A 54-year-old man of Albanian ethnicity, with no significant past history, presented in January 2026 with a one-month history of progressive thoracic, rib, and lumbar pain unresponsive to over-the-counter analgesics. There was no fever, weight loss, trauma, or family history of haematological disease. Examination revealed tenderness over the lower thoracic spine and the left hemithorax, with no lymphadenopathy, organomegaly, or neurological deficit.
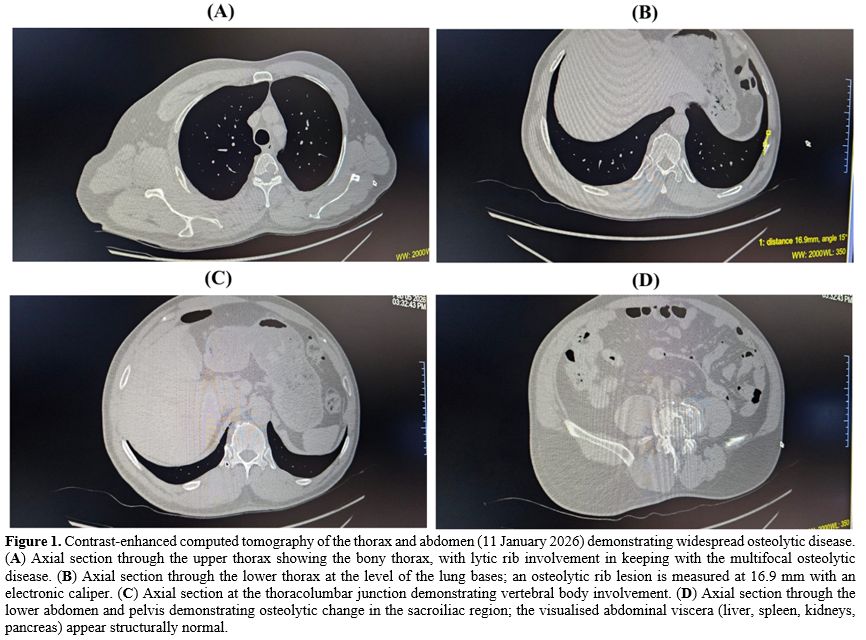
A contrast-enhanced computed tomography (CT) scan of the thorax and abdomen (11 January 2026) demonstrated multiple osteolytic lesions, including the anterior arc of the 9th and 10th left ribs (largest 20 × 10 mm), the posterior arc of the 10th left rib and the 12th right rib, additional millimetric lesions in the 4th to 8th right ribs, a 15 mm lesion in the 4th thoracic vertebral body, a cervical 6 vertebral body lesion, and destructive changes in the posterior body of L4 and the anterior wall of L5 with disc involvement at L4 to L5 (Figure 1). No pulmonary, pleural, pericardial, lymph node, or visceral organ abnormality was identified.
