A 17-year-old male with well-controlled bronchial asthma presented with one week of fever, reduced appetite, epigastric discomfort and early satiety. He later reported three days of painful penile and scrotal swelling. There was no history of trauma or recent sexual activity. On arrival, he was febrile and tachycardic, with marked splenomegaly. Genital examination showed diffuse tender penile and scrotal swelling.
Initial investigations showed total white cell count 323.81 x 10^9/L, haemoglobin 10.3 g/dL, platelet count 533 x 10^9/L, lactate dehydrogenase 828 U/L, uric acid 317 µmol/L, C-reactive protein 159.4 mg/L and procalcitonin 0.22 ng/mL. Differential count showed predominant neutrophilia with basophilia, and the peripheral blood film showed 1% blasts, in keeping with chronic-phase CML. The urology team initially considered stuttering priapism in the context of marked hyperleucocytosis, but true priapism was not objectively documented; the available clinical image did not demonstrate erection. Genital Doppler ultrasound instead demonstrated bilateral epididymo-orchitis and funiculitis with scrotal and penile cellulitis. Cytoreduction was commenced with high-dose hydroxyurea, allopurinol and intravenous hydration.
On day 4 of admission, haemopurulent discharge appeared from the left dorsum of the penile shaft. Incision and drainage identified a discharging sinus over the left dorsum of the penile shaft, with necrotic material and pus extending from the root of the penis into the left hemiscrotum (Figure 1). Both blood cultures and intraoperative specimens yielded non-typhoidal Salmonella, subsequently serotyped as S. enteritidis. He denied consumption of raw or undercooked food, including uncooked meat and raw eggs. Abdominal ultrasound showed no intra-abdominal collection.
 |
|
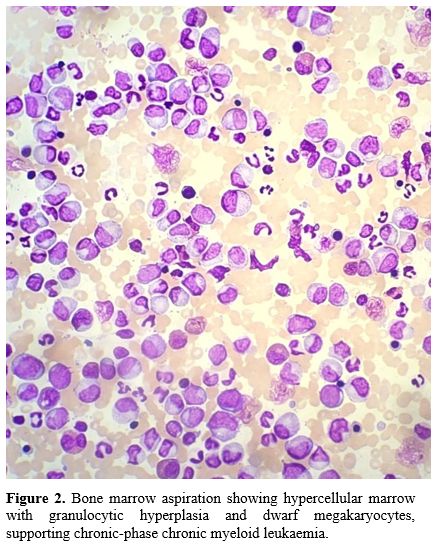
He improved after drainage and targeted antimicrobial therapy. Following two weeks of intravenous ceftriaxone, he received a further four weeks of oral sulfamethoxazole/trimethoprim as eradication therapy after infectious disease consultation. Bone marrow aspiration and trephine biopsy showed hypercellular marrow with granulocytic hyperplasia and dwarf megakaryocytes, and the major BCR::ABL1 fusion transcript was detected, confirming chronic-phase CML (Figure 2). He was subsequently commenced on nilotinib. His wounds healed well, splenomegaly resolved, and penile function was preserved.
 |
|
The main interpretative issue is the relationship between chronic-phase CML, hyperleucocytosis and focal Salmonella infection. Priapism in CML is attributed to hyperviscosity and leucostasis, causing impaired venous outflow and microvascular obstruction within the corpora cavernosa.[3] In this patient, however, the initial concern for priapism was not objectively confirmed, and subsequent imaging and operative findings supported cellulitis, epididymo-orchitis/funiculitis and evolving abscess. It is therefore more appropriate to interpret the abscess as probable haematogenous seeding of inflamed or locally compromised genital tissue during S. enteritidis bacteraemia. Marked hyperleucocytosis-related microvascular dysfunction may have contributed to local tissue susceptibility, but this remains a plausible mechanism rather than a proven causal pathway.
