 |
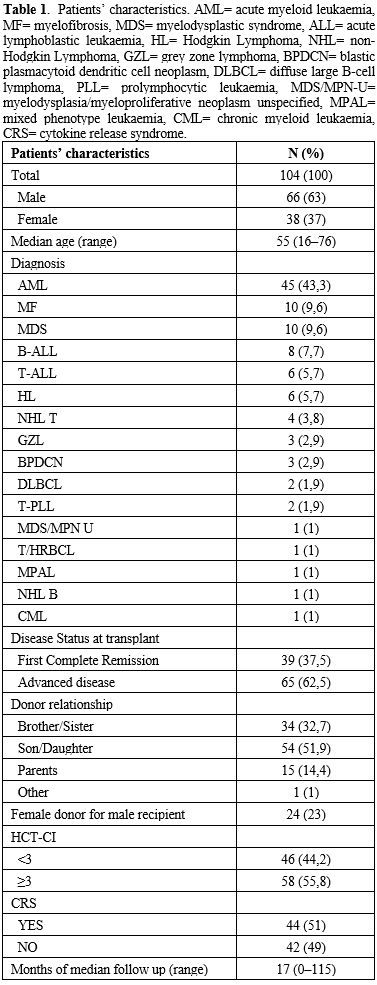
Table 1.
Patients’ characteristics. AML= acute myeloid leukaemia, MF=
myelofibrosis, MDS= myelodysplastic syndrome, ALL= acute lymphoblastic
leukaemia, HL= Hodgkin Lymphoma, NHL= non-Hodgkin Lymphoma, GZL= grey
zone lymphoma, BPDCN= blastic plasmacytoid dendritic cell neoplasm,
DLBCL= diffuse large B-cell lymphoma, PLL= prolymphocytic leukaemia,
MDS/MPN-U= myelodysplasia/myeloproliferative neoplasm unspecified,
MPAL= mixed phenotype leukaemia, CML= chronic myeloid leukaemia, CRS=
cytokine release syndrome. |
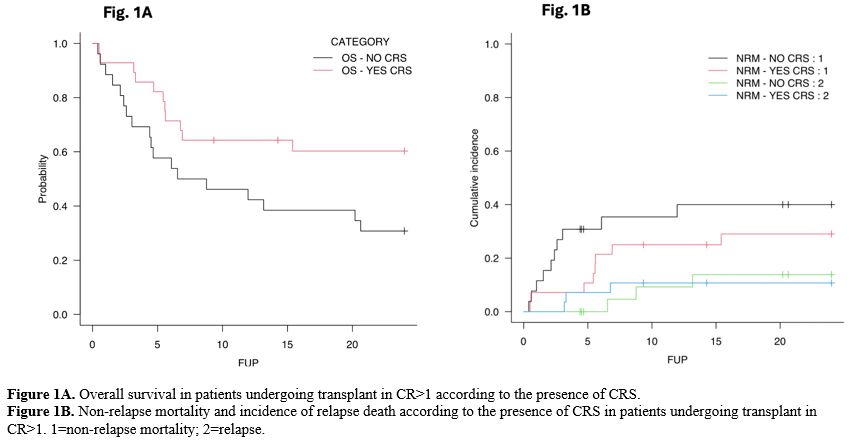 |
Figure 1A. Overall survival in patients undergoing transplant in CR>1 according to the presence of CRS. Figure 1B. Non-relapse mortality and incidence of relapse death according to the presence of CRS in patients undergoing transplant in CR>1. 1=non-relapse mortality; 2=relapse. |
Notably, no patients received specific treatment for CRS, and clinical manifestations resolved after post-transplant cyclophosphamide administration. This observation supports the hypothesis that CRS in this setting is driven by early alloimmune activation, subsequently modulated by PTCy, as suggested by other groups.[9-11]
This study has several limitations, including its retrospective design, single-center setting, and limited sample size, particularly for subgroup analyses. In addition, the cohort was heterogeneous and included different hematologic malignancies with distinct relapse risks and potentially different sensitivities to graft-versus-leukemia effects. The relatively small number of severe CRS cases also precluded a meaningful analysis according to CRS grade. Finally, the exclusion of patients with early documented infections, although intended to improve diagnostic specificity for CRS, may have introduced selection bias. In conclusion, CRS after haplo-HSCT was associated with improved survival in patients with advanced disease, without evidence of increased TRM. These findings suggest that CRS may reflect early alloimmune activation after transplantation; however, the retrospective design, limited sample size, and cohort heterogeneity preclude definitive conclusions regarding a graft-versus-tumor effect. Larger prospective studies are needed to validate these observations.