 |
|
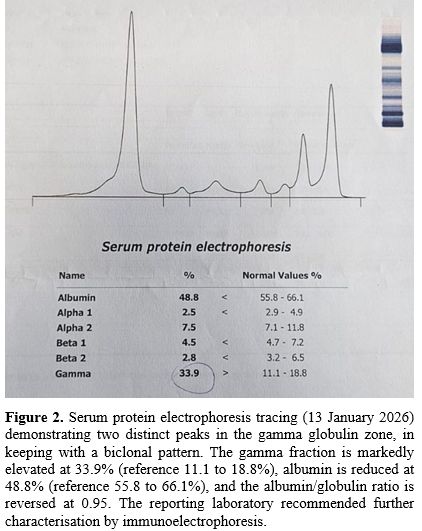
Initial laboratory workup (13 January 2026) showed haemoglobin 15.3 g/dL, white cell count 11.5 × 10⁹/L, platelets 225 × 10⁹/L, preserved renal function (creatinine 0.99 mg/dL), and normal calcium and lactate dehydrogenase. SPEP demonstrated two distinct peaks in the gamma globulin zone, with the gamma fraction markedly elevated at 33.9% (reference 11.1 to 18.8%), albumin reduced at 48.8% (reference 55.8 to 66.1%), and an albumin/globulin ratio of 0.95 (Figure 2). The reporting laboratory described the tracing as a biclonal pattern in the gamma globulin zone, with each peak likely representing a different immunoglobulin type, and recommended further characterisation by immunoelectrophoresis. Immunofixation electrophoresis was not available locally, and the two bands could not be characterised as heavy- or light-chain classes. Quantitative serum immunoglobulins showed markedly elevated IgG (3251 mg/dL; reference 700 to 1600), with severe immunoparesis of IgM (20.1 mg/dL; reference 40 to 230) and IgA (29.3 mg/dL; reference 70 to 400). Serum free light chain analysis at the local laboratory reported kappa at 982 mg/dL and lambda at 61 mg/dL, yielding a markedly abnormal kappa/lambda ratio of 16.0. The absolute values and the local reference ranges reported by the laboratory differ from those of the standard nephelometric or turbidimetric Freelite assays, in which serum free light chains are conventionally reported in mg/L. The qualitative finding of a markedly abnormal kappa/lambda ratio is internally consistent with the rest of the workup, but standardised Freelite values were not obtainable in our setting, and the absolute values should be interpreted with caution. Beta-2 microglobulin was 2.14 mg/L and serum albumin 4.2 g/dL, placing the patient in International Staging System stage I.[2]
 |
|
The patient was admitted to the Department of Haematology of Spitali Rajonal Durres. Bone marrow aspiration was performed from a posterior iliac crest site. The specimen was hemodilute, with only 2% plasma cells on the myelogram differential, a predominance of peripheral blood elements on flow cytometric immunophenotyping (lymphoid 41%, granulocytic 53%, monocytes 5%, erythroid 1%), and no aberrant plasma cell population detectable in the submitted sample. A bone marrow trephine biopsy from the standard posterior iliac crest site was not performed locally. Given the marked discordance between the aspirate findings and the clinical, radiological, and laboratory picture, CT-guided core biopsy of an accessible lytic rib lesion was pursued. At Spitali Katolik "Zoja e Këshillit të Mirë" in Tirana, two 14-gauge cores were obtained from the lytic lesion of the 10th left rib (10 February 2026). Histopathology showed diffuse infiltrative proliferation of atypical plasma cells, with immunohistochemistry positive for CD38 (3+), CD138 (3+), and kappa light chain (3+), and minimal lambda expression, supporting plasma cell infiltration with kappa light chain restriction.
The patient was started on daratumumab, bortezomib, cyclophosphamide, and dexamethasone (Dara-VCd), together with zoledronic acid for bone protection. Daratumumab-based induction with a proteasome inhibitor is the current standard of care for newly diagnosed transplant-eligible patients, and the choice of alkylator or immunomodulator backbone depends on local practice and access.[3,4] Lenalidomide was not readily accessible through the local reimbursement framework, and cyclophosphamide was substituted as the alkylator backbone, preserving the daratumumab and bortezomib activity. Autologous stem cell transplantation will be considered after first-line induction. Treatment was tolerated without major toxicity, and post-induction response assessment was pending at the time of manuscript preparation.
This case highlights two clinical points. The first, and the central diagnostic message, is that image-guided biopsy of an accessible osteolytic lesion can resolve the diagnosis of multiple myeloma when the standard marrow aspirate is non-representative. Our patient had overt myeloma on all other axes, with widespread osteolytic disease on imaging, marked elevation of IgG, severe immunoparesis of the uninvolved immunoglobulins, a biclonal SPEP pattern, and a markedly abnormal kappa/lambda ratio. Yet the bone marrow aspirate from the posterior iliac crest showed only 2% plasma cells. The most likely explanation is hemodilution of the aspirate, supported by the flow cytometric predominance of peripheral blood elements over marrow precursors. In patients with focal involvement or technically limited samples, aspirate plasma cell counts may underestimate disease burden, and the International Myeloma Working Group criteria allow a diagnosis of multiple myeloma when biopsy-proven plasmacytoma coexists with myeloma-defining events, even if the marrow plasma cell fraction is below 10%.[1] In this patient, osteolytic bone disease fulfilled the bone disease criterion, and the CT-guided rib biopsy provided the decisive histopathological evidence.