This case should also be distinguished from the more familiar pattern of genital necrotising infection in acute leukaemias. Fournier’s gangrene has been repeatedly described in patients with oncohaematological diseases, particularly in the setting of acute leukaemias, profound neutropenia, intensive chemotherapy or disease-related immunosuppression.[4] Genital ulceration has also been reported during all-trans retinoic acid therapy for acute promyelocytic leukaemia.[5] In contrast, genital infection in chronic-phase CML appears exceptional. The present case is therefore not best framed as typical leukaemia-associated Fournier’s syndrome, but as a rare microbiologically documented S. enteritidis penile abscess occurring in the setting of newly diagnosed chronic-phase CML.
Non-typhoidal Salmonella usually causes self-limiting gastroenteritis, but bacteraemia and focal extraintestinal infection can occur, particularly when host or tissue factors permit bacterial seeding.[6,7] Any anatomical site may theoretically be seeded during bacteraemia, although focal abscess formation remains uncommon.[6] The concordant recovery of non-typhoidal Salmonella from both blood and operative specimens gives this case stronger microbiological credibility than anecdotal abscess reports based on a single culture source.
Conclusions
We describe a rare, microbiologically confirmed penile abscess caused by S. enteritidis in an adolescent with newly diagnosed chronic-phase CML. The case is best interpreted as S. enteritidis bacteraemia with probable haematogenous seeding of locally inflamed or compromised genital tissue, rather than as a typical leukaemia-associated Fournier’s syndrome or as direct evidence that chronic-phase CML causes severe bacterial immunosuppression. Early surgical drainage, targeted antimicrobial therapy and coordinated urology, infectious disease and haematology input were central to the favourable outcome.Consent for publication
Written informed consent was obtained from the patient and his legal guardian for publication of the case details and clinical images. Given the sensitive anatomical site, the genital photographs were included only after careful consideration of their clinical relevance. The images were selected to show essential diagnostic findings, were anonymised as far as possible, and contain no facial features or direct personal identifiers. The authors acknowledge that final inclusion of these images remains subject to editorial assessment of necessity, anonymisation and publication suitability.Acknowledgements
The authors thank the urology, infectious disease, haematology, pathology and nursing teams involved in the patient's care.References
- Jabbour E, Kantarjian H. Chronic myeloid leukemia:
2018 update on diagnosis, therapy and monitoring. Am J Hematol.
2018;93(3):442-459. https://doi.org/10.1002/ajh.25011 PMid:29411417
- Breccia
M, Girmenia C, Latagliata R, Loglisci G, Santopietro M, Federico V, et
al. Low incidence rate of opportunistic and viral infections during
imatinib treatment in chronic myeloid leukemia patients in early and
late chronic phase. Mediterr J Hematol Infect Dis. 2011;3(1):e2011021. https://doi.org/10.4084/mjhid.2011.021 PMid:21713076 PMCid:PMC3113277
- Ali
E, Soliman A, De Sanctis V, Nussbaumer D, Yassin M. Priapism in
patients with chronic myeloid leukemia (CML): a systematic review. Acta
Biomed. 2021;92(3):e2021193.
- Creta
M, Sica A, Napolitano L, Celentano G, La Rocca R, Capece M, et al.
Fournier's gangrene in patients with oncohematological diseases: a
systematic review of published cases. Healthcare (Basel).
2021;9(9):1123. https://doi.org/10.3390/healthcare9091123 PMid:34574898 PMCid:PMC8469850
- Yavasoglu
I, Unubol M, Sargin G, Kadikoylu G, Bolaman Z. Penile ulcer ATRA
related in patient with acute promyelocytic leukemia. Mediterr J
Hematol Infect Dis. 2012;4(1):e2012054. https://doi.org/10.4084/mjhid.2012.054 PMid:22973498 PMCid:PMC3435123
- Acheson D, Hohmann EL. Nontyphoidal salmonellosis. Clin Infect Dis. 2001;32(2):263-269. https://doi.org/10.1086/318457 PMid:11170916
- Zhou H, Jia C, Cao Q, Huang L, Teng L, Wang Z, et al. Invasive non-typhoidal Salmonella infections in China (1961-2024): a retrospective systematic analysis of multicentre case reports. J Glob Health. 2026;16:04008. https://doi.org/10.7189/jogh.16.04008 PMid:41524234 PMCid:PMC12796866