and consolidation chemotherapy and subsequently underwent haploidentical HSCT from his sister. Conditioning consisted of busulfan, fludarabine, and cyclophosphamide, followed by post-transplant cyclophosphamide (PTCy). GVHD prophylaxis included mycophenolate mofetil and tacrolimus.
The early post-transplant course was uneventful, with neutrophil and platelet engraftment on days +12 and +14, respectively, and donor chimerism of 99% on day +21. On day +20, CMV reactivation was detected and ganciclovir was initiated. However, after one week of treatment, CMV viral load continued to increase from 2,332 copies/mL to 3,945 copies/mL and then 4,828 copies/mL, accompanied by worsening cytopenia. Antiviral therapy was therefore switched to foscarnet on day +30. By day +36, CMV viral load had decreased to 3,480 copies/mL.
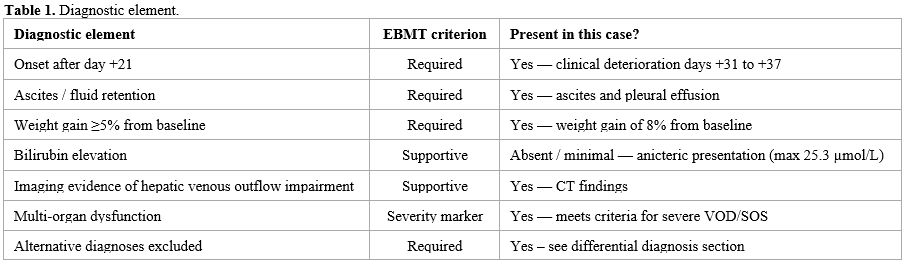
Between days +31 and +37, the patient developed rapidly progressive clinical deterioration. Liver enzymes increased markedly (AST up to 2,238 U/L and ALT up to 1,896 U/L), while total bilirubin remained relatively low (6.5–25.3 µmol/L; 0.38–1. 48 mg/dL), consistent with an anicteric pattern.[4] The patient also developed ascites, pleural effusion, weight gain of 8% from baseline and progressive cytopenia, with laboratory evidence of systemic inflammation and coagulopathy. His condition further deteriorated with multi-organ failure requiring intensive care support.
The differential diagnosis was broad, including CMV hepatitis, drug-induced liver injury, acute graft-versus-host disease (GVHD), sepsis-associated liver injury, thrombotic microangiopathy, hemophagocytic lymphohistiocytosis–like syndrome (HLH-like syndrome), ischemic hepatitis, and hepatic vascular thrombosis.[2]
CMV hepatitis was initially considered, given the documented viremia.[5] The CMV viral load showed a downward trend (from 4,828 to 3,480 copies/mL) after switching to foscarnet, while transaminases rose abruptly and markedly during the same period (AST up to 2,238 U/L, ALT up to 1,896 U/L). This temporal discordance between virological improvement and worsening hepatic injury argues strongly against CMV hepatitis as the primary cause. Tissue biopsy for CMV inclusion bodies was not feasible due to severe coagulopathy. Drug-induced liver injury was also considered, particularly in the context of exposure to conditioning agents and antiviral therapy. Ganciclovir was initiated on day +20 and switched to foscarnet on day +30. Tacrolimus levels were within the therapeutic range. However, the abrupt and severe increase in AST/ALT, together with the development of ascites and features suggestive of hepatic congestion, was not consistent with a typical drug-induced pattern. Acute hepatic GVHD was considered less likely in the absence of concurrent skin or gastrointestinal involvement and without a cholestatic pattern. Alkaline phosphatase and gamma-glutamyl transferase were only mildly elevated, further arguing against hepatic GVHD. Sepsis-associated liver injury was also considered, particularly in the setting of recurrent fever. However, blood cultures were negative. Hemodynamic instability was attributed to multi-organ failure in the context of VOD/SOS rather than septic shock. Procalcitonin levels ranged from 0.33 to 0.41 ng/mL, which was not consistent with significant bacterial sepsis. Broad-spectrum antibiotics were maintained without improvement in hepatic function. Thrombotic microangiopathy was also considered, but the peripheral blood smear showed no schistocytes. Haptoglobin was within normal limits. There were no features of hypertension or proteinuria. HLH-like syndrome was also evaluated: ferritin was markedly elevated (peak 16,196 ng/mL), and LDH was elevated (1,947 U/L), but triglycerides and fibrinogen (2.05 g/L) were not significantly abnormal, and the overall picture did not meet HLH-2004 criteria.
Given the inability to perform liver biopsy due to severe thrombocytopenia and coagulopathy, the diagnosis relied on clinical and imaging findings. In the context of rapid weight gain (8% from baseline), ascites, severe transaminase elevation, and progression to multi-organ failure, contrast-enhanced CT demonstrated hepatomegaly with diffuse, heterogeneous parenchymal enhancement, poor visualization and narrowing of the right and middle hepatic veins without macroscopic thrombosis, collapse of the inferior vena cava within the hepatic segment, and free abdominal fluid, findings consistent with hepatic venous outflow impairment.[6] Taken together, the clinical evolution, imaging findings, and exclusion of major alternative causes supported a diagnosis of severe late-onset anicteric VOD/SOS, in accordance with the revised European Society for Blood and Marrow Transplantation (EBMT) criteria.[3,7]
 |
|
Defibrotide therapy was initiated promptly, together with intensive supportive care, including high-flow oxygen therapy and drainage of pleural and abdominal fluid.[8,9] The patient showed gradual clinical improvement with resolution of organ dysfunction and was discharged on day +70. The clinical and biochemical response to defibrotide further supported the diagnosis of VOD/SOS. At 21 months of follow-up, he remains in complete remission, off immunosuppressive therapy, and has returned to normal daily activities.