The second point concerns the SPEP pattern, and is more limited in scope. Biclonal gammopathies, defined by two distinct monoclonal protein bands on SPEP or immunofixation, are uncommon overall and heterogeneous in their biological basis.[5,6] The two species may differ by heavy chain, light chain, or both. In our patient, we are not in a position to make a precise biological claim about the two SPEP peaks, and the present report should be read with that limit in mind. Without immunofixation or immunoelectrophoresis, we cannot say whether the two abnormal bands reflect two independent plasma cell clones each producing its own monoclonal immunoglobulin, or a single clone producing more than one monoclonal protein, or one true monoclonal band accompanied by an additional component. The kappa restriction observed on the rib biopsy is consistent with at least one kappa-restricted clone but does not exclude the alternative interpretations, particularly in the absence of parallel flow cytometric and molecular characterisation of the plasma cell population. The patient therefore has a histologically confirmed multiple myeloma associated with a biclonal pattern on SPEP, rather than a fully characterised biclonal multiple myeloma in the biological sense.
Several substantive limitations should be acknowledged. Immunofixation electrophoresis and immunoelectrophoresis were not available locally, so the two M-protein species could not be characterised by heavy or light chain class. Bone marrow trephine biopsy from the standard posterior iliac crest site was not performed, which could have shown a higher plasma cell fraction than the hemodilute aspirate, would have allowed structured assessment of marrow architecture, and would have provided tissue for full plasma cell immunophenotyping by flow cytometry and immunohistochemistry. Comprehensive plasma cell immunophenotyping, including CD19, CD45, CD56, CD117, and clonality markers, was not performed. Cytogenetic studies, including interphase fluorescence in situ hybridisation for high-risk markers such as del(17p), t(4;14), t(14;16), gain(1q), and del(1p), were not available, and the Revised International Staging System could not be assigned, nor could the current risk-adapted staging be completed.[7] Molecular studies, including the assessment of high-risk lesions now recognised in contemporary risk stratification, were not performed.[8] The absolute values of the local serum free light chain assay differ in units, and reference ranges from those of the standard Freelite assay; the absolute values should be interpreted with caution. The clinically informative finding is the qualitative ratio, supported by convergent evidence from quantitative immunoglobulins, histological kappa restriction, and radiological evidence of bone disease. These limitations are substantive rather than technical, and they constrain the biological interpretation of the case while leaving the central clinical message intact.
In summary, this brief report supports two practical points. When a bone marrow aspirate is hemodilute and clearly discordant with the overall clinical, radiological, and laboratory picture, biopsy of an accessible focal lytic lesion may provide the decisive diagnostic evidence. When a biclonal SPEP pattern is encountered without immunofixation, immunoelectrophoresis, full plasma cell immunophenotyping, and cytogenetic and molecular characterisation, the biological interpretation of the two bands should remain cautious. In resource-constrained settings, the diagnostic pathway can be constructed around what is available, but the limitations should be acknowledged in proportion to their substantive significance. Recent reviews on multiple myeloma diagnosis, risk stratification, and first-line therapy provide a useful framework for situating individual cases within current practice.[3,8,9,10]
Acknowledgments
The authors thank the radiology and pathology teams of Spitali Katolik "Zoja e Këshillit të Mirë" in Tirana for the CT-guided rib biopsy and histopathological analysis, and the laboratory and clinical teams of the contributing institutions for their support during this patient’s diagnostic workup. The authors are grateful to the patient for granting permission to publish this case in the hope that it will inform the care of similar patients.Authors' Contributions
AC was the primary inpatient haematologist responsible for clinical care at Spitali Rajonal Durres, supervised the bone marrow examination and laboratory workup, and contributed to the manuscript draft and revision. LS conceived the case report, collected the clinical and radiological data, performed the literature review, and drafted the manuscript. SQ contributed to the CT-guided rib biopsy workflow at Spitali Katolik "Zoja e Këshillit të Mirë", provided clinical and editorial input, and reviewed the manuscript. All authors read and approved the final version.Ethics Approval and Consent
This case report was prepared in accordance with the principles of the Declaration of Helsinki and institutional guidelines. Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.References
- Rajkumar SV, Dimopoulos
MA, Palumbo A, Blade J,
Merlini G, Mateos MV, et al. International Myeloma Working Group
updated criteria for the diagnosis of multiple myeloma. Lancet Oncol.