References
- Abboud, R. et al. Cytokine release syndrome after
haploidentical hematopoietic cell transplantation: an international
multicenter analysis. Bone Marrow Transplant 56, 2763-2770 (2021). https://doi.org/10.1038/s41409-021-01403-w PMid:34262142
- McCurdy,
S. R. et al. Early Fever after Haploidentical Bone Marrow
Transplantation Correlates with Class II HLA-Mismatching and
Myeloablation but Not Outcomes. Biol Blood Marrow Transplant 24,
2056-2064 (2018). https://doi.org/10.1016/j.bbmt.2018.06.004 PMid:29909152 PMCid:PMC6385878
- Modi,
D. et al. Grade 3-4 cytokine release syndrome is associated with poor
survival in haploidentical peripheral blood stem cell transplantation.
Leuk Lymphoma 62, 1982-1989 (2021). https://doi.org/10.1080/10428194.2021.1891231 PMid:33627028
- Wachsmuth,
L. P. et al. Posttransplantation cyclophosphamide prevents
graft-versus-host disease by inducing alloreactive T cell dysfunction
and suppression. J Clin Invest 129, 2357-2373. https://doi.org/10.1172/JCI124218 PMid:30913039 PMCid:PMC6546453
- McCurdy,
S. R. & Luznik, L. How we perform haploidentical stem cell
transplantation with posttransplant cyclophosphamide. Blood 134,
1802-1810 (2019). https://doi.org/10.1182/blood.2019001323 PMid:31751485 PMCid:PMC6872960
- Avenoso,
D. et al. Haploidentical Transplant with Post-Transplant
Cyclophosphamide for Acute Myeloid Leukaemia and Myelodysplastic
Syndromes Patients: The Role of Previous Lines of Therapy. Mediterr J
Hematol Infect Dis 16, e2024002 (2024). https://doi.org/10.4084/MJHID.2024.002 PMid:38223487 PMCid:PMC10786144
- Lee,
D. W. et al. ASTCT Consensus Grading for Cytokine Release Syndrome and
Neurologic Toxicity Associated with Immune Effector Cells-NC-ND
license. (http://creativecommons.org/licenses/by-nc-nd/4.0/). Biology
of Blood and Marrow Transplantation 25, 625-638 (2019). https://doi.org/10.1016/j.bbmt.2018.12.758 PMid:30592986 PMCid:PMC12180426
- Shapiro,
R. M. et al. Cytokine release syndrome in haploidentical stem cell
transplant may impact T-cell recovery and relapse. Blood Adv 7,
4080-4088 (2023). https://doi.org/10.1182/bloodadvances.2023009657 PMid:37216223 PMCid:PMC10388727
- Benavente,
R. et al. Cytokine release syndrome: implications for transplant
outcomes in haploidentical and HLA-matched HSCT using PTCy. Bone Marrow
Transplant 60, 1020-1026 (2025). https://doi.org/10.1038/s41409-025-02594-2 PMid:40269279
- Kitamura,
W. et al. Feasibility of early tacrolimus initiation in
haploidentical-PBSCT with post-transplant cyclophosphamide after
melphalan-based conditioning regimen. Blood Cell Ther 8, 262-267
(2025). https://doi.org/10.31547/bct-2025-013 PMid:41368186 PMCid:PMC12682609
- Koh,
J. S. et al. Post-transplant cyclophosphamide plus anti-thymocyte
globulin decreased serum IL-6 levels when compared with post-transplant
cyclophosphamide alone after haploidentical hematopoietic stem cell
transplantation. Blood Res 60, 5 (2025).
https://doi.org/10.1007/s44313-024-00049-z PMid:39812969 PMCid:PMC11735700