This case highlights several important clinical points. First, VOD/SOS may occur beyond the early post-transplant period and present without hyperbilirubinemia, leading to underrecognition if classical diagnostic criteria are applied strictly.[3,4] Second, CMV reactivation served as a key diagnostic confounder rather than a proven causal factor, contributing to overlapping clinical manifestations and potentially delaying recognition of VOD/SOS.[5] Third, imaging findings can provide important supportive evidence of hepatic venous outflow impairment when invasive procedures are not feasible.[6] Late-onset VOD/SOS has been increasingly recognized in recent studies.[10]
In conclusion, late-onset, anicteric VOD/SOS should be considered in patients with persistent clinical deterioration after HSCT, even in the presence of CMV reactivation. Early recognition based on clinical suspicion and non-invasive imaging, followed by timely initiation of defibrotide, is essential to improve outcomes.[7]
Authors’ contributions
TTMN, TTN, VTT conceived the study. TTMN, TTN, VTT designed the study. TTMN participated in data collection and processing. TTMN participated in data analysis and interpretation. All authors participated in the literature search and wrote the manuscript. All authors have read and approved the final manuscript.Ethics approval and consent to participate
Written informed consent was obtained from the patient for publication of this case report.References
- Song Z, Han X, Zhou Z, et al. Comprehensive
management of hematopoietic stem cell transplantation complications:
from infection prevention to immune microenvironment reconstruction.
Front Immunol. 2026;17:1740067. https://doi.org/10.3389/fimmu.2026.1740067 PMid:41890754 PMCid:PMC13012925
- Bonifazi
F, Barbato F, Ravaioli F, Sessa M, Defrancesco I, Arpinati M, et al.
Diagnosis and treatment of veno-occlusive disease/sinusoidal
obstruction syndrome after allogeneic hematopoietic stem cell
transplantation. Front Immunol. 2020;11:489. https://doi.org/10.3389/fimmu.2020.00489 PMid:32318059 PMCid:PMC7147118
- Mohty
M, Malard F, Abecassis M, Aerts E, Alaskar AS, Aljurf M, et al. Revised
diagnosis and severity criteria for sinusoidal obstruction
syndrome/veno-occlusive disease in adult patients: a new classification
from the European Society for Blood and Marrow Transplantation. Bone
Marrow Transplant. 2016;51:906-912. https://doi.org/10.1038/bmt.2016.130 PMid:27183098 PMCid:PMC4935979
- Corbacioglu
S, Kernan NA, Pagliuca A, Ryan RJ, Tappe W, Richardson PG. Incidence of
anicteric veno-occlusive disease/sinusoidal obstruction syndrome and
outcomes with defibrotide following hematopoietic cell transplantation
in adult and pediatric patients. Biol Blood Marrow Transplant.
2020;26:1342-1349. https://doi.org/10.1016/j.bbmt.2020.03.011 PMid:32200121 PMCid:PMC8407521
- Limaye
AP, Babu TM, Boeckh M. Progress and challenges in the prevention,
diagnosis, and management of cytomegalovirus infection in
transplantation. Clin Microbiol Rev. 2020;34:e00043-19. https://doi.org/10.1128/CMR.00043-19 PMid:33115722 PMCid:PMC7920732
- Lee
SB, Lee S, Cho YJ, Choi YH, Cheon JE, Hong KT, et al. Shear wave
elastography and dispersion imaging for hepatic veno-occlusive disease
prediction after pediatric hematopoietic stem cell transplantation: a
feasibility study. Pediatr Radiol. 2024;54:1144-1155. https://doi.org/10.1007/s00247-024-05940-6 PMid:38772925 PMCid:PMC11182801
- Cairo
MS, Cooke KR, Lazarus HM, Chao N. Modified diagnostic criteria, grading
classification and newly elucidated pathophysiology of hepatic
sinusoidal obstruction syndrome/veno-occlusive disease after
hematopoietic cell transplantation. Br J Haematol. 2020;190:822-836. https://doi.org/10.1111/bjh.16557 PMid:32133623 PMCid:PMC7483983
- Castellino
A., Guidi S., Dellacasa C., Gozzini A., Donnini I., Nozzoli C., Manetta
S., Aydin S., Giaccone L., Festuccia M., Brunello L., Maffini E., Bruno
B., David E., Busca A.Late-onset hepatic veno-occlusive disease after
allografting: report of two cases with atypical clinical features
successfully treated with defibrotide.Mediterr J Hematol Infect Dis
2018, 10(1): e2018001, https://doi.org/10.4084/mjhid.2018.001 PMid:29326798 PMCid:PMC5760078
- Richardson
PG, Corbacioglu S. Veno-occlusive disease/sinusoidal obstruction
syndrome in patients: survival after defibrotide treatment. Blood
Cancer J. 2020;10:29. https://doi.org/10.1038/s41408-020-0286-5 PMid:32132522 PMCid:PMC7055222
- Mehra
V, Tetlow S, Choy A, de Lavallade H, Kulasekararaj A, Krishnamurthy P,
et al. Early and late-onset veno-occlusive disease/sinusoidal
obstruction syndrome post allogeneic stem cell transplantation: a
real-world experience. Am J Transplant. 2021;21:864-869. https://doi.org/10.1111/ajt.16345 PMid:33037770