2014;15:e538-e548. https://doi.org/10.1016/S1470-2045(14)70442-5
PMid:25439696
- Greipp
PR, San Miguel J, Durie BG, Crowley JJ, Barlogie B, Bladé J, et al.
International staging system for multiple myeloma. J Clin Oncol.
2005;23:3412-3420. https://doi.org/10.1200/JCO.2005.04.242
PMid:15809451
- Houbaida
Y, Del Giudice ML, Galimberti S, Buda G. How first-line therapy is
changing in transplant-eligible multiple myeloma patients. Mediterr J
Hematol Infect Dis. 2025;17:e2025026. doi:10.4084/MJHID.2025.026. https://doi.org/10.4084/MJHID.2025.026
PMid:40084095 PMCid:PMC11906123
- Voorhees
PM, Kaufman JL, Laubach J, Sborov DW, Reeves B, Rodriguez C, et al.
Daratumumab, lenalidomide, bortezomib, and dexamethasone for
transplant-eligible newly diagnosed multiple myeloma: the GRIFFIN
trial. Blood. 2020;136:936-945. https://doi.org/10.1182/blood.2020005288
PMid:32325490 PMCid:PMC7441167
- Kyle
RA, Robinson RA, Katzmann JA. The clinical aspects of biclonal
gammopathies: review of 57 cases. Am J Med. 1981;71:999-1008. https://doi.org/10.1016/0002-9343(81)90326-0
PMid:6797297
- Mullikin
TC, Rajkumar SV, Dispenzieri A, Buadi FK, Lacy MQ, Lin Y, et al.
Clinical characteristics and outcomes in biclonal gammopathies. Am J
Hematol. 2016;91:473-475. https://doi.org/10.1002/ajh.24319
PMid:26840395 PMCid:PMC5780647
- Palumbo
A, Avet-Loiseau H, Oliva S, Lokhorst HM, Goldschmidt H, Rosinol L, et
al. Revised International Staging System for multiple myeloma: a report
from International Myeloma Working Group. J Clin Oncol.
2015;33:2863-2869. https://doi.org/10.1200/JCO.2015.61.2267
PMid:26240224 PMCid:PMC4846284
- Martino
EA, Mele G, Morabito F, Gentile M, Vigna E. Refining high-risk multiple
myeloma: advancements in genomic, clinical, and prognostic criteria.
Mediterr J Hematol Infect Dis. 2025;17:e2025006.
doi:10.4084/MJHID.2025.006. https://doi.org/10.4084/MJHID.2025.006
PMid:39830800 PMCid:PMC11740893
- Morè
S, Corvatta L, Manieri VM, Morsia E, Poloni A, Offidani M. Novelties on
multiple myeloma from the main 2024 hematology conferences. Mediterr J
Hematol Infect Dis. 2025;17:e2025027. doi:10.4084/MJHID.2025.027. https://doi.org/10.4084/MJHID.2025.027
PMid:40084104 PMCid:PMC11906126
- Dimopoulos MA, Moreau P, Terpos E, Mateos MV, Zweegman S, Cook G, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32:309-322. https://doi.org/10.1016/j.annonc.2020.11.014 PMid:33